The MMR vaccine: Public health, private fears
Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Tuesday, 9 June 2026, 12:27 PM
The MMR vaccine: Public health, private fears
Introduction
The MMR dispute is of enormous public significance and this course helps unravel why this has been an area of such dispute.
This OpenLearn course provides a sample of postgraduate study in Science.
Learning outcomes
After studying this course, you should be able to:
understand more of the scientific factors that relate to the dispute about the safety of the MMR vaccine in the UK
assess the strength of arguments for and against the use of the MMR vaccine
show how issues of risk, trust, communication and media representation of science and medicine have a strong bearing on public perception of the MMR vaccine
explain why there is such a strong consensus amongst the medical profession testifying to the safety of the MMR vaccine.
1 The MMR controversy
The furore over the measles, mumps and rubella (MMR) vaccination has rapidly escalated into a landmark controversy in the UK. Since the suggestion in 1998 by Dr Andrew Wakefield that MMR might be implicated as a cause of autism, a steady stream of claim and counterclaim has been played out in the scientific press, and newspaper headlines have see-sawed between condemnation and commendation (see the chronicle of events outlined in Box 1). More generally, the MMR debate illustrates that public health programmes are frequently underpinned by a strong ‘reliance on science’, which may not be an effective persuasive strategy for its target audience. Instead, this course will show that the public have witnessed an element of dissent within the scientific and medical establishments. Furthermore, the political and scientific management of this conflict, and a reluctance to acknowledge the social context within which it has arisen, have given the debate a longevity and potency perhaps far beyond that which the scientific arguments themselves warrant.
MMR vaccine consists of a freeze-dried preparation of live but weakened (attenuated) virus particles, intended to provoke recognition of the measles, mumps and rubella viruses by the body's immune system but not cause any symptoms of the diseases themselves. The vaccine is usually given in two doses, both by injection. The first dose is given to babies aged 12–15 months, and the second (a ‘booster’) is given at school age, intended to protect those children (about 5–10%) that did not respond to the first dose. The triple vaccination programme was introduced in the UK in 1988. It replaced the single vaccine given to babies for measles and a vaccination for rubella given to teenage girls. Mumps was not previously widely vaccinated against.
In this course, we'll explore why the MMR controversy has loomed so large in public consciousness. We'll have a look at the effects of media coverage, and see how social factors are inextricable from science when it comes to assessing risk. Like many other parents of young children, I have had to take a difficult decision about whether or not to trust the MMR vaccine. The scientific consensus is almost unanimous against an association between MMR and autism, so why do parents agonise about it? Is this a symptom of wider public anxiety about scientific pronouncements on public health, and is this uneasiness justified?
Box 1 Chronicle of some of the main events in the MMR controversy
| October 1988 | The MMR vaccine replaces single vaccines for measles and rubella in the UK. |
| April 1993 | Andrew Wakefield claims to have established a link between measles and Crohn's disease (an intestinal disorder), but further studies could not confirm this. |
| 28 February 1998 | Wakefield and 12 co-authors publish an early report in The Lancet showing intestinal inflammation in 12 children with developmental disorders. Wakefield announces his concern about links between MMR and autism at a press conference. |
| 23 March 1998 | Meeting of 37 experts by Medical Research Council reviews published and unpublished evidence and concludes there is no link between MMR and autism. |
| 2 May 1998 | Finnish study published in which reported adverse reactions to the MMR vaccine between 1988 and 1996 revealed no association between MMR and autism. |
| 12 June 1999 | Epidemiological study of 498 cases of autism in eight North Thames health districts finds that there was no sudden step-up increase in diagnoses after the introduction of MMR in 1998 and no developmental regression clustered after vaccination. |
| 6 April 2000 | Wakefield testifies in support of his MMR–autism hypothesis to a US Congressional Hearing. |
| December 2000 | Wakefield publishes a paper entitled ‘MMR vaccine: through a glass, darkly’, criticising safety procedures when MMR was first introduced. |
| 21 January 2001 | Wakefield discloses to the Telegraph that he has seen 170 cases of ‘a new syndrome of autism’, with the majority of cases backed by documentary evidence of regression following vaccination. He claims that regulators have failed to adequately address safety of the MMR vaccine. |
| March 2001 | Department of Health drops advertising campaign to promote MMR in the face of criticism that the money would be better spent on research into autism. |
| 9 June 2001 | Lothian division of the British Medical Association (BMA) requests the BMA to back single vaccines as an alternative for parents who refuse the MMR. |
| 30 November 2001 | Wakefield ‘asked to resign’ from Royal Free Hospital. |
| 13 December 2001 | Review by Medical Research Council into autism finds that the number of cases has increased (6 in 1000 children), but this is largely due to increased recognition and changing definitions of autism. The report finds no evidence of a link with MMR. |
| 19 December 2001 | During Prime Minister's Questions, MP Julie Kirkbride asks Mr Blair whether his son Leo had been immunised with MMR. Mr Blair declines to answer on privacy grounds. |
| 3 February 2002 | BBC TV Panorama special presents a largely sympathetic account of Wakefield's hypothesis. Wakefield claims that research has found measles in the guts of 75 of 91 autistic children with bowel disease. |
| 19 June 2002 | Wakefield presents evidence to a US congressional committee claiming that the measles virus identified in the guts of autistic children had been identified by a team led by John O'Leary as originating from the vaccine. The technique was subsequently criticised as being too crude to discriminate wild infection from the vaccine. |
| 2 July 2002 | Ken Livingstone, Mayor of London, announces that he will opt for single vaccines for his as yet unborn child. |
| 7 November 2002 | Danish study of half a million infants finds that autism is no more prevalent in vaccinated vs unvaccinated children. |
| 13 June 2003 | High Court rules that children of two estranged couples should have the MMR vaccine, against the mothers' wishes. |
| 27 February 2004 | Parents who believe their children were damaged by MMR are refused legal aid funding to sue manufacturers of the vaccine. |
| 6 March 2004 | Ten of the 13 authors of the original Lancet paper issue a partial retraction. |
2 Background to the controversy
In February 1998, Andrew Wakefield and twelve co-authors published a study in The Lancet – a respected peer-reviewed medical journal. The paper was published with the highly technical, but seemingly innocuous, title: ‘Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children’. It was based on a study of twelve children who had been referred to Wakefield's clinic with gastrointestinal disease. Most of the children had a regressive form of autism in which they appeared to develop normally as infants, before losing acquired skills including communication.
In medical examinations the lining of the children's intestines all showed patchy inflammation. According to the authors, the findings seemed to support the hypothesis that a damaged intestine may, in some cases, trigger behavioural changes in children. The mechanism suggested for this in the Lancet paper relies on the ‘opioid excess’ hypothesis for autism. When peptides from food such as barley, rye and oats, and casein from dairy products, are not fully digested in the gut, they are absorbed and bind with peptidase enzymes. These enzymes usually break down the naturally occurring peptide opioids that function in the central nervous system. The hypothesis suggests that the consequential disruption of the central nervous system adversely influences brain development.
Wakefield's paper relates that the parents or the physicians of eight of the study's twelve children reported that behavioural problems started within two weeks of the MMR triple vaccine being administered. This evidence was purely anecdotal. In the discussion part of the paper, the authors acknowledge as much: ‘We did not prove an association between measles, mumps, and rubella vaccine and the syndrome described,’ and ‘Published evidence is inadequate to show whether there is a change in incidence or a link with measles, mumps, and rubella vaccine’ (Wakefield et al., 1998).
However, at a press conference to mark the publication of the paper, Wakefield told reporters that he believed that the three vaccines in MMR should be given separately. Investigative journalist Brian Deer (2004) recalls the occasion:
At the centre of the speakers’ table sat the principal author of the study, Dr Andrew Wakefield. Cutting a dashing and charismatic figure, the young gastroenterologist had a very different message to impart. Yes, it was just one study and yes, there was no proof, but he personally believed that action was needed. ‘One more case of this is too many,’ he declared. ‘It's a moral issue for me and I can't support the continued use of these three vaccines given in combination until this issue has been resolved.’ He wanted single jabs.
(Deer, Sunday Times, 22 February 2004)
Reading 1
Although the suggestion of a link between the MMR vaccine and autism was made at a press conference and was not explicitly part of the research paper, the study itself came under fire for its methodology and data interpretation. The question is often asked how such a contentious paper came to be published in the first place. Click on the following link to download a PDF of the original paper published in The Lancet (1998), 351, pp. 637–41 – http://briandeer.com/ mmr/ lancet-paper.pdf (accessed 6 September 2012). It will be useful to have this paper to hand as you now look at Reading 1 in detail. The chapter id entitled ‘The Lancet Paper’ from MMR and Autism: What Parents Need to Know by Dr Michael Fitzpatrick, which outlines the response of the scientific community to the controversy. The author, a general practitioner and himself a father of an autistic son, is a vociferous proponent of the MMR vaccine. As you read, keep a note of the categories of arguments that Fitzpatrick employs in his critique – for example, scientific,
Discussion
What strikes me as particularly significant from Fitzpatrick's account is that the circumstances surrounding the Lancet paper's publication highlighted the subjectivity of the process of deciding not only what scientific research gets done, but also which results get published and why. It is often said in science that ‘the facts speak for themselves’. The circumstances of research approval, publication and reaction to scientific investigations which have political, economic and social consequences seem to me to exemplify what a fallacy this is. The reading also highlights how complex the process is of testing a seemingly straightforward hypothesis in the ‘real world’ as opposed to carefully controlled laboratory conditions.
Fitzpatrick chronicles the barrage of experts stepping forward to criticise Wakefield's study and issue reassurances about the safety of MMR. In spite of this, the effects were dramatic. The Health Protection Agency monitors vaccination uptake in the UK: from a peak of 92% uptake in 1995–96, this figure dropped to below 80% by 2003 and was as low as 60% in some areas. There was a concomitant rise in cases of measles. In 2003, 442 cases of measles were reported: a threefold increase in the numbers reported in 1996. It was clear that a significant number of parents had decided not to immunise their children with the MMR vaccine.
3 Risk perception
At first glance, the public response to the risk of a link between MMR and autism appears to be wildly disproportionate. From a scientific point of view, an association is unsupported by major epidemiological studies involving vast numbers of participants. Neither has evidence been presented of a plausible biological mechanism. Common sense would seem to dictate that the claim to any link simply lacks credibility and well-informed parents should behave ‘rationally’ and allow their children to be immunised, or else run the very real risk of exposing children to potentially serious diseases (see Table 1).
| Disease | Symptoms | Complications |
|---|---|---|
| Measles | Fever, rash, cough, sore eyes, swollen glands, loss of appetite | Ear infection, pneumonia/bronchitis, convulsion, diarrhoea, meningitis, death |
| Mumps | Swollen glands, fever, headache, abdominal pain, loss of appetite | Swollen testicles, meningitis/encephalitis, pancreatitis, deafness, miscarriage |
| Rubella | Fever, headache, rash, sore eyes, cough, swollen glands, joint pains, loss of appetite | Encephalitis, bleeding disorders. In pregnancy: deafness, blindness, heart problems, brain damage in foetus |
These symptoms and complications are unpleasant at best and life-threatening at worst. Yet it may be worth considering the extent to which today's parents have witnessed the diseases of measles, mumps or rubella. A study by Gore et al. (1999) into the factors that affected parents' decisions to immunise found that in communities where infectious diseases were rarely witnessed, immunisations were often considered to be redundant.
Reading 2
Click to view Reading 2, Bellaby, P. (2003) ‘Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination’, BMJ, 327, pp. 725–28. Bellaby argues that parents' responses to the MMR controversy are not necessarily irrational. What factors does he use to support his argument?
Discussion
One of Bellaby's points is that ‘the case evokes cultural and social context rather than “economic man”’ (‘economic man’ is an economist-theory model of human behaviour, which presumes that people act entirely in their own self interest). He shows that context often proves decisive in decision making by parents about whether to allow their children to be immunised with the MMR vaccine.
Although risk is always a social evaluation, rather than a natural phenomenon that can be separated from its context, risk experts often refer to the qualitative aspects as ‘the social amplification of risk’. A combination of circumstances makes certain events seem more risky than the orthodox scientific assessment would have it. One of the main driving forces is the perception of ‘fright factors’. These are characteristics of a controversy that elevate levels of alarm. Bennett (1999) has summarised these ‘fright factors’. He argues that risks are generally more anxiety-inducing if they are perceived to:
-
be involuntary rather than voluntary
-
be inequitably distributed (some benefit while others are adversely affected)
-
be inescapable by taking personal precautions
-
arise from an unfamiliar or novel source
-
result from artificial rather than natural sources
-
cause hidden and irreversible damage
-
pose particular danger to small children or pregnant women, or to future generations
-
threaten a form of death or illness arousing particular dread
-
damage identifiable rather than anonymous victims
-
be poorly understood by science
-
be subject to contradictory statements from responsible sources.
Activity 1
Go through this list of ‘fright factors’ and note down which of them apply to MMR and why.
Discussion
It quickly becomes apparent that the MMR vaccine controversy rates very highly indeed on ‘fright factors’ compared with other types of risks that might, statistically, be more likely to occur. A scientific assessment of risk, which focuses on mathematical probabilities, often tends to ignore these ‘fright factors’, whereas public perceptions tend to prioritise them over statistical and experimental data.
Indeed, assessments of risk are rarely objective. Value judgements, impossible to measure scientifically, often frame individuals' reactions to risk. Thinking of your own response to risk, you might prioritise or downplay certain ‘fright factors’ in any one situation depending on your moral, political, ethical or religious stance.
Scientists have a tendency to frame risk in terms of effects on populations whereas lay people (non-experts, so to speak) tend to be concerned with individuals. This is particularly relevant to an issue such as immunisation where we can see immediately that there may be a tension between a scientific and a lay perspective. No vaccination is without some degree of risk to the individual, however small. Yet for a mass immunisation policy to work, a significant proportion of the population needs to be immunised to achieve ‘herd immunity’ (estimated to be 95% for MMR by the World Health Organization). Scientifically (and politically) the small risk of an adverse reaction is seen as a price worth paying. Most governments acknowledge the inherent unfairness of this. In Britain, in the event of a serious reaction, parents can apply for vaccine damage payments to compensate for ‘sacrificing’ their child's health for the public good. However, financial compensation is likely to be of little comfort to parents whose children have been disabled through vaccine damage.
As the collective memory of diseases like measles and mumps recedes, the risk of adverse effects comes into sharper focus. An appeal to social responsibility in maintaining herd immunity may matter less to parents who perceive the risk of autism to be greater than the risk of contracting measles or mumps. The benefits of protection conferred by immunisation and the risk taken of adverse effects is an individual one, but the risks of transmitting an infectious disease when herd immunity is not maintained are social as they extend to those beyond the MMR dissenters. Indeed, the groups most vulnerable to mumps, measles or rubella are babies too young to be immunised and teenagers whose vaccinations predated MMR, many of whom were not immunised for mumps.
Fitzpatrick (2004) provocatively speculates that for some parents the decision to refuse the MMR triple vaccine has little to do with medical science per se.
Middle class discontents became apparent around a range of political issues: fuel prices, student loans, blood sports and the invasion of Iraq. Yet MMR provided a focus for protest that was both intensely personal and highly political … The controversy over immunisation allowed scope for individual initiative, at least in the form of a gesture of defiance, which was generally lacking in the public sphere.
(Fitzpatrick, 2004, p. 56)
While, for some, withholding immunisation may have had an element of political defiance, for others it was the path of least resistance. Taking a child to be vaccinated is a distressing experience at the best of times. For parents uncertain about what to do, the balance easily tips in favour of postponing a decision or doing nothing (Scottish Executive, 2002).
The picture painted here is that the scientific consensus on the risk that the MMR triple vaccine causes autism is hugely disproportionate to the public perception of that risk – a perception that is influenced by a much wider range of factors. Parents might appreciate that mainstream scientific consensus is that the MMR triple vaccine poses a negligible risk, but these ‘informed dissenters’ may still decide not to immunise their children for a variety of personal or political reasons that have little to do with science.
4 Single vaccines – the middle way?
Much of the campaign surrounding doubts about the MMR vaccine has centred on a call to replace MMR with single vaccines. This is seen as part of a precautionary argument, just in case Wakefield turns out to be right about an association between the MMR vaccine and autism. After all, the spectre of government reassurances about the ‘safety’ of BSE-infected meat and the subsequent climb down still loom large in public consciousness. Comparisons to the BSE crisis were reinforced by Wakefield, who termed the intestinal inflammation he had found in autistic patients as ‘new variant inflammatory bowel disease’ – an unambiguous allusion to ‘new variant CJD’.
Wakefield's hypotheses for MMR-induced damage have always focused on the measles component of the vaccine. If he believes this, why should separate measles vaccine pose any less of a risk? His call for single vaccines is based on a notion that giving too many vaccines at once overloads the immune system. In some cases, it is claimed, the attenuated strain of the measles virus present in the vaccine causes chronic measles infection and leads to the ‘leaky gut’ which renders the developing brain susceptible to damage.
The hypothesis that the immune system is overloaded by combined childhood vaccines has never had scientific currency, but in light of the MMR controversy, a team of researchers led by Paul Offit re-examined the issue (Offit et al., 2002). Modern vaccines contain fewer antigens than in the past. Collectively, the immunisation programme recommended for infants in Britain exposes them to less than 100 antigens whereas the immune system is theoretically capable of responding to about 1010 antigens. Other studies tested the hypothesis that if the MMR vaccine did damage the immune system, an increased level of hospitalisation for infectious diseases would occur following the vaccine. Again, no association was found (Miller et al., 2003). It is, however, worth reflecting at this point on the difficulty in collecting and interpreting trends where there are a multiplicity of interdependent variables – a situation which confounds many epidemiological studies.
The main stance of the Department of Health has been that single vaccines expose children to the possibility of infection while waiting to complete the immunisation schedule. Fitzpatrick (2004) associates the momentum of the single-vaccines campaign with the Labour government's policies which have continuously emphasised parental choice, especially with regard to schools and hospitals. By not making available single vaccines as an alternative to MMR, the government's stance has been seen as an active denial of choice, counter to the policy of patient empowerment.
In stark contrast to the unwavering stance of the government, Wakefield is often portrayed as the ‘listening doctor’ in the press – an image he has taken care to cultivate. In response to criticism of the Lancet paper, he said: ‘the approach of the clinical scientists should reflect the first and most important lesson learnt as a medical student – to listen to the patient or the patient's parent, and they will tell you the answer’ (Wakefield, 1998).
In the battle for hearts and minds that characterises the MMR controversy, the sympathetic Wakefield clearly trumps the perceived heavy-handed authoritarian approach of the health establishment.
5 MMR and the media
5.1 Overview
An important dimension to the social perception of risk is how the media report an issue. Researchers at the Cardiff University School of Journalism investigated media coverage of three scientific issues with social policy implications: climate change; cloning and genetic medical research; and the MMR vaccine. The study analysed the way the media covered the MMR controversy in 561 articles over a seven-month period. Then two nationally representative surveys were carried out in April and October 2002, with the stated aim of investigating how public understanding could be seen as reflecting the nature of the media coverage.
Reading 3
Click to view Reading 3: extracts from the ESRC report Towards a Better Map: Science, the Public and the Media. Take careful note of the way in which the information was obtained and how it is being interpreted. Note strengths and weaknesses of this type of content analysis and social science research.
Discussion
Although surveys of this type inevitably oversimplify the link between media coverage and public understanding of science, the results are useful for identifying certain trends. One of the most interesting findings of the research was that there was a mismatch between the information reported in the media and the public's impression of that coverage. An attempt by the media to provide ‘balance’, by covering both sides of the controversy, created the misleading impression that there was equal evidence on both sides of the debate (39% of respondents to the ESRC survey thought so in April 2002 rising to 53% by October), in spite of the majority of evidence being overwhelmingly in favour of the safety of MMR.
The reporting of the MMR controversy is an example of the ‘myth of balance’ in news coverage. Showing both sides of the story – often considered a hallmark of good reporting – does not guarantee objectivity or accuracy. This is not to say that such coverage somehow lacks legitimacy however. The processes by which news is produced and disseminated are very different to – and often incommensurable with – the processes by which scientific knowledge is generated. In a debate as complex as that about MMR, suffused as it is with politics, economics and ethics, there is no ‘right’ way to report the issue.
5.2 Blair's babe
The ESRC report demonstrated the high awareness amongst the public of the Leo Blair issue, in spite of it not being the most prominent aspect of the media coverage. In December 2001, during Prime Minister's Questions in the House of Commons, Tony Blair was asked whether his infant son had been immunised with MMR. Mr Blair declined to answer on the basis that it was a private family matter. The perception in the media was that if Leo had been immunised, Mr Blair would have been happy to say so. His wife, Cherie Blair, had been the subject of media reports highlighting her interest in New Age alternative medicine which contributed to the suspicion that Mr Blair was promoting MMR in public but opting out in private. The impact of this issue on immunisation levels is hard to measure in isolation but uptake certainly fell in the wake of the publicity (Fitzpatrick, 2004).
Activity 2 What do you think?
Politicians are often criticised for using their families for political gain (recall the now iconic image of John Gummer and his daughter reproduced in Reading 2), yet they are expected to act as suitable role models. Are politicians ethically obliged to follow their recommended policies, or is this indeed an undue invasion of privacy?
5.3 The expert patient
Shifting notions of expertise also feature in the ESRC report. While the medical establishment lined up to proclaim the safety of the MMR vaccine, the anti-MMR voices in the media were mainly provided by parents of autistic children. The unquestionable sincerity of these voices conferred upon them a high level of authority compared with the unemotional scientific evidence given by medical experts.
The continuum between lay expertise and scientific expertise is becoming increasingly blurred. Access to specialist data is no longer the preserve of an academic elite. The internet has meant that swathes of information are instantly available at many people's fingertips. As the volume of accessible information grows, so do the problems of evaluating that information. Doctors and health visitors provide a crucial link in this regard.
The medical profession is somewhat polarised on the concept of an ‘expert patient’. The legitimising of patient views (or, more accurately, parent views in the MMR debate) is seen as a backlash against ‘medical paternalism’. This is the idea that doctors patronise their patients by assuming that they know more about a condition than those living with it. Opponents of this view insist that lay people can never acquire the medical expertise necessary to discriminate between corroborated scientific evidence and rumour, conjecture and superstition. Proponents hold that patients' expertise does not undermine medical authority but helps doctors to understand a condition from a patient's perspective. A government-sponsored expert patient programme encourages patients with chronic illnesses to better self-manage their conditions, recognising that compliance with medication regimes is much more likely if patients have collaborated with their doctors in deciding on treatment (Shaw and Baker, 2004).
The expert-patient scenario described here, in which doctors and patients benefit from mutual expertise, does not ‘scale up’ to the type of media coverage in which patient or parent is often pitted against doctor or scientist. The implication in such coverage is that their expertises are equivalent and comparable. Although views from both lay and medical perspectives are valid in their own right, they are different in scope and focus. Once again, there is potential for tension between the scientific community and the public.
5.4 Telling tales
An aspect alluded to by the ESRC report is the importance of narrative: the way in which we organise events into intelligible stories. Media reports construct narratives, and we also impose our own narratives on the information we glean from a variety of sources. Narrative is a very powerful, often-unconscious human trait. Certain narratives, especially those involving conflict, are cross-cultural and deeply embedded in our psyches. They may have an appeal that transcends logic or conventional rationality. An appealing plot is one in which a sympathetic hero encounters a series of obstacles: everyone seems to be against the protagonist who is seen as a selfless crusader on behalf of common good. Andrew Wakefield easily fits this stereotype in popular imagination: the underdog ‘David’ pitted against the ‘Goliath’ of the medical and government establishment.
Activity 3
The factors that make for a ‘good story’ in the media often share elements of a good fictional plot. Can you identify other science-based news stories in which narrative appeal has potentially shaped public perceptions of an issue?
Discussion
Channel Five recognised the narrative potential in the MMR story and made it explicit: in December 2003 they screened a drama, written by Timothy Prager, called Hear the Silence. It starred Hugh Bonneville as Andrew Wakefield and Juliet Stevenson as the mother of an autistic child convinced of the link between the MMR vaccine and her son's condition. The drama, watched by 1.3 million people, stirred up a huge amount of controversy. Most of the coverage was negative, criticising the drama for being one-sided and for indulging in conspiracy theory. For example, Mark Lawson wrote in the Guardian (8 December 2003):
A series of distracted, sarcastic or conventional doctors representing conventional medicine are systematically shamed and humbled by Saint Mum and Saint Doctor. Scenes in which the Wakefields' phone is bugged and they receive threatening phone calls are casually dramatised, without any explanation of whether it's the drug companies or the NHS or the CIA that is being fingered for intimidation. If you walked into a doctor's surgery looking as lopsided as this drama, you would be sent for emergency orthopaedic surgery at once.
(Lawson, Guardian, 8 December 2003)
Channel Five, anticipating criticism, attempted to balance the anti-MMR message of the drama by following it with a prerecorded debate. Many leading MMR proponents declined invitations to appear on the programme in protest at Channel Five's ‘irresponsible’ dramatisation – ironically contributing ‘silence’ to what had hitherto been a very vocal debate in the media and the medical press. One commentator has this to say:
I can't claim to have been convinced by the heart-on-sleeve ‘heroic little doc versus the mighty medico-political-drug-company establishment’ thesis, but the film was a worthwhile and pungent contribution. Less so was the supposedly ‘balancing’ debate which followed. To stave off the controversy which the drama was bound to attract, Five assembled a panel to discuss the issues. And to emphasise the relative brilliance of drama, MMR: The Debate was ditchwater arid, with crummy sound, amateur camerawork and bad lighting. Perhaps the discrepancy can partly be ascribed to the fact that the film must have cost about a million quid, while the debate came free with a cornflake packet. Andrew Wakefield, Juliet Stephenson and the film's producer were pitched against GPs, biochemists – and a written statement from the Government. As I've said, I'm unconvinced by the film's thrust – but the Government's feeble disregard for the doubters' position can only feed the distrust.
(Courthauld, Observer on Sunday, 21 December 2003)
Whatever the doubts about the MMR message put across, Hear the Silence resonated strongly with parents of autistic children for highlighting the strain experienced by families coping with autism.
The narrative of Wakefield as a misunderstood genius has been reinforced by some of the images accompanying press coverage, most notably a photograph by Phil Hansen in the Sunday Times magazine in December 2003. Wakefield is depicted writing MMR: 1+1+1 ![]() 3 on a window – echoing memorable scenes from the film Beautiful Mind in which Russell Crowe, playing mathematician John Nash, covers his windows with mathematical equations.
3 on a window – echoing memorable scenes from the film Beautiful Mind in which Russell Crowe, playing mathematician John Nash, covers his windows with mathematical equations.
Activity 4 What do you think?
Was Channel Five irresponsible to dramatise the MMR–autism controversy, lending credibility to a scientifically discredited viewpoint? Or is it patronising to assume that the drama's stance will be slavishly adopted by a gullible public, incapable of separating fact from fiction?
6 Everyone's interests
So far we have seen that the MMR debate has been far from neutral, with collective and individual values playing a part in decision making – by scientists, policy makers and parents. One angle of the debate has been a preoccupation with conflicts of interest. With researchers increasingly reliant on funding from sources that have clear interests in the outcome, openness and transparency about who funds what research is deemed essential so that reviewers can take this into account when assessing whether a paper is suitably objective.
Events in the MMR debate took an important turn on 22 February 2004 when the Sunday Times reported that Wakefield had secured £55 000 from the Legal Aid Board in 1996, two months before the study reported in the 1998 Lancet paper commenced. The funding was to investigate the link between the MMR vaccine and autism in the cases of ten children with a view to establishing whether the parents would be able to sue for compensation. ‘Four, maybe five’ of the children were involved in the study reported in The Lancet. Although Wakefield continues to insist that this did not represent a conflict of interest, most of his co-authors and the editors of The Lancet thought otherwise. On 6 March 2004, a ‘partial retraction’ of the original paper was issued by ten of the thirteen authors. Whereas the findings on gastrointestinal problems associated with autism were allowed to stand, the interpretation of a possible link between autism and the MMR vaccine – although this was never made explicit in the paper – was deemed to have had ‘major implications for public health’ and the interpretation was formally retracted.
The Lancet requires authors to declare financial arrangements or personal relationships that could bias their work. The failure to declare the Legal Aid Board funding was the final straw for Lancet editor Richard Horton. Having spent six years defending his own and the journal's reputation from recriminations for publishing in the first place, the incident provided an opportunity for The Lancet to distance itself from what had become one of the most controversial papers ever published.
Reading 4
In a commentary accompanying the partial retraction of the 1998 paper, Richard Horton sets out the difficulties that accompany research of this type, and the problems with decisions about publication. Click to view Reading 4: Horton, R. ‘The lessons of MMR’, The Lancet, 363, pp. 747–49. Horton emphasises that there are ‘lessons to be learned’. List the lessons Horton outlines in this article, and compare it with your own list of what lessons you think should be learned from the MMR controversy. What is your position on the view that Horton was being opportunistic in using the conflict-of-interest issue to deflect criticism of his handling of the matter?
Peer review is often held up to be the criterion which distinguishes research that stands up to ‘scientific scrutiny’. It is a validation gateway through which scientific research must pass before it is admitted to the canon of reliable knowledge. Yet the process of peer review is highly subjective, relying on editors' and reviewers' judgements on the influence of funding sources on interpretation of results. It is widely recognised that few scientists are entirely disinterested in the results of their research, although these interests do not necessarily bias the outcome. However, by not declaring potential conflicts of interest, researchers leave themselves open to accusations of lack of integrity.
A second potential conflict of interest plays an important role in the MMR debate, and that is the funding general practitioners receive for reaching immunisation targets – in the region of £3000 per annum if 90% of the infants on their patient register complete the immunisation programme. This may have a negative effect on the perceived impartiality of the advice given to patients by GPs. Some practices were found to be removing unimmunised children from their registers in order to boost their percentage uptake.
Issues surrounding conflicts of interest serve to highlight the importance of trust. Parenting is largely a matter of instinct. Subjecting a child to a painful, invasive intervention, such as a vaccine, goes against instinct and relies on trust that the procedure is in the child's best interests. No matter how unproven the risk of contracting autism from MMR is, the decision to vaccinate remains a very real dilemma.
7 Concluding remarks
The MMR controversy is inherently complex and there are many additional facets of the debate that go beyond the scope of this course. The issues discussed here have sought to provide a social context for the MMR debate. It is unrealistic to expect scientific aspects to be separable from the myriad other factors that interact with science in a public context.
Decisions about MMR extend beyond science to emotional, ethical and political considerations. Stephen Pattison (2001) points out that ‘scientists must take care not to treat fear and reservation as ignorance and then try to destroy it with a blunt “rational” instrument’. I agree with him that to do so is to trivialise concerns of parents engendered by a lack of trust in official pronouncements of ‘safety’.
At the time of writing (August 2004), the MMR controversy is far from reaching closure. Wakefield is still a key player in the MMR debate, as Chief Medical Scientist for Visceral, a US-based charity which funds research into links between environmental factors and autism. Parents continue to agonise over the decision to allow their children to be immunised with the triple MMR jab. Sadly but inevitably, a small percentage of children will develop regressive autism, whether by coincidence or as a result of some as yet unknown cause.
The controversy surrounding the MMR vaccine has contributed to a lack of public confidence in combination vaccines, undermining a public health policy which has made a very real contribution to protection against infectious diseases. It is perhaps too simplistic to declare that Wakefield's original paper should never have been published. It is clearly undesirable for peer review to operate as a form of censorship: researchers should be allowed to raise concerns that contradict mainstream opinion without being ostracised. Yet the MMR debate has had a life of its own, extending far beyond the technical issues and scientific uncertainties. Could and should the controversy have been better managed? Should lay concerns be considered in conjunction with scientific evidence when making decisions about health policy? If you were faced with a decision on whether to immunise your child with the MMR vaccine, on what evidence would you base your decision?
My son was scheduled to have the MMR vaccine at the height of the flare up of the debate in 2001. My biochemical training and everything I'd read in the scientific research suggested that there was no evidence for a link between MMR and autism. So why was it still such a difficult decision? Parenting is not an inherently rational enterprise. After much soul searching, I did decide to have my children immunised with the MMR. For me, the risks to my children of suffering the ill effects of contracting the diseases themselves, or passing disease on to someone else, outweighed the risk that there might be something after all to the hypothesis that autism is linked to the MMR vaccine. But it was an anxious time – before and after the vaccination. I can empathise with parents who decide that the balance of risk is against MMR immunisation for their children.
Might future controversies be managed better if, for example, uncertainties and dissent are dealt with more even-handedly, lay understandings are acknowledged more explicitly, and the wider social context is articulated and explored?
8 Reading 1: The Lancet Paper
8.1 Reading 1: The Lancet Paper
Fitzpatrick, M. (2004) Chapter 8 ‘The Lancet Paper’ taken from MMR and Autism: What Parents Need to Know, London, Routledge. Copyright © 2004 Michael Fitzpatrick.
We identified associated gastrointestinal disease and developmental regression in a group of previously normal children, which was generally associated in time with possible environmental triggers.
(Wakefield et al., 1998, p. 637)
We did not prove a link between MMR vaccine and this syndrome [‘autistic enterocolitis’].
(Wakefield et al., 1998, p. 641)
Dr Wakefield's landmark paper, published in The Lancet on 28 February 1998, provided the missing link in the theory that MMR was responsible for the supposed ‘autism epidemic’. That link was ‘autistic enterocolitis’ – a novel and distinctive form of inflammatory bowel disease found in children with autism and other developmental disorders. Dr Wakefield was the ‘senior scientific investigator’ in the Royal Free research team and the paper's lead author. A dozen co-authors included paediatric gastroenterologists Simon Murch and Mike Thomson, who did the colonoscopies, child psychiatrist Mark Berelowitz, and Professor John Walker-Smith, who was the ‘senior clinical investigator’. Dr Wakefield and his colleagues believed they had made a discovery of historic significance; it was rumoured that some of them wondered aloud whether they might win a Nobel Prize or some similar recognition if their bold hypothesis was vindicated.
The paper was based on the investigation of 12 children, who were said to have been consecutively referred to Dr Wakefield's clinic at the Royal Free Hospital with a history of diarrhoea, abdominal pain, bloating, and food intolerance. The dozen included only one girl; in ten cases the diagnosis was autism or ‘autistic spectrum dis-order’; in two there was a suspicion of ‘post-viral encephalitis’; and in one the diagnosis was uncertain between autism and ‘disintegrative disorder’. Examination of the lining of the large and small intestine through a fibre-optic endoscope (ileo-colonoscopy) passed up the rectum (under sedation) revealed a distinctive pattern of inflammation (non-specific colitis) associated with enlarged lymph glands at the end of the small intestine (ileal lymphoid nodular hyper-plasia). Microscopic examination of biopsy specimens confirmed chronic inflammatory changes. Furthermore, the authors reported that the parents of eight of the children believed that their behavioural symptoms, characterised as ‘regression’, began shortly after the MMR immunisation (on average after 6.3 days). They suggested that, in these children, the measles virus (present in an attenuated form in the MMR vaccine) might have produced bowel inflammation, allowing toxic peptides to ‘leak’ into the bloodstream and hence pass to the brain, causing autism.
The authors conceded that they had not proved a link between MMR and ‘autistic enterocolitis’. However, they considered that the chronic inflammatory features they had identified in both the small and large bowels of these children ‘may be’ related to neuropsychi-atric dysfunction. The interpretation offered in the summary at the head of the report, as quoted above, was that the authors had ‘identified associated gastro-intestinal disease and developmental regression in a group of previously normal children, which was generally associated in time with possible environmental triggers’ (Wakefield et al 1998: 637). The only ‘environmental trigger’ identified in the report was MMR immunisation, which was linked by eight of the children's parents to the onset of their disturbed behaviour.
8.2 An acrimonious debate
Fitzpatrick, M. (2004) Chapter 8 ‘The Lancet Paper’ taken from MMR and Autism: What Parents Need to Know, London, Routledge. Copyright © 2004 Michael Fitzpatrick.
There were two unusual aspects to the publication of the Wakefield paper and both contributed to the subsequent furore. The first was that it was accompanied by a critical commentary by Robert Chen and Frank DeStefano, two American vaccine specialists (Chen, DeStefano 1998). The second was that it was launched at press conference at the Royal Free Hospital. Let us look at these in turn. As Richard Horton, editor of The Lancet, has indicated in his reflection on the ‘acrimonious debate’ that erupted following his decision to publish the Wakefield paper, he was well aware of its controversial character (Horton 2003: 207). The substance of Dr Wakefield's MMR-autism thesis had already been widely leaked and The Lancet's peer reviewers had raised concerns about the study's methods and interpretations, as well as about the dangers of undermining public confidence in immunisations. Dr Horton insisted that the paper was revised to clarify that its authors had no proof that MMR caused autism, following which it was published under the label of ‘early report’ to ‘highlight its preliminary nature’ (Horton 2003: 208). Furthermore, he commissioned two US vaccine experts, Robert Chen and Frank DeStefano to write ‘Vaccine adverse events: causal or coincidental?’ – a brief but devastating critique of the Wakefield paper published in the same issue of The Lancet (Chen, De Stefano 1998).
Chen and DeStefano first indicated the excellent safety record of MMR in hundreds of millions of people worldwide over three decades. They questioned whether the newly identified syndrome of autistic enterocolitis could be considered clinically distinctive: ‘no clear case-definition was presented, a necessary requirement of a true new clinical syndrome and an essential step for future research’ (Chen, DeStefano 1998: 612). They emphasised that the authors had not confirmed the presence of vaccine virus in the tissues of their patients. They suggested that ‘selection bias’ might have resulted from the referral of children to the clinic of ‘a group known to be specially interested in studying the relation of MMR vaccine with inflammatory bowel disease’ (Chen, DeStefano 1998: 612). They noted that it is usually difficult to date precisely the onset of a syndrome such as autism, and wondered whether ‘recall bias’ may have resulted from parents attempting to relate the onset of their child's problems to an unusual event such as a coincidental vaccine reaction. They also pointed out that, although Dr Wakefield and his colleagues postulated that MMR might lead to inflammatory bowel disease, which, in turn, might cause autism, in almost all the cases reported in their paper behavioural changes preceded bowel symptoms. The time course of these pathological processes was also curious: in one case the effect of MMR on behaviour was evident within 24 hours – faster than any known process of infection-induced vasculitis (the underlying pathology postulated as the cause of ‘autistic enterocolitis, a type of process that unfolds over several weeks).
In conclusion, Chen and DeStefano warned presciently that, if claims of adverse events resulting from vaccines were not properly substantiated, there was a danger that vaccine-safety concerns may ‘snowball into societal tragedies when the media and the public confuse association with causality and shun immunisation’ (Chen, DeStefano 1998: 612). Many of these themes were taken up and expanded in subsequent letters to The Lancet.
In retrospect, Dr Horton conceded that the publication of Dr Wakefield's paper in The Lancet gave it ‘more credibility than it deserved as evidence of a link between the MMR vaccine and the new syndrome’ (Horton 2003: 209). Yet, while he defended his decision to publish the paper, he unreservedly admitted to ‘a failure to manage the media reaction’ – a failure that started with the now notorious Royal Free press conference.
The press conference was an extraordinary event. Journalists were treated to a special introductory video prepared by the Royal Free press office and the Dean of the Medical School, Professor Arie Zuckerman, himself a vaccine specialist, presided over the conference. (Professor Walker-Smith refused to attend, indicating that he disapproved of medical research being debated prematurely in the mass media. He has recalled that the only enthusiasm for the conference came from Dr Wakefield and his staunch ally Professor Roy Pounder, senior adult gastroenterologist at the hospital [Walker-Smith 2003: 241].)
Dr Wakefield seized the next day's headlines with his sensational recommendation that parents should reject the MMR immunisation and give their children each of the three components separately, 12 months apart (The Times, 27 February 1998, Daily Telegraph, 27 February 1998). This recommendation was not included in the Lancet paper and is in no way supported by it. Such a programme of vaccination has not been introduced anywhere in the world and there is no evidence to justify any particular interval between vaccinations. It was immediately repudiated by Professor Zuckerman and by the paediatricians in the Wakefield team. Dr Simon Murch, Dr Mike Thomson and Professor Walker-Smith subsequently wrote to The Lancet to disassociate themselves from Dr Wakefield's call for separate vaccines (Murch et al 1998). Not a single member of the team publicly endorsed Dr Wakefield's anti-MMR stand. Yet, as the press conference broke up in rancour, the campaign against MMR received its biggest boost so far.
Five years later Richard Horton was still smarting from the ‘vituperative attack and personal rebuke’ he experienced as a result of his decision to publish the Wakefield paper (Horton 2003: 213). Many critics complained that The Lancet's process of peer review should have exposed the weaknesses of the paper and prevented its publication. Dr Horton insists that the role of peer review is not to judge the validity of a piece of research – that can only be verified by other scientists – but to comment on the importance of the issue under investigation and on the design and execution of the study (Horton 2003: 213). He decided to publish Wakefield's paper, not because he believed it to be true, but because it raised an important question that required urgent verification. Dr Horton has argued the important principle that medical journals must uphold free expression in scientific debate even if this creates problems for public health. He maintains that to have refused to publish Wakefield would have been an act of censorship. But, as Chen and DeStefano and many others have pointed out, there were basic errors in design, execution, analysis and interpretation in the Wakefield paper. Dr Horton indicates elsewhere that, every year, The Lancet publishes 500 out of 10,000 papers that are submitted: this is not censorship but editorial judgement (Horton 2003: 307). Indeed, when Dr Wakefield submitted his follow-up paper, including a further 48 cases, Dr Horton exercised this discretion and rejected it (it was finally published in the American Journal of Gastroenterology; Wakefield et al 2000).
8.3 MMR and the Medical Research Council
Fitzpatrick, M. (2004) Chapter 8 ‘The Lancet Paper’ taken from MMR and Autism: What Parents Need to Know, London, Routledge. Copyright © 2004 Michael Fitzpatrick.
Although the Royal Free press conference projected the MMR-autism debate onto the national stage, and Dr Wakefield gained a growing status among anti-immunisation campaigners and parents of autistic children, he made little headway in convincing his medical and scientific colleagues of his case. In March 1998, at the request of Sir Kenneth Caiman, Chief Medical Officer, the Medical Research Council (MRC) convened an ad hoc group of 37 experts, drawn from the spheres of virology, gastroenterology, epidemiology, immunology, paediatrics and child psychiatry, to review the associations suggested by the Royal Free team between measles virus and MMR on the one hand, and between inflammatory bowel disease and autism on the other (MRC 1998). The group's meeting was chaired by the pathologist Professor Sir John Pattison (a veteran of the mad cow crisis); Dr Wakefield and epidemiologist Scott Montgomery (one of the Royal Free team) attended the meeting to present and discuss their case.
The group first considered the laboratory evidence produced by the Royal Free group for the hypothesis that measles virus caused inflammatory bowel disease and noted that ‘the most sensitive molecular genetic techniques were negative in the hands of all groups’ (MRC 1998: 2). They emphasised that further studies ‘must involve independent laboratories testing the same specimens, using full controls and a range of techniques with agreed experimental protocols’ (MRC 1998: 2). When considering the epidemiological evidence claimed to link viral infections and inflammatory bowel disease, the group found no correlation between measles or mumps infection alone and Crohn's disease and ulcerative colitis. The experts agreed that there was some correlation between the occurrence of measles and mumps infection within the same year and the later incidence of inflammatory bowel disease. However, they considered existing studies limited and recommended further examination by independent groups.
On autism, the group considered the Lancet paper and emphasised the point that autism commonly becomes apparent in the second year of life – at around the time children receive MMR. However, the group insisted, ‘such coincidence does not imply a causal link’. They pointed out that, whatever the trends in the incidence of autism, they bore no relationship to the Introduction of MMR. They considered that the proposed ‘leaky bowel’/opioid excess mechanism was ‘biologically implausible’ (MRC 1998: 3). They further pointed out that the supposedly distinctive pattern of ‘lymphoid nodular hyperplasia’ identified by the Royal Free group was a common and benign condition in children. Finally, it was argued that the findings of abnormally low levels of some immunoglobulins (IgA) in four out of the twelve children was a simple error resulting from the use of adult normal ranges (when using appropriate paediatric ranges, only one child had a low IgA level) (Richmond, Goldblatt 1998).
After a day-long meeting the experts concluded that there was no current evidence linking MMR and autism. They thought that ‘it would be surprising if the link had not been noted in other countries with good diagnostic facilities for autism where MMR has been widely given for many years’ and suggested that ‘further research on an international basis would settle this matter’ (MRC 1998: 3). The expert group advised the Chief Medical Officer that there was no reason for a change in current MMR vaccination policy, as had been recommended by Dr Wakefield. However, they proposed more research on both inflammatory bowel disease and autism. These Conclusions were sent in summary form to every doctor in the country in a letter from the Chief Medical Officer on 27 March (Caiman 1998).
Dr Wakefield later complained that he felt he had been ‘set up’ at this meeting (Mills 2002: 17). He claimed that the 37 experts had all been ‘picked by the government’ and that he and Dr Montgomery had had to face them ‘alone’. He felt that a nine-hour meeting fell short of the detailed scrutiny he had hoped for.
Following the March 1998 meeting, the MRC set up an expert subgroup to steer and monitor research in inflammatory bowel disease and autism. This subgroup included leading figures in the relevant disciplines and it invited other specialists to attend particular meetings: these included Dr Wakefield, and his co-authors Professor John Walker-Smith and Dr Simon Murch. In its report in April 2000, the subgroup noted further evidence from the Royal Free group of ‘a classic pan-colitis associated with severe constipation and immune dysregulation in a group of children with developmental disorders’ (MRC 2000, Wakefield et al 2000).
This study compared a series of 60 ‘consecutive’ cases of ‘autistic enterocolitis’ (including the orginal 12), with a control group of 37 developmentally normal children undergoing ileo-colonscopy. Given the controversy still raging around the Lancet paper, it was curious that the new study included no information about MMR or any other immunisation history. The study confirmed ‘an endoscopically and histologically consistent pattern of ileo-colonic pathology’ in ‘a cohort of children with developmental disorders’ (Wakefield et al 2000: 2294). It also recorded results of investigations suggesting minor immunological abnormalities. The authors described a subtle ‘new variant’ inflammatory bowel disease, lacking the specific features of either Crohn's disease or ulcerative colitis. They again drew attention to the association of this pattern of bowel disease with ‘a developmental disorder that was associated with a clear history of regression’ – a loss of skills after a year or more of normal development. They concluded that ‘this syndrome [autistic enterocolitis] may reflect a subset of children with developmental disorders with distinct etiological and clinical features’ (Wakefield et al 2000: 2294).
This study was open to the same charges of selection bias as the Lancet paper. It was also criticised on the grounds that the control group was not properly matched for age. Apart from providing a fuller picture of the supposed new syndrome of ‘autistic enterocolitis’, it added little to the continuing MMR-autism controversy. The MRC report concluded that ‘the case for “autistic enterocolitis” had not been proven’ (MRC 2000: 4). It commented that the Royal Free studies had been performed in a ‘self-selected group of patients and the histological finding of ileal lymphoid-nodular hyperplasia may have been secondary to severe constipation’ (MRC 2000: 4).
The subgroup concluded that, in the 18-month period following Dr Wakefield's Lancet paper, ‘there had been no new evidence to suggest a causal link between MMR and inflammatory bowel disease/autism’ (MRC 2000: 5). It conceded that much remained unknown about these conditions and that MRC support for research in these areas, particularly inflammatory bowel disease, was weak. It made a series of specific recommendations for future research.
8.4 Testing the MMR-autism hypothesis
Fitzpatrick, M. (2004) Chapter 8 ‘The Lancet Paper’ taken from MMR and Autism: What Parents Need to Know, London, Routledge. Copyright © 2004 Michael Fitzpatrick.
In the concluding ‘discussion’ section of their Lancet paper, Dr Wakefield and colleagues suggested that further investigations were needed to examine the syndrome of ‘autistic enterocolitis’ and ‘its possible relation’ to MMR (Wakefield et 1998: 641). They indicated two directions for further research. First, the authors observed that if there were a causal link between MMR vaccine and this syndrome ‘a rising incidence might be anticipated after the introduction of this vaccine in the UK in 1988’. They considered that published evidence was inadequate to answer this question, inviting further epidemio-logical research to clarify it. Second, they reported that ‘virological studies’ (presumably those later reported by the team headed by Professor John O'Leary in Dublin, Ireland) were ‘underway’. Let us now examine the outcome of attempts to substantiate the MMR-autism hypothesis through researches in these areas.
In its responsibility for vaccine safety, the Medicines Control Agency commissioned an epidemiological study to investigate the question of whether there was an increase in cases of autism in Britain following the introduction of MMR. Dr Wakefield's challenge to analyse any rise in incidence was taken up by Professor Brent Taylor, community paediatrician at the Royal Free Hospital, and a team including vaccine specialist Dr Elizabeth Miller and Open University statistician Dr Paddy Farrington. Their results were published in The Lancet in June 1999 (Taylor et al 1999a).
They identified all known children with an autistic spectrum disorder born between 1979 and 1998 in eight North Thames health districts 498 children in all – and studied their medical and vaccination records. They found that:
-
although the number of cases of autism had increased steadily since 1979, there was no sudden ‘step-up’ or change in the trend line after the Introduction of MMR in 1988;
-
there was no difference in age at diagnosis between the cases vaccinated before 18 months of age, after 18 months of age, and those never vaccinated;
-
there was no clustering of developmental regression in the months after vaccination.
They concluded that ‘our analyses do not support a causal association between MMR vaccine and autism’ (Taylor et al 1999a: 2026).
The authors themselves acknowledged two limitations of their study. They could not verify the diagnoses of autism in all cases and they may have missed some cases. They relied on clinical notes of variable quality and many did not contain systematic or regularly updated information, which would have allowed independent validation of diagnosis. Despite making ‘substantial efforts’ to identify all cases, they may have missed some children who were not known to local health or education authorities. However, it is unlikely that these factors significantly affected the overall results.
In a letter to The Lancet, Dr Wakefield criticised the Taylor study on three grounds (Wakefield 1999). He claimed that the statistical methodology used (‘case-series’) was inappropriate to detect temporal associations between vaccination and conditions, such as autism, characterised by an insidious onset and delay in diagnosis. On the contrary, the authors replied, this method was particularly suitable for this sort of study, which has a good record of revealing rare adverse effects (Taylor et al 1999b). Dr Wakefield's second objection focused on the authors’ judgement that one finding that of a marginally significant raised incidence of parental concern between 0 and 5 months after MMR – was a statistical artefact. The authors claimed that one such finding (out of 14) might have been expected by chance, and that it could be explained by ‘the combined effect of approximate recording of parental concern at 18 months and a peak in MMR vaccinations at 13 months’. Finally, Dr Wakefield made the accusation that the authors had ‘failed to declare’ the fact that some of the children in the study may have received MMR as a result of a catch-up campaign. The authors’ rebuttal was that these children had been identified and that in all cases in which the age of first parental concern was recorded, it preceded vaccination.
If epidemiological studies failed to support the MMR-autism hypothesis, what about the virological studies? During 2002 two papers based on studies of intestinal biopsies on Dr Wakefield's ‘autistic enterocolitis’ patients by a team lead by Professor John O'Leary in Dublin were published.
In the first paper, published in February, the researchers claimed to have identified fragments of the measles virus in intestinal tissues of 75 out of 91 children with inflammatory bowel disease and developmental disorder (Uhlmann et al 2002). However, this study did not indicate whether the children had had measles or MMR. The authors did not indicate whether they had found whole measles virus, whether of wild or vaccine strain, or any other viruses, such as mumps and rubella. Many commentators wondered whether inadvertent sample contamination or some other technical error with the notoriously difficult reverse transcriptase polymerase chain reaction assays might explain these results (Afzal et al 2003). The study was also criticised on the grounds that the controls were not matched for age or time since vaccination. Others observed that, even if these findings were confirmed and replicated, the presence of measles virus fragments in the gut would not prove that they caused either inflammatory bowel disease or autism.
In response to the controversy generated by his paper, Professor O'Leary issued a statement insisting that he had ‘not set out to investigate the role of MMR in the development of either bowel disease or developmental disorder, and no conclusions about such a role could, or should be, drawn from our findings’ (O'Leary 2002a).
In a presentation in June 2002 to a US congressional committee Dr Wakefield claimed that a new study, due to be published by Professor O'Leary, had confirmed that the measles virus present ‘in the diseased intestinal tissues of children with regressive autism’ was indeed derived from the MMR vaccine (Wakefield 2002a). For Dr Wakefield, these studies constituted ‘a key piece of evidence in the examination of the relationship between MMR vaccine and regressive autism’. Professor O'Leary, however, promptly rejected Dr Wakefield's interpretation of his work, insisting that it ‘in no way establishes any link between the MMR vaccine and autism’. (O'Leary 2002b). Indeed, he strongly recommended that parents should give their children MMR1.
An abstract (summary) of the new O'Leary study was duly presented at the annual meeting of the Pathological Society of Great Britain and Ireland in Dublin in July 2002. This was a pilot study designed to discover whether the measles virus RNA found in the guts of children in the earlier study originated in wild measles or from immunisation. The paper described a technique for discriminating between two closely related genome sequences, which the authors claimed could distinguish between wild and vaccine strain measles (by identifying a single nucleotide at position 7901 of the genetic code of the wild measles virus). They found vaccine-strain measles virus in the gut biopsies of 12 children with inflammatory bowel disease and development disorder (and confirmed wild measles strain in brain specimens of three patients with SSPE – a rare complication of measles). They concluded that ‘this pilot study corroborates our earlier findings of an association between the presence of measles virus and gut abnormalities in children with developmental disorder, and indicates the origins of the virus to be vaccine strain’ (Shiels et al 2002).
However, an immediate response to this study from the WHO collaborating centre for measles in the UK challenged the validity of the technique used by O'Leary's team. This indicated that the method used was not able to distinguish between wild and vaccine strains (it could result in several wild strains being incorrectly classified as vaccine strains). ‘Consequently’, it concluded, ‘the technique described does not reliably discriminate between wild and vaccine measles virus’ (Brown et al 2002). When presented with this information at the US congressional hearings on autism, Dr Wakefield accepted that if this method could not reliably make distinguish the two different forms of measles, then the Conclusion drawn by the paper was not justified. The first piece of evidence promising some support to the hypothesis advanced by Dr Wakefield in 1998 was thus discredited even before publication.
1 It is interesting to note that Professor O'Leary's repudiation of the claims, made on his behalf by Dr Wakefield and his supporters, has never been acknowledged by the anti-MMR campaigners, who continue to cite O'Leary's research in support of the MMR-autism thesis, in explicit defiance of his statements to the contrary.
8.5 MMR safety
Fitzpatrick, M. (2004) Chapter 8 ‘The Lancet Paper’ taken from MMR and Autism: What Parents Need to Know, London, Routledge. Copyright © 2004 Michael Fitzpatrick.
In January 2001 Dr Wakefield adopted a radically different tack in the campaign against MMR. He now turned to the field of public health and vaccination policy, questioning whether appropriate safety procedures had been followed when MMR was introduced into Britain in the late 1980s. In a paper written with his Royal Free colleague, epidemiologist Scott Montgomery, Dr Wakefield claimed that the trials carried out on MMR before it was licensed in Britain involved monitoring children for side effects for only 28 days (Wakefield, Montgomery 2000). They also claimed that the authorities had not taken account of the problems of ‘viral interference’ arising from using the combined MMR vaccine and that early studies had missed or ignored evidence of gastro-intestinal side effects of MMR.
Entitled ‘MMR vaccine: through a glass, darkly’2 the Wakefield and Montgomery paper provoked a storm of controversy.
It was published in the Adverse Drug Reactions and Toxicological Reviews, a highly specialist (and now defunct) journal with a regular readership estimated at around 300. The editors of this journal, anticipating a critical response to the article, published it together with the comments of four reviewers. (Critics subsequently pointed out that, although the reviewers were distinguished in their own fields, they did not include a vaccine specialist.) The most significant comment came from Dr Peter Fletcher, a former head of the Committee on Safety of Medicines, who substantially endorsed the case made by Wakefield and Montgomery and concluded with the damning judgement that ‘the granting of a produce licence [for MMR] was premature’ (Fletcher 2001: 289). In the subsequent discussion, another supporter of the anti-MMR campaign emerged: Dr Stephen Dealler, consultant microbiologist at Burnley General Hospital in Lancashire (Dealler 2001). A veteran of the BSE/CJD controversy, in which he emerged as a protege of Professor Richard Lacey (whose maverick reputation appeared to be enhanced when the nightmare scenario he had long predicted came, at least in part, to pass), Dr Dealler had now become a supporter of Dr Wakefield's theory of autism (see Fitzpatrick 1998: 45–8). He had already published a comprehensive endorsement of unorthodox biomedical approaches to autism on the Internet (Dealler 1999).
Recognising that his most recent paper might not otherwise attract public attention, Dr Wakefield launched the article at a press conference and released copies of the paper to the mainstream media before either public health authorities or doctors involved in giving vaccinations had a chance to read it. Another stormy press conference guaranteed a blaze of publicity (Abbasi 2001).
The Wakefield/Montgomery paper prompted forceful rebuttals from vaccine authorities. On behalf of the Medicines Control Agency, Arlett and Bryan insisted that the MMR trials had followed up children for between six and nine weeks (and, in some studies, for longer) (Arlett, Bryan 2001). They accused Wakefield and Montgomery of errors of statistics and interpretation of key surveys, and claimed that they had missed or ignored other important studies. A scathing review from the Public Health Laboratory Service (now the Health Protection Agency) concluded that ‘overall, we find this paper lacking in a coherent scientific rationale, selective in the reporting and interpretation of other work and statistically invalid’ (Miller, Andrews 2001). Paediatric vaccine specialists dismissed the concerns raised by Wakefield and Montgomery as ‘idiosyncratic’ and questioned the authors' tactics in presenting their paper to the popular press before most clinicians had a chance to read it in a peer-reviewed journal (Elliman, Bedford, 2001).
Two distinct issues were confused in the discussion of ‘interference’ (Arlett, Bryan 2001, Wakefield, Montgomery 2001). One is the question of whether there is a higher incidence of adverse reactions with the combined vaccine, compared with vaccines given separately. Contrary to Dr Wakefield's claims, the consensus emerging from a number of studies is that there is not (Halsey 2001). For the MCA, Arlett and Bryan insisted that there was no convincing evidence of either chronic gastro-intestinal problems or autism resulting from MMR (Arlett, Bryan 2001). The second is the question of ‘immuno-logical interference’: does giving three antigens together lead to a diminished antibody response to each one? According to the review by the American Academy of Pediatrics, ‘although early studies showed the potential for some interference between these vaccine viruses as indicated by reduction in the mean antibody response to one or more of the components in the combined vaccines, adjusting the titres of the vaccine viruses resulted in similar responses for the combined and separate administration of these vaccines’ (Halsey 2001: 25). Arlett and Bryan pointed out that, in 30 studies of the combined MMR vaccine before its Introduction in Britain, no problems of interference had been identified. Furthermore, the effectiveness of post-licensing surveillance had been confirmed by its success in identifying, as a rare adverse reaction, ITP (idiopathic thrombo-cytopenic purpura – a rash associated with a blood abnormality, which usually resolves spontaneously) at a rate of one in 24,000 cases (Miller 2001).
In the subsequent discussion about the safety of MMR a number of issues arose (although none shed much light on the MMR-autism hypothesis). One set of concerns – promoted at first by the wider anti-immunisation movement – focused on the withdrawal in Britain in 1992 of two brands of MMR that used a mumps component derived from the Urabe strain of the virus. In 1988, before the Introduction of MMR in Britain, a study in Canada and the UK reported the occurrence of aseptic meningitis following immunisation with the Urabe strain mumps vaccine, at a rate of between one in 100,000 to one in 250,000. Given that this rate of meningitis was much lower than that occurring with natural mumps (which MMR had been shown to prevent) it was preferable to proceed with the Introduction of MMR. Furthermore, it was not, at that time, clear that any alternative vaccine was safer. However, although passive surveillance procedures showed a very low risk, a more intensive study in 1992 in the Nottingham area revealed a higher incidence of aseptic meningitis at a rate of one in 3,000 – following MMR (Miller et al 1993). Accordingly, the vaccine authorities decided to switch to using only brands of MMR containing the Jeryl Lynn strain of mumps (which had not been linked to cases of meningitis). In response to continuing claims of government perfidy in introducing MMR including Urabe (on the grounds that it was known to cause aseptic meningitis in rare cases), it has been pointed out that, if Jeryl Lynn had not been available, it would still have been preferable to carry on with MMR include Urabe as the benefit from reducing the risk of mumps far exceeded the risk of vaccine-related meningitis.
Another controversy arose from official attempts to promote studies of MMR safety in general as evidence against claims that it caused autism. The most popular study in this regard comes from Finland – a country that introduced a two-dose MMR programme in 1982 and now claims to have virtually eradicated these three diseases. Long-term population-based passive surveillance studies found that no cases of developmental regression had been reported as resulting from MMR in 1.8 million children (Peltola et al 1998, Patja et al 2000). It is true, however, that because people in Finland had no reason to suspect that MMR might be associated with autism, they would be unlikely to report it as an adverse reaction. Dr Fletcher, among many others, was critical of the government's use of such ‘negative studies as absolute evidence of safety’. Nevertheless, the large-scale, long-term, comprehensive and prospective character of these studies make them strong evidence for the safety of MMR in general (Bandolier 2002).
In response to studies of this type, which failed to substantiate the claims of anti-MMR campaigners, they retorted that ‘absence of evidence is not the same as evidence of absence’ (Aitken 2001b) – meaning that just because a particular study does not turn up evidence for the MMR-autism link does not prove that there is no link. (This epithet became something of a mantra.) But two things may be said in response to this. The first is that, as stated in the MCA reply to Wakefield's paper, ‘it is not that there is no evidence, but that there is evidence and it does not show an association’ (Arlett, Bryan 2001: 44). The second is that, if you have looked hard enough for a particular sort of evidence and have failed to find it, the sensible conclusion must be that it is not there and that it is time to think again and look elsewhere. This is how Professor Vivian Moses responded to similar demands for absolute assurances of the safety of genetically modified food products:
Since we can judge present and future safety only on the basis of past experience, an absence of evidence of harm is precisely the only evidence we can ever expect to accumulate for the absence of harm.
(Moses 2002: 2)
Alternatively, one can continue to demand that the rest of the world proves that there is no link, or one can delude oneself that the evidence really is there, if only the rest of the world could see it.
The most curious feature of the ‘through a glass, darkly’ paper is that it has no direct relevance to the MMR-autism link. Even if it were true that pre-licensing surveillance of MMR had been inadequate, this would not advance Dr Wakefield's claim that MMR was causing ‘autistic enterocolitis’ and thus contributing to an epidemic of autism. It is strange that, at a time when he was under intense pressure to substantiate this hypothesis, Dr Wakefield chose to turn aside from his own sphere of expertise (gastroenterology) to enter fields (public health and vaccination policy) in which he had no previous experience. However, a close reading of the concluding section of the paper suggests that Dr Wakefield's strategy was that, if the safety of MMR in general could be put in doubt, the credibility of any particular risk attributed to the vaccine would be raised.
Confident of finding a resonance in an increasingly risk-averse climate, Dr Wakefield invoked the ‘precautionary principle’ popularised by the environmentalist movement:
Surely, when a medical intervention is intended for universal use, particularly in healthy infants, there is almost no limit to the vigilance that should be exercised.
(Wakefield, Montgomery 2000: 277)
With a reference to ‘healthy infants’ that was guaranteed to appeal to the popular press, Dr Wakefield proposed an extreme level of caution that would deter any preventive or therapeutic intervention. In truth, there must always be a limit to vigilance: otherwise we allow the danger against which we are vigilant to become oppressive.
Despite this, at a time when the nation was in the grip of a multiplicity of millennial anxieties, Dr Wakefield readily found the highest authority for his precautionary approach:
As the last Minister for Health, the Hon. Frank Dobson said recently, in the context of another medical intervention, ‘if there is even a hypothetical risk [of harm] and a safer alternative exists, we should use it’
(Wakefield, Montgomery 2000: 279)
As a ‘precautionary measure’ to prevent possible transmission of variant CJD in February 1998, Mr Dobson had insisted that albumen (derived from blood products) used as a stabiliser in some vaccines should be imported from countries not affected by BSE. If the Minister for Health himself could use a hypothetical risk to justify introducing an alternative, then so could Dr Wakefield. He argued, ‘for MMR’, in relation to autism and inflammatory bowel disease, ‘a significant index of suspicion exists without adequate evidence of safety’ (Wakefield, Montgomery 2000: 279).
Although Dr Wakefield had not clearly established either that there was ‘a significant index of suspicion’ about MMR or that its safety record was inadequate, his case appeared to be strengthened by coupling these two dubious propositions together. ‘If the risk of chronic immune-mediated disease is increased by concurrent exposure to the component viruses of MMR, either in their natural or vaccine form’ (a conditional clause that remained unvalidated), then, Dr Wakefield triumphantly concluded, by giving the vaccines separately ‘we have the ability to artificially dissociate these exposures, and the possible associated risks’ (Wakefield, Montgomery 2000: 279). By disparaging the safety record of MMR and inflating unsubstantiated risks, Dr Wakefield may not have advanced the MMR-autism thesis, but he had given a powerful boost to the demand for separate vaccines.
2 The title is derived from the epistles of St Paul: ‘For now we see through a glass, darkly; but then face to face: now I know in part; but then shall I know even as I am known’ (Corinthians I; 13:12).
8.6 Moving the goalposts
Fitzpatrick, M. (2004) Chapter 8 ‘The Lancet Paper’ taken from MMR and Autism: What Parents Need to Know, London, Routledge. Copyright © 2004 Michael Fitzpatrick.
If these researchers are able to prove cause and effect between immunisation and the described syndrome, they should do so straight away. If they are unable to do so they should publicly set the matter straight lest the health of our nation's children suffers.
(Lindley, Milla 1998)
This challenge to Wakefield and his colleagues was issued by two senior gastroenterologists at Great Ormond Street Hospital for Children in immediate response to the Lancet paper in February 1998. Five years later Wakefield and his colleagues had still neither proven their hypothesis, nor withdrawn it.
In response to the failure of research in the two areas recommended in the Lancet paper – epidemiology and virology – to substantiate his hypothesis, Dr Wakefield continued to support the campaign against MMR, while redefining his case for its causative role in autism. At the outset, the concept of MMR-induced ‘autistic enterocolitis’ was advanced to explain a dramatic increase in the incidence of autism (the ‘autism epidemic’). Before long, however, a close temporal association between MMR and the onset of behavioural regression – at first regarded as a significant indicator of causation – was relaxed and then abandoned. When epidemiological studies still failed to substantiate a link, Dr Wakefield hypothesised that MMR caused ‘autistic enterocolitis’ in a subset of children, rendered vulnerable by a combination of genetic and environmental factors (including food allergy, antibiotic use, ear infection, multiple concurrent vaccine exposure, a strong family history of atopic and auto-immune disease, and exposure to mercury) (Wakefield 2001b). (This list of possible cofactors in the aetiology of autism – familiar from our account of unorthodox biomedical approaches to autism – reflects Dr Wakefield's growing reliance on parent activists and anti-immunisation campaigners.)
In a response to a Danish epidemiological study (published in the New England Journal of Medicine in November 2002) that failed to show any link between MMR and autism, Dr Wakefield argued that this subset may be ‘no more than 10 per cent of diagnoses’ (Madsen et al 2002, Wakefield 2002b). In a subsequent letter to the journal, Dr Wakefield appeared to give up on epidemiology, arguing that the effect of the number and complexity of cofactors was ‘to reduce statistical power to the extent that such studies fail to offer any convincing evidence either way’ (Wakefield 2002b). Or as he put it in a newspaper interview in March 2003, ‘retrospective studies like this are meaningless’ (Phillips 2003: 43). But it was retrospective studies such as this that Wakefield specifically invited in his Lancet paper.
The end result of this process of shifting the goalposts is that MMR, once blamed for producing an autism epidemic, is now said to be a factor in causing autism in a number of cases too small to discern by epidemiological methods. If this is so, how can MMR have caused autism in more than 1,000 cases currently pursuing compensation under the leadership of Richard Barr (with expert medical advice from Dr Wakefield)? We know that such methods of study are capable of detecting rare adverse effects of immunisation, such as ITP at a rate of one in 32,000 vaccinations (around 20 cases a year), so detecting a subset the size of 10 per cent of all cases of autism should be fairly straightforward.
Given the failure of epidemiology to confirm his hypothesis, Dr Wakefield has counter-posed the need for clinical studies – a call loyally echoed by his anti-MMR campaign followers. But populations are made up of individuals: if an effect of MMR – a vaccine administered at a population level – cannot be discerned at a population level, then it does not exist. Furthermore, Dr Wakefield's attempts to substantiate his hypothesis at a clinical level, in collaboration with Professor O'Leary, have also failed to bear fruit.
Unfortunately, instead of accepting the failure to prove their hypothesis, and – in the interests of public health – withdrawing it, Wakefield and his supporters have doggedly and dogmatically continued to proclaim their conviction that MMR causes autism in some children, in defiance of all evidence to the contrary.
As the anti-MMR campaign found itself on the defensive, its supporters mounted increasingly personal attacks on critics of the Wakefield position. Brent Taylor and Elizabeth Miller, whose epidemiological work provided the most powerful defence of MMR, came in for particular vilification. In response to their 1999 paper, for example, Allergy-induced Autism issued a scurrilous denunciation of these authors, accusing them of ‘a cynical attempt to disguise the truth’ and of perpetrating ‘a scandalous public dupe of BSE proportions’ (AiA 1999). It demanded the resignation of ‘all key members of the study group’ insisting that such an ‘attempt to justify health policy by using inadequate research as propaganda is reprehensible’. The criticisms of the Taylor study made by AiA were the same as those made by Dr Wakefield in a slightly more restrained letter to The Lancet. In his testimony to the US senate committee hearing in April 2000, Dr Wakefield claimed that the Taylor paper was the subject of a ‘highly critical’ debate at the Royal Statistical Society in London, which concluded that the ‘study design was wrong’ (Wakefield, Montgomery 2000). In fact no such debate took place and the Royal Statistical Society came to no Conclusion about the design or validity of the study. This study was described by the US Institute of Medicine's immunisation safety review as ‘the most extensive epidemiological study and the strongest published evidence against the hypothesis that MMR causes ASD [austistic spectrum disorder]’ (Institute of Medicine 2001: 44).
As the debate became increasingly polarised, Wakefield and his supporters resorted to impugning the motives of critics of the campaign against MMR by alleging conflicts of interest arising from their links with vaccine manufacturers. Two distinct issues thereby became confused.
First, as a result of the class action against the manufacturers of MMR, the pharmaceutical companies concerned were obliged to seek expert advice from the small pool of specialists in the relevant disciplines. These specialists received fees for their services, in the same way that expert witnesses for the plaintiffs received fees from the Legal Aid funds secured by Richard Barr and his team. Though payments should be disclosed where there is any question of a conflict of interests, the notion that the receipt of such fees implies a loss of professional discretion and integrity is both absurd and offensive. Given the low profile of pharmaceutical companies in paediatrics or autism, it is highly unlikely that any of these specialists would have become ‘drug company advisors’ if it were not for the activities of the anti-MMR campaign.
Second, paediatricians or immunologists who are engaged in research or clinical trials of vaccines are obliged to do this work in collaboration with pharmaceutical companies, since virtually all vaccines are manufactured by such companies. It is standard practice that researchers are excluded from investing for personal gain in companies sponsoring their research. However, although they may not gain personally, professional success is to some extent dependent upon generating research funding, so it is legitimate to declare this interest. According to Adam Finn, professor of paediatrics at the University of Bristol, such declarations should be interpreted as a qualification to give a well-informed opinion, ‘as anyone unable to declare such competing interests is unlikely to have had any direct experience of using new vaccines in children’ (Finn 2002: 733). However, in the rancorous climate generated by the MMR controversy, anti-MMR campaigners have presented such declarations of interest – available on easily accessible official websites – as though they were investigative journalists uncovering conspiracy and corruption. Although the implication that everybody is governed by the most venal motives is widely held in modern society, it is corrosive of any kind of civilised discourse.
Populist jibes against the drug companies are a recurrent theme among campaigners against all forms of immunisation. No doubt the pharmaceutical corporations, like all capitalist enterprises, are more concerned about their profitability than the welfare of their consumers. There are many areas in which they can be legitimately accused of profiteering, disease-mongering and sharp practice (see Moynihan et al 2002). Yet the provision of vaccines, a relatively low-volume and low-profit sector, is not one of them. Indeed it is an area characterised by low investment and declining innovation, partly as a result of the climate of risk aversion and litigiousness, particularly in the USA (Galambos 1999). In August 2003 a report by the US Institute of Medicine complained of supply problems resulting from the declining number of vaccine manufacturers and urged the government to subsidise vaccine costs (Institute of Medicine 2003). The report noted the relatively small size of the vaccine market in the USA and the fact that vaccines accounted for only 1.5% of global pharmaceutical sales. Companies complained that their return on investment was small and there was little incentive towards research and development. In a contribution to a conference on vaccination in the USA in October 2003, Richard Gallagher, editor of The Scientist, noted that ‘vaccinations are unattractive targets for industry, under-appreciated from the public health perspective, underfunded by basic research organisations, and treated with suspicion by the public’ (Gallagher 2003). He commented on the ‘malign influence’ of three groups – anti-vaccination lobbyists (whose ‘ignorant’ websites included contributions from ‘health nuts, conspiracy theorists and misguided physicians’), journalists (who wrote ‘badly-researched and poorly-argued scare stories’) and lawyers. At the same conference, vaccine specialist Neil Halsey noted that class action lawsuits led to large damage awards and complained that the courts provided a forum for ‘junk science’ in the guise of expert testimony (The Daily News, 27 October 2003).
8.7 References for Reading 1
Fitzpatrick, M. (2004) Chapter 8 ‘The Lancet Paper’ taken from MMR and Autism: What Parents Need to Know, London, Routledge. Copyright © 2004 Michael Fitzpatrick.
Note: Internet sites originally accessed between January and December 2003.
Abbasi, K. (2001) ‘Man, mission, rumpus’, British Medical Journal; 322: p.306.
Afzal, M.A., Osterhaus, A.D.M.E., Cosby, S.L., Jin, L., Beeler, J., Takeuchi, K., Kawashima, H. (2003) ‘Comparative evaluation of measles virus-specific RT-PCR methods through an international collaborative study’, Journal of Medical Virology; 70: pp. 171–6.
Allergy Induced Autism (1999) Statement on Taylor et al. 1999, at http://www.whale.to/ vaccines/ aia.html.
Aitken, K.J. (2001b) ‘Q&A’ at http://www.singlevaccines.com/ ken-aitken1.html.
Arlett, P., Bryan, P. (2001) ‘A response to “MMR: through a glass, darkly” by Drs A.J. Wakefield and S.M. Montgomery and published reviewers’ comments’, Adverse Drug Reactions and Toxicological Review; 20 (1): pp. 37–45.
Bandolier (2002) ‘MMR vaccination’ at http://www.jr2.ox.ac.uk/ bandolier/ band84/ MMR.html.
Brown, D.W.G., Jin, L., Ramsay, M. (2002) ‘Comments on abstract submission’, Infectious Diseases in the News (27 June), London: Public Health Laboratory Service (http://www.phls.org.uk/ press).
Calman, K. (1998) ‘MMR vaccine, Crohn's disease and autism’, From the Chief Medical Officer (27 March).
Chen, R.T., DeStefano, F. (1998) ‘Vaccine adverse events: causal or coincidental?’, Lancet; 351: pp.611–12.
Dealler, S. (2001) ‘MMR and toxicology’, Adverse Drug Reactions and Toxicology Review; 20(1): pp.55–7.
Elliman, D., Bedford, H. (2001) ‘MMR vaccine: the continuing saga’, British Medical Journal; 322: pp. 183–4.
Finn, A. (2002) ‘MMR vaccine debate: competing interests need to be declared’ (Letter), British Medical Journal; 324: pp.734–5.
Fitzpatrick, M. (1998) ‘How now mad cow?’ in I. McCalman with B. Penny and M. Cook (eds.), Mad Cows and Modernity: Cross disciplinary reflections on the crisis of Creutzfeldt-Jakob Disease, Humanities Research Centre Monograph Series No. 13, Canberra: Australian National University.
Fletcher, A.P. (2000) ‘Referee 3’ (comments on ‘MMR vaccine: through a glass darkly’ by A.J. Wakefield and S.M. Montgomery) Adverse Drug Reactions and Toxicology Reviews; 19 (4): pp.288–91.
Galambos, L. (1999) ‘A century of innovation in vaccines’, Vaccine; 17: S7–10.
Gallagher, R. (2003) ‘Vaccination undermined’, The Scientist; 17 (22) (17 November): p.6.
Halsey, N.A. et al. (2001) ‘MMR vaccine and autistic spectrum disorder: a report from the new challenges in childhood immunisation conference’, Paediatrics; 107(5): e84.
Horton, R. (2003) Second Opinion: Doctors, diseases and decisions in modern medicine, London: Granta.
Institute of Medicine (2003) Financing Vaccines in the 21st Century: Assuring access and availability, Washington, DC: National Academy of Sciences.
Lindley, K.J., Milla, P.J. (1998) ‘Autism, inflammatory bowel disease, and MMR vaccine’ (Correspondence), Lancet; 351: p.907.
Madsen, K.M., Hvidd, A., Vestergaard, M., Schendel, D., Wohlfart, J., Thorsen, P., Olsen, J., Melbye, M. (2002) ‘A population-based study of MMR vaccine and autism’, New England Journal of Medicine; 347: pp. 1477–82.
Miller, D.L., Madge, N., Diamond, J., Wadsworth, J., Ross, E. (1993) ‘Pertussis immunisation and serious acute neurological illnesses in children’, British Medical Journal; 307: pp.1171–6.
Miller, E., Andrews, N. (2001) ‘Comments on “MMR: through a glass darkly”’ (http://www.phls.co.uk/ facts/ Vaccination/ 012201wakefield.htm).
Mills, H. (2002) MMR: The story so far, Private Eye Special Report, London: Private Eye.
Moses, V. (2002) ‘Chewing over GM food’, spiked-online, 5 February, http://www.spiked-online.com/ Articles/ 00000002D3EF.htm.
Moynihan, R., Heath I., Henry D. (2002) ‘Selling Sickness: The pharmaceutical industry and disease mongering’, British Medical Journal; 324:pp.886–91.
MRC (Medical Research Council) (1998) ‘Group concluded no reason for change in MMR vaccine policy’, Press Release Ref: 09/98, London: MRC.
Murch, S., Thomson, M., Walker-Smith, J.A. (1998) ‘Autism, inflammatory bowel disease, and MMR vaccine’ (Correspondence: authors’ reply), Lancet; 351: p.908.
O'Leary, J.J. (2002a) ‘Link found between measles virus and gut abnormalities in children with developmental disorder’ (Press Statement) (see mp.bmjjournals.com/cgi/content/full/54/DC1).
Peltola, H. Patja, A., Leinikki, P., Valle, M., Davidkin, I., Paunio, M. (1998) ‘No evidence for MMR vaccine-associated inflammatory bowel disease or autism in a 14-year prospective study’, Lancet; 351: pp.1327–8.
Phillips, M. (2003) ‘MMR: the truth’, Daily Mail, 11–13 March.
Richmond, P., Goldblatt, D. (1998) ‘Autism, inflammatory bowel disease, and MMR vaccine’ (Correspondence), Lancet; 351: p. 1355.
Shiels, O., Smyth, P., Martin, C., O'Leary, J.J. (2002) ‘Development of an ‘allelic discrimination’ type assay to differentiate between the strain origins of measles virus detected in intestinal tissue of children with ileocolonic lymphonodular hyperplasia and concomitant developmental disorder’. Abstract (No 20) presented at Pathological Society of Great Britain and Ireland (http://www.pathsoc.org.uk/ meet/ prog.shtml).
Taylor, B., Miller, E., Farrington, C.P., Petropooulos, M.-C., Favot-Mayaud, I., Li, J. Waight, P.A. (1999a) ‘Autism and MMR vaccine: no epidemiological evidence for a causal association’, Lancet; 353: pp.2026–9.
Taylor, B., Miller, R., Farrington, C.P. (1999b) ‘MMR vaccination and autism’, (Correspondence: authors’ reply), Lancet; 354: p.950.
Uhlmann, V., Shiels, O., Wakefield, A.J., O'Leary, J. (2002) ‘Potential viral pathogenic mechanism for new variant IBD’, Journal of Clinical Pathology and Molecular Pathology; 55 (2): pp.84–90.
Wakefield, A.J., Montgomery, S.M. (2000) ‘MMR vaccine: through a glass darkly’, Adverse Drug Reactions and Toxicology Reviews; 19: pp.265–83.
Wakefield, A.J. (2001b) ‘Testimony of Dr Andrew J Wakefield before the Government Reform Committee of the US House of Representatives’, at http://www.unlockingautism.org/ testimonies/ index.
Wakefield, A.J. (2002b) Visceral, Press release, November, in response to Madsen et al. (2002) at http://www.visceral.org.uk.
Wakefield, A.J., Murch, S.M., Anthony, A., Linnell, J., Casson, D.M., Malik, M., Berelowitz, M., Dhillon, A.P., Thomson, M.A., Harvey, P., Valentine, A., Davies, S.E., Walker-Smith, J.A. (1998) ‘Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children’, Lancet; 351: pp.637–41.
Walker-Smith, J.A. (2003) ‘Enduring Memories: A paediatric gastroenterologist remembers’, London: The Memoir Club.
This completes Reading 1. Please click here to return to the main course.
9 Reading 2: Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination
9.1 Communication and miscommunication of risk
Bellaby, P. (2003) ‘Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination’, British Medical Journal, 327, 27 September 2003, pp. 725–28. Reproduced by permission from the BMJ Publishing Group; Mary Evans Picture Library Ltd; P A Photos.
In this article on the public perception of risks Paul Bellaby considers three examples of risks to children in the UK – an insignificant risk (autism caused by MMR vaccine), a real but probably small risk (vCJD from BSE), and a real and demonstrably larger risk (injuries from road crashes) – and contrasts the perceptions of the risks by parents
Science cannot prove a negative, but, where their children are concerned, parents want to be assured that risk is zero. Would establishing a comprehensive ‘Richter scale’ of risks remove that misunderstanding? If not, then what accounts for miscommunication of risk and how might it be overcome? In this article I try to provide answers by considering public perception of three risks, each of a different order, all involving children:
-
Autism linked to the combined measles, mumps, and rubella (MMR) vaccination
-
Variant Creutzfeldt-Jakob disease (vCJD) arising from food containing the causative agent for bovine spongiform encephalopathy (BSE)
-
Injury and death in road transport crashes.
9.2 Background
Bellaby, P. (2003) ‘Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination’, British Medical Journal, 327, 27 September 2003, pp. 725–28. Reproduced by permission from the BMJ Publishing Group; Mary Evans Picture Library Ltd; P A Photos.
In 1998 Wakefield was the first to make the claim that autism and the MMR vaccine are linked.1 It is based on a dozen clinical cases of gastrointestinal disorders with which developmental regression seemed to be linked. They arose in previously normal children. His team found that eight of the 12 parents attributed the onset to the MMR vaccination. On a population level, diagnoses of autism increased rapidly from 1988, when MMR was introduced, and through the 1990s, not only in Britain but also in North America. Yet epidemiologi-cal studies have found no link between increasing numbers of diagnoses of autism and the Introduction of MMR vaccine.2, 3 The weight of scientific opinion is that the risk is insignificant.
By contrast, there is both laboratory and epidemio-logical evidence for the transmission of BSE from cat-tle to humans. Consumption of mechanically recovered meat, common among children, has been implicated.4 The risk is considered real but small. Brown et al estimate 10–15 cases a year from its first appearance in 1994, eight years after BSE was identified in UK cattle,5 and Ghani et al suggest that the primary epidemic in the known susceptible genotype began to decline in 2001.6 It seems that the outbreak of
BSE that led to vCJD abated long ago, and no further cases are likely to be incubating.
Injuries incurred in road transport crashes by children (ages 0–15 years) are easy to demonstrate, common, and recur year on year. In 2002 there were 34 689 casualties from road crashes in Great Britain, of whom 4596 received serious injuries or were killed.7 Children (like elderly people) are relatively vulnerable as pedestrians. They are also prone to cycling injuries. But about 45% of child road casualties are car passengers (more than 70% for those aged under 2 years). Although the overall number of casualties from road crashes continues to decline, children are progressively more likely to travel by car and less likely to walk or cycle, even to get to school.8 This is one of the factors implicated in the decline of exercise and increasing obesity in children.
9.3 Parents' responses to the risks
Bellaby, P. (2003) ‘Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination’, British Medical Journal, 327, 27 September 2003, pp. 725–28. Reproduced by permission from the BMJ Publishing Group; Mary Evans Picture Library Ltd; P A Photos.
Although road transport crashes carry by far the largest risk of the three, they have raised little controversy.

The alleged link between MMR vaccination and autism and the small risk of vCJD both met with widespread concern from parents. There has been conflict between expert and lay opinion about MMR and vCJD. Bartlett suspected collusion between government and industrial interests to cover up the threat from BSE.9 Similar suspicions of cover up by government developed after Wakefield's claims about MMR and autism.
Adams dismissed the possibility of a Richter scale of risk, arguing that uncertainty and probability are elusive concepts and that the public quite reasonably finds some risks readily perceptible10; but others, known to experts, are not acknowledged by the public, and still others are “virtual” rather than real. Unfortunately this classification does not seem to account for how parents perceive the three risks in question. Road transport crashes are perceptible risks, the low risk of vCJD is an expert assessment, and the link between autism and MMR is, if anything, virtual. Parents seem to neglect the easily perceptible risk, to reject the expert assessment, and to amplify the virtual risk.
Does this suggest that parents are irrational? Might they be pawns of mass media that seek not the truth but to support minorities against authority, as Bedford and Elliman imply?11 It is a short step from answering “yes” to arguing that the authorities ought to act in the interests of the child, if need be against the wishes of parents, as the Court of Appeal has ruled against two mothers in recent cases involving MMR vaccination.12
9.4 Lessons from history
Bellaby, P. (2003) ‘Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination’, British Medical Journal, 327, 27 September 2003, pp. 725–28. Reproduced by permission from the BMJ Publishing Group; Mary Evans Picture Library Ltd; P A Photos.
Yet there is a history to compulsory vaccination of infants in Britain that is an object lesson for today. From its Introduction in law in 1853, compulsory smallpox vaccination for infants provoked vigorous opposition, not only from middle class radical liberals, but also from working class movements.13 It was not until 1898 that conscientious objection was allowed, but this followed progressive decline in compliance with vaccination law from about 1889. From then on, Britain differed from most countries, including the United States and Germany, in not relying on compulsory vaccination in order to control smallpox.

A comparison of vaccination policy and its effects on population health in England and in Prussia and Imperial Germany from 1835 to 1914 suggests that compulsory vaccination led to an earlier downturn in smallpox in Germany. However, by the end of the period, both countries had controlled the disease.14 This was partly attributable to disease surveillance and containment in Britain, but was also due to another factor, which contributed to Britain's success with many childhood diseases at the turn of the 20th century. This was active engagement with the public at local level in health improvement.15 By the late 19th century, the liberal middle classes were encouraging the “deserving poor” to change their lifestyles by face to face engagement in their homes, schools, and neighbourhoods.16 At the same time, they might provide an example of domestic management and hygiene to the many women servants in middle class homes who would later rear their own children in working class areas.
9.5 What went wrong with MMR?
Bellaby, P. (2003) ‘Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination’, British Medical Journal, 327, 27 September 2003, pp. 725–28. Reproduced by permission from the BMJ Publishing Group; Mary Evans Picture Library Ltd; P A Photos.
The extent of people's willingness to conform to public health programmes in Britain was and remains considerable. From the Introduction of the MMR vaccination in 1988 until the scare broke in 1998, levels of take up had been high, rising to 92% in 1997, sufficient to achieve population immunity. One estimate based on surveys to date is that take up fell by only 8.6% from 1995 to 2001.17
In 1988, at the start of the MMR campaign, take up was higher in affluent areas-a familiar pattern in Britain and North America.18, 19 Up to 1997, the affluent pattern of take up spread to less affluent areas.20 All the more remarkable then, that, from 1998, take up decreased first in affluent areas and more so than in deprived areas. Even when parents decided for MMR vaccination, a study based on focus groups among the public indicated widespread misgivings.21 A survey of health professionals who provided vaccination for children suggested that parents’ unease rubbed off on the professionals.22
The vicissitudes of the MMR campaign show that “mass communication” is mediated or filtered in different ways, through the diverse groups that comprise society and through hierarchies, including the medical profession. It should be no surprise that the same message conveys different meanings to different people.
The conduct of the media may have contributed to the miscommunication of risk,23 but it would be a mistake to suppose that the media led the public. Parents were predisposed to act in what seemed to them to be the interests of their children. The response of “the establishment” confirmed for some their suspicions that inconvenient truths would be covered up. The handling of the earlier BSE crisis lent support to this view. In the case of MMR vaccination, the chief medical officer would not meet parents’ concerns half way by sanctioning access to single disease vaccinations. The grounds for refusal were reasonable enough: the six administrations required in all (measles, mumps, and rubella, each twice) would increase the likelihood that vaccinations would not be completed. In the United States children under 18 months old are now given protection against 11 childhood diseases, which requires some 15–19 doses of vaccine, and this has driven healthcare managers to seek ways of reducing infant distress and so making the process more acceptable to parents.24, 25 After 1998, many UK parents would probably interpret the chief medical officer's argument as insulting, both to their conviction that they were acting in their children's interests and to their competence as responsible parents to ensure that individual vaccination courses were completed.
In spite of appearances to the contrary, one can argue that parents have behaved rationally, not only with respect to MMR vaccination, but also in relation to vCJD and road transport crashes. The case evokes cultural and social context rather than “economic man.” True, as the economic man argument suggests, parents who refuse vaccination may “free ride” on the compliance of the majority in order to secure the benefit of herd immunity for their child. But, taken together, responses to the three risks we have reviewed suggest that parents are acting conscientiously as norms dictate, not selfishly. They act in what they perceive to be the interests of their children. If there seems to be any risk to their child, responsible parents will avoid it. Thus, they avoid beef products, and they question the safety of the MMR vaccination. Even though taking children to school and elsewhere by car may have unintended consequences for their health and safety, it is interpreted as a way of protecting them from greater dangers on the streets from other road users and abduction by strangers.26
9.6 Changing parents' perceptions
Bellaby, P. (2003) ‘Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination’, British Medical Journal, 327, 27 September 2003, pp. 725–28. Reproduced by permission from the BMJ Publishing Group; Mary Evans Picture Library Ltd; P A Photos.
Vaccination has a heroic history in the control of communicable diseases. However, collective provision that is taken for granted today in Britain-not just vaccination, but also sewerage, clean water supply, and food safety-had to be fought for. In the mass mobilisation wars of the 20th century, several public health plans that had foundered for lack of public support in peace time came to seem necessary for the war effort. But mass mobilisation is not a normal state in healthy democracies. A consequence of peace is that public health measures that have not become part of infrastructure have often been challenged. For example, when rationing of food was lifted in 1954, nutritional standards and their rough equality achieved during the second world war were sacrificed for the sake of choice.27
The case of public reaction to MMR vaccination should be viewed in this broader historical context. Any attempt to restore the compulsion that failed in the late 19th century would almost certainly fail again. Instead, public health professionals and scientists should consider the lessons that experience with MMR offers and apply it in the future. The first is that challenge to authority, including the authority of science, should be expected in a healthy democracy. The second is that the establishment should disseminate evidence to the public in a transparent way that is sensitive to the ways of understanding of diverse groups. The third lesson is that communicating risk effectively to the so called masses, and so priming people to act appropriately, is about much more than providing even the best of information: it is a matter of two way communication and obtaining agreement. Concordance has to be the aim if compliance is to fall into place.28
Summary points
The size of a risk does not necessarily relate to the controversy it causes.
Parents seem to neglect the most obvious risks to their children (such as road crashes), reject expert assessment (as over BSE), and amplify a virtually non-existent risk (autism from vaccination).
Yet public willingness to conform to public health programmes remains high, and parents' behaviour is not necessarily irrational.
Parents' behaviour is understandable if they are seen as acting to protect their children within a particular social context.
Competing interests: None declared.
9.7 References for Reading 2
Bellaby, P. (2003) ‘Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination’, British Medical Journal, 327, 27 September 2003, pp. 725–28. Reproduced by permission from the BMJ Publishing Group; Mary Evans Picture Library Ltd; P A Photos.
-
Wakefield AJ, Murch, SH, Anthony, A, Linnell, J, Casson, DM, Malik, M, et al. ‘Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children’. Lancet 1998;351:637–41.
-
Kaye, JA, Melero-Montes, M,Jick, H. ‘Mumps, measles, and rubella vaccine and the incidence of autism recorded by general practitioners: a time trend analysis’. BMJ 2001;322:460–3.
-
Taylor, B, Miller, E, Lingam, R, Andrews, N, Simmons, A, Stowe, J. ‘Measles, mumps, and rubella vaccination and bowel problems or developmental regression in children with autism: population study’. BMJ 2002;324:393–6.
-
Cousens, S, Everington, D, Ward, HJT, Will, RG, Smith, PG. ‘The geographical distribution of variant Creutzfeldt-Jakob disease cases in the UK: what can we learn from it?’ StatMethods Med Res 2003;12:235–46.
-
Brown, P, Will, RG, Bradley, R, Asher, DM, Detwiler, L. ‘Bovine spongiform encephalopathy and variant Creutzfeldt-Jakob disease: background, evolution, and current concerns’. Emerg Infect Dis 2001;7:6–16.
-
Ghani, AC, Donnelly, CA, Ferguson, NM, Anderson, RM. ‘Updated projections of future vCJD deaths in the UK’. BMC Infect Dis 2003;3:4.
-
Office of National Statistics. ‘Road accident casualties: by road user type and severity 1991–2001‘. Annual Abstract of Statistics 2003. http://www.statistics.gov.uk/ STATBASE/ ssdataset.asp?vlnk= 4031 (accessed 17 Sep 2003).
-
DiGuiseppi, C, Roberts, I, Li, L. ‘Influence of changing travel patterns on child death rates from injury: trend analysis’. BMJ 1997;314:710–3.
-
Bartlett, DMC. ‘Mad cows and democratic governance: BSE and the construction of a “free market” in the UK’. Crime, Law and Social Change 1998;30: 237–57.
-
Adams, J. ‘A “Richter scale for risk”? Scientific management of uncertainty versus management of scientific uncertainty’. Interdiscip Sci Rev 1998;23:146–55.
-
Bedford, H, Elliman, D ‘Press: MMR: the onslaught continues’. BMJ 2003;326:718.
-
Durbach, N. ‘“They might as well brand us”: working class resistance to compulsory vaccination in Victorian England’. Soc Hist Med 2000;13: 45–62.
-
Hennock, EP. ‘Vaccination policy against smallpox, 1835–1914: a comparison of England with Prussia and Imperial Germany’. Soc Hist Med 1998;11:49–71.
-
Szreter, S. ‘The importance of social intervention in Britain's mortality decline c 1815–1914: a reinterpretation of the role of public health’. Soc Hist Med 1988;1:1–39
-
Marks, L. Metropolitan maternity: maternal and infant welfare services in early twentieth century London. Amsterdam : Rodopi, 1996. (Wellcome Institute series in the history of medicine.)
-
Ramsay, ME, Yarwood, J, Lewis, D, Campbell, H, White, J. ‘Parental confidence in measles, mumps and rubella vaccine’. Br J Gen Pract 2002;52:912–6.
-
Boulianne, N, Deveuninck, G, Lavoie, F, Dionne, M, Carley, J, Valiquette, L, et al. ‘Why some 2-year-old children are not completely immunized’. Can J Public Health 2003;94:218–23
-
Bobo, JK, Gale, JL, Thapa, PB, Wassilak, SGF. ‘Risk-factors for delayed immunization in a random sample of 1163 children from Oregon and Washington’. Pediatrics 1993;91:308–14.
-
Middleton, E, Baker, D. ‘Comparison of social distribution of immunisation with measles, mumps, and rubella vaccine, England, 1991–2001’. BMJ 2003;326:854.
-
Evans, M, Stoddart, H, Condon, L, Freeman, E, Grizzell, M, Mullen, R. ‘Parents' perspectives on the MMR immunisation: a focus group study’. Br J Gen Pract 2001 ;51:904–10
-
Petrovic, M, Roberts, R, Ramsay, M. ‘Second dose of measles, mumps, and rubella vaccine: questionnaire survey of health professionals’. BMJ 2001;322:82–5.
-
Science Media Centre (2002) MMR: learning lessons. http://www.sciencemediacentre.org/ aboutus/ MMRreport.html (accessed 1 Sep 2003).
-
Lutwick, SM. ‘Pediatric vaccine compliance’. Pediatr Clin North Am 2000;47:427–34.
-
Mullany, L. ‘Considerations for implementing a new combination vaccine into managed care’. AmJManag Care 2003;9(1 suppl):S23–9.
-
Hillman, M, Adams, J, Whitelegg, J. One false move … a study of children's independent mobility. London: PSI Publishing, 1990.
-
Huxley, RR, Lloyd, BB, Goldacre, M, Neil, HA. ‘Nutritional research in World War 2: the Oxford nutrition survey and its research potential 50 years later’. BrJNutr 2000;84:247–51.
-
Vernon, JG. ‘Immunisation policy: from compliance to concordance?’ BrJ Gen Pract 2003;53:399–404.
This completes Reading 2. Please click here to return to the main course.
10 Reading 3: Towards a better map: Science, the public and the media
10.1 Media coverage of the MMR controversy
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
Unlike the other two stories, the MMR coverage conforms to a more conventional news pattern in which a story breaks, generates discussion and debate, then fades away. Of the 561 stories on MMR recorded over a seven and a half month period, 56 percent of the entire sample appeared in one month between 28 January and 28 February. Coverage was most concentrated on television, after Panorama broadcast a programme at the beginning of February on Dr Andrew Wakefield's latest research into the possible links between autism, bowel disease and the MMR vaccine (71 per cent of television coverage appeared period between 2nd and 16th of February).
While the other two stories involve a variety of angles and themes, the reporting of the MMR story was fairly consistent, revolving around the same set of messages and ideas. The story also followed a fairly clear narrative, with the Prime Minister playing a central role. The main focus of the story is the possibility of a link between the MMR jab and autism (or bowel disease linked to autism), a fact mentioned in over two thirds of stories on this issue. It is this link – and hence the more general idea that the MMR jab may be unsafe -that clearly provided the impetus for the story.
However, the source of these claims – Andrew Wakefield's research – is mentioned in only a quarter of these stories, with the broadsheet newspapers accounting for most of these references (suggesting that this was an aspect of the story that was often dropped by those media with less space available).
The bulk of evidence suggests that the MMR vaccine is safe – as opposed to the well established risks of the diseases themselves. The use of such evidence to was often used to ‘balance’ Wakefield's claim – although not, perhaps, as widely as might have been expected. Television took the lead in this respect: half the television reports on the issue referred to such evidence, while less than a third (32 per cent) of the broadsheet press reports did so. Similarly, over a third of all TV reports mentioned that the MMR vaccine is regarded as safe in the 90 countries in which it is used – a point made in only 11 per cent of reports overall.
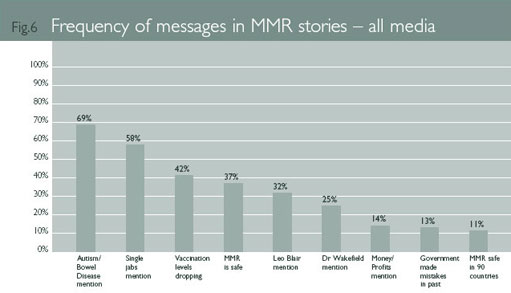
Attempts to balance claims about the risks of the MMR jab tended merely to indicate that there were two competing bodies of evidence rather than offer more substantive evaluations of the case for or against a link. The following example are typical:
“Ministers continue to insist the MMR jab which some doctors have linked to autism is the best way of protecting children” (ITV News, 5th Feb, 2002).
“Although health chiefs insist that the MMR vaccine is safe, many parents have been put off by uncertainty over possible links to autism and bowel disorders” (Daily Mail, 5th Feb, 2002).
“The government has mounted campaigns to persuade parents the MMR jab is safe after some research linked it to autism and bowel disorders in children” (The Sunday Times, 28th April, 2002)
The MMR vaccine was introduced in 1988 by Edwina Currie, then Tory Health Minister. In February 1998, Dr Andrew Wakefield and his colleagues from the Royal Free Hospital published a paper in the Lancet (Wakefield A J et al, 1998) based on a study of 12 children with an unusual bowel syndrome (linked to autism). Wakefield et al purported to have discovered traces of the measles virus in their guts. Although this experiment has been repeated a number of times since then, no other researcher has had similar results. The paper in the Lancet did not present evidence linking MMR to bowel syndrome or autism, but at a press conference publicising the research, Dr Wakefield argued that giving children the vaccines in three separate doses would be safer – a suggestion not supported by his many co-authors nor by any scientific evidence.
The evidence provided by Wakefield's research – limited as it is – involves a link between the measles virus (as opposed to the MMR vaccine itself) and a form of bowel disease linked to autism. The connection between the MMR vaccine and autism is a speculative claim made by Wakefield with questionable scientific data to support it.
Despite this, Wakefield's claims were not comprehensively or systematically challenged in media coverage. It is beyond the remit of this study to account for this failure: what is certainly true is that the weakness of empirical evidence in support of Wakefield's claim was never fully aired.
Recent coverage was prompted by two simultaneous events; a measles outbreak in South London and an episode of Panorama broadcast on 3 February 2002, asking ‘How safe is MMR?’ Dr Wakefield, Professor O'Leary and colleagues then pre-published a paper in Molecular Pathology to accompany the Panorama edition, which focused on this research.
Even if we accept the link in Wakefield's data, on the basis of the empirical evidence, it is not clear that a single measles vaccination would be safer than the MMR jab. There is no data establishing a link with autism that compares the MMR vaccine to the measles virus. Nonetheless, the media coverage quickly moved to the speculative link- without, in most cases, exploring Wakefield's actual data. Because the risks involved with non-vaccination are fairly clear, the idea of offering three single vaccinations as a potentially safer alternative thereby gained a great deal of currency – especially on television and in the tabloids (where 71 per cent and 62 per cent of stories mentioned the proposal to offer single jabs).
This government's reluctance to offer single jabs (on the basis that might reduce overall levels of vaccination, when the bulk of evidence suggested MMR was safe and no evidence directly implicated the MMR vaccine), pushed attention onto the Prime Minister. The fact that Tony Blair had a young child was seen as a test of the government's integrity on this issue.
The Prime Minister's refusal to disclose whether Leo Blair had been vaccinated with the MMR jab tended to increase speculation on the matter, and around a third of all the MMR reports (32 per cent) referred to it.
The following transcript from ITV news, broadcast on 4th February, is indicative of the way the story developed:
“It was reported over the weekend that Leo Blair has had the jab although Downing Street still won't officially confirm it. In Tonight's poll most respondents think that Tony Blair should go public. 80 per cent also want alternatives to MMR. This Liverpool clinic does just that – offering single jabs for each disease to worried parents.”
Parent (holding child): “You should be able to have your children vaccinated singly at your own doctors. I object strongly to being told what and when to inject into my children.”
Dr Pat Troop, Deputy Chief Medical Officer: “We have no concerns about our current vaccine. I think it will send a very strong signal that parents will say, hang on we think that maybe there is a problem around this vaccine – why else would you offer us a single vaccine – and confidence would go.”
This report also demonstrates how the argument against single jabs is more difficult to make in a limited amount of time than a simple appeal to parental choice. Indeed, the framework constructed here very clearly places the burden of proof on the side of those defending the MMR vaccine (one of the earliest studies examining the relationship between science coverage and public opinion found that the appearance of a dispute often works to benefit opponents of technology – Mazur 1981: 114).
The decline in public confidence suggested by this report led to another recurring theme – the idea that vaccination levels were falling as a consequence of parental anxieties. This point was made in 42 per cent of MMR stories, despite the limited evidence available to confirm it. In February 2002 the rate of MMR vaccinations had dropped by approximately six percent in the previous five years (it is unclear how much this is due to a lack of confidence in the vaccine). A number of media reports used data rather selectively, which, although often technically correct, implied a more dramatic fall in the take up of the MMR jab.
So, for example, the Today programme reported that the MMR vaccine was down to ‘70 per cent uptake in some areas’ (2nd Feb, 2002), the Mail reported that ‘Uptake of the triple vaccine has fallen to ‘dangerously low levels’ in some areas, according to the Public Health Laboratory Service’ (2nd Feb, 2002), while ITV News reported that ‘in parts of London that figure is down to 65 per cent – meaning only two children in three are having the MMR jab. With so many children left unprotected medical experts fear there is a distinct possibility of a measles epidemic…’ (5th Feb, 2002).
Other media simply made claims without any supporting evidence. The Sun, for example, reported:
“growing concern of possible links between MMR and autism and bowel disorders have seen a massive drop in the number of parents opting for the treatment. The connection was made by Dr Andrew Wakefield in 1998. No scientists confirmed his findings but many parents say their children changed dramatically after the injection”.
(The Sun, 5th Feb, 2002)
This example from The Sun is also indicative of the nature of the balance struck between competing claims. Since most health experts were fairly clearly lined up in support of the MMR vaccine, balance was often provided by pitching medical experts against parents: an approach facilitated by the work of parental pressure groups on this issue. This created a serious difficulty for scientists and health professionals, who are only able to propose dry generalisations against the more emotive and sympathetic figures of parents concerned for the welfare of their children.
Our own survey suggests that more parents would, given a choice, still opt for the MMR vaccine over three separate vaccinations or no vaccinations at all. The media coverage, on the hand, suggested anti-MMR parents outnumbered those in favour by more than 5 to 1.
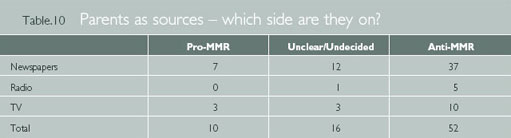
There is, of course, a danger here of a significant decline in take up of the MMR vaccine becoming a self-fulfilling prophecy, a point we explore below. The key question we should ask is whetherthe coverage enabled members of the public to make informed decisions about MMR, either as citizens (on a matter of public policy) or as parents of young children.
10.2 Media coverage of cloning and genetic medical research
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
Kitzinger and Reilly, writing about the coverage of genetic research, identified the dichotomous nature of media coverage on this issue. Human medical genetic research is either framed in terms of'the ‘great promise’ discourse focusing on the benefits the science can bring’ or else, the ‘concern’ discourse, focusing on the risks associated with the application of knowledge gained’ (1997: 322). Our study confirms that this dichotomous framework remains very much in operation: reports tend to be scientifically technical, or else avoid all mention of science and concentrate on the ethical aspect of genetic medical research.
The Sun's coverage of the creation of a national Cell Bank is a good example of this dichotomy, to the extent that the same story is reported twice with very different headlines. The first story, on August 28, 2002, led with the headline ‘EMBRYO CELL BANK SHOCK’, clearly prompting the ‘concern’ framework, even if the copy itself is less alarmist:
“HUMAN embryos are to be used by Government scientists to create a bank of cells for medical research. Couples will be asked to donate embryos left over after IVF treatment. The Medical Research Council would then build up a stock of stem cells – the body's building blocks which can develop into any type of cell. Critics claimed there would be undue pressure on IVF couples to make donations. But the Department of Health said: ‘We welcome the initiative’.”
Two weeks later (on September 10, 2002) The Sun reported the same issue with the headline ‘STEM CELLS BANK A FIRST’, suggesting that such a thing was a symbol of scientific progress.
“EUROPE'S first stem cells bank may be set up in the UK within a year, it was announced yesterday. The National Institute for Biological Standards and Control has won a Pounds 2.6million government contract to run one in Hertfordshire. Stem cells – the body's base cells – can be extracted from embryos and adult bone marrow. Doctors will use them to treat such diseases as Parkinson's and diabetes.”
The ‘great promise’ framework relies upon an understanding of the medical potential of genetic medical research, and television and radio reports on this issue tend to also do a better job than the press in explaining why this kind of science is of medical importance. Television, in particular, is consistent in explaining the scientific rational behind the research, and did so in 16 of the 17 news reports on this issue. However, whilst television may be presenting the issue with a mission to explain it, there is little television coverage overall. So, for example, while the House of Lords decision to permit experimentation of cloned embryos on February 28th was top of both I TV and BBC early evening news broadcasts, coverage of the story was not sustained, making only sporadic appearances over the next six months.
Less than a third of newspaper articles by contrast (32 per cent), explain the scientific rationale behind most of this research. And although the Mail was more likely than many other newspapers to include a scientific rationale, it also provides an example of how this scientific context tends to be excluded when the story moves into the ‘concern’ framework, as in the following editorial:
“In America a lesbian couple deliberately produce a test-tube baby that is, like themselves, deaf. Meanwhile, it is reported that a patient of Italian fertility expert Professor Severino Antinori is pregnant with the world's first human clone, though medical opinion fears for its health in the unlikely event of it ever being born. Such stories provide a chilling, warning vision of the nightmare world we could be entering by allowing such irresponsible dabbling with the very stuff of human life” (8th April, 2002).
Figure 7 shows how often the scientific context is often omitted from newspaper articles about genetic medical research. The first column ‘Science Explicitly Explained’ represents instances where newspapers have dedicated more than one sentence to explaining the science associated with the story covered.
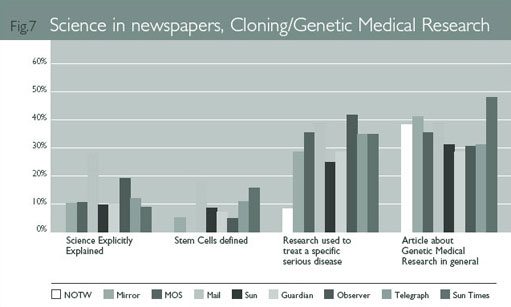
One could argue that the greater volume of newspaper stories on this issue means that explanations might appear to editors to be repetitive. So, for example, The Sun and The Daily Mirror both ran short explanatory pieces on the day of the House of Lords ruling – (‘STEM CELLS: THE FACTS’ AND ‘HOW STEM CELLS CAN AID MEDICINE’ respectively). The problem with this argument, as we shall see, is the implication that public understanding is such that such repetition is unnecessary.
This lack of clarity may be compounded by the news value given to the more disturbing orfrivolous possibilities of cloning research, with headlines like ‘SCIENTISTS TO CLONE EXTINCT BEASTS FOR THEME PARK’ (The Sun, 20th Aug, 2002) or ‘JUST WHAT THE WORLD NEEDS – ANOTHER TIDDLES’ (The Observer, 17th Feb, 2002). The first of these stories – despite its scientific implausibility – was the subject of a follow up The Sun, through one of their regular ‘vox pops’ featuring the views of a ‘White Van Man’, who opined on August 24th: ‘This is crazy. Scientists could be unleashing something dangerous. I don't think they should be playing around with nature – they might get some nasty surprises…’
Figure 7 also shows that a number of stories in the sample addressed Genetic Medical Research, as opposed to cloning. A smaller percentage of these articles referred to current research helping specific diseases, making it easier for the public to understand why the research was carried out. The following two articles show how journalists and politicians use a reference to a medical disease as a short cut in explaining the research:
“BRITISH scientists yesterday announced a breakthrough in the treatment of cervical cancer – that could be taken in an OINTMENT. They have identified a molecule that kills cancerous cells but ignores healthy ones. The scientists claim it could be sold in ointment form – avoiding surgery or radiotherapy, which affect fertility …” (The Sun, September 6, 2002, upper case in original article).
“I want to make the UK the best place in the world for this research, so in time our scientists, together with those we are attracting from overseas, can develop new therapies to tackle brain and spinal cord repair, Alzheimer's disease and other degenerative diseases, such as Parkinson's,” said Mr Blair … (The Daily Telegraph, May 24, 2002).
On the whole, the dichotomous coverage would, in terms of style, seem to lean in favour of the ‘concern’ framework, which is generally more dramatic and engaging than the coverage of more benign developments in cloning and genetic medical research, which are generally pigeon-holed as ‘science’ stories. Some newspapers do attempt to liven up their coverage, however, with the use of celebrities. Although not mentioned in significant numbers in most media on this issue, celebrities appear in half of all the cloning and genetic medical research articles in the News of the World - in particular the actor Michael J Fox's battle with Parkinsons disease and Christopher Reeve's support for stem cell research.
In terms of public understanding, the main issue here would seem to lie in people's ability to connect these two frameworks. In short, we need to understand something about the science of cloning and genetic medical research if we are to make the ethical judgments that place this issue in the public domain.
10.3 The media and the public understanding of science
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
In this section we shall explore the public understanding of and attitudes towards science on the basis of two nationwide surveys. We will look in detail at public knowledge of the three issues we have tracked thus far, and then explore the relationship between media coverage and public understanding.
10.4 Trust
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
Our first survey in April showed that people, in theory at least, differentiate between types of scientists in terms of trusting the information they receive.
Most people place a great deal of trust in university research scientists, while a majority say they distrust what scientists working for private business have to say.
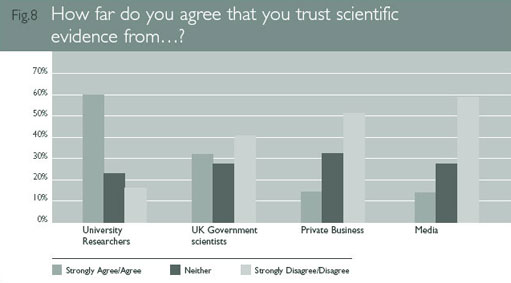
Government scientists come somewhere in between the two. This suggests that scientific information is partly judged in terms of the perceived independence of those producing it. It also reflects trends in other surveys showing the decreasing trust people have towards the motives of private business.
The relevance of this for media coverage is not as straightforward as it might seem. Even if it is clear from media coverage who a scientist quoted is working for (and, perhaps more pertinently, where their funding comes from), it is unlikely, given the generally low levels of recall elicited by news, that most people are able to attend to such detail when absorbing information.
A majority also say they distrust scientific information they receive from the media – another response we should not take at face value. Research generally suggests that many people often claim to receive media – especially, in the British case, the press – with a high level of critical scepticism. This scepticism tends to be somewhat abstract, however, as people tend to trust the media they actually use (Hargreaves and Thomas, 2002). Given this, it is not at all certain that people are actually this discriminating in processing information (Lewis, 2001; Kitzinger, 2000), as we will see shortly.
Since our first survey suggested that people assume that the motive behind research is important to understanding the research itself, we explored the issue further in our second survey. The results here suggest that if some people are cynical about the aims of scientific research, a clear majority – 70 per cent – still see scientific research as a force for good in the world.
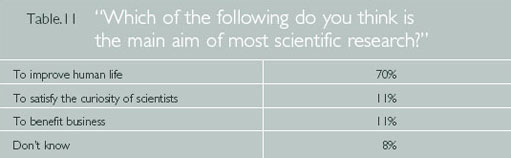
While one in seven (14 per cent) of the stories on the MMR coverage in our study refer to a decrease in the trust of science and scientists in the last few years – this response would indicate that one should not over-estimate this loss of trust. So, how big an impact did issues like CJD/BSE, in which mainstream science was called into question, actually have on people? The second survey asked the following open-ended question, with responses as listed:

Thus prompted, a majority do imply a decreasing level of trust, although since the question tends to encourage this response, it is notable how many – 45 per cent – say that nothing has decreased their level of trust. And while the CJD/BSE outbreak is often regarded in media discourse as the key moment in this respect, it may be a distant memory for some people, since it only just heads a fairly wide list of issues people were able to nominate.
10.5 Overall levels of scientific understanding
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
Both surveys asked the same 13 questions in order to establish levels of public understanding of science or science policy. The questions were designed to test a basic (rather than advanced) knowledge of the science or research, with particular emphasis on exploring the policy and political developments in relation to scientific issues. It is worth noting, at this point, that we are not suggesting that these questions are all necessarily things people need to know to be able to make useful or worthwhile responses to these issues. Some facts, in this respect, are clearly more pivotal than others. We shall return to this in our Conclusion: at this point, we want simply to record what people knew, what they didn't, and, crucially, how these things might be responses to media coverage.
All the questions in the index were multiple choice, offering between two and five possible answers. The average number of correct responses remained remarkably constant – and fairly low – across the two surveys, decreasing marginally from 5.0 correct responses in April to 4.9 correct responses in October (around 38 percent in both surveys). On the basis of this, it is clear that overall levels of public understanding are fairly low, especially when one considers that the average score is not much higher than it would have been – given the multiple choice format- had people been guessing arbitrarily throughout. We should note, however, that the shape of responses do suggest a degree of understanding, albeit limited, in some areas.
What is, perhaps, more surprising, are the scores amongst those with more science education, or more education generally. While those with more education did better, the difference between those with more and less education was not as great as might have been expected.

So, for example, while those with no science education at all scored between 4.3 and 4.5, those with science degrees only scored just above 50 per cent (between 6.8 and 6.9).
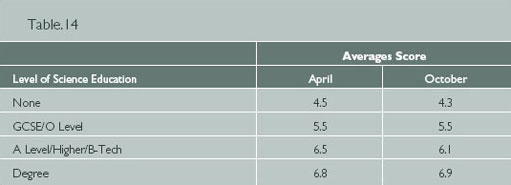
In terms of age, those between 45–54 scored highest, with the under 25s and over 65s scoring lowest. There are some interesting exceptions to this, which we will look at later in relation to climate change.
Although television is the most popular source of information about science related stories (59 per cent say it is their main source of such information1), the amount of television people watch has little effect on knowledge. Heavier television users tend to score lower, although this group also tends to be less educated. The frequency with which people watch television news also has little discernible effect, with the exception of people who watch little or no news, who do tend to score lower.
Perhaps not surprisingly, broadsheet readers did better than tabloid readers, although again, differences are not that great. Most broadsheet readers averaged scores between five and six, tabloid readers between four and five (although readers of the Daily Star were well at the bottom of both surveys, averaging around 3.5 correct answers).
Given the fairly low levels of knowledge overall, it is not surprising that when we asked respondents (in the October survey) if there were occasions when they ‘felt confused about scientific issues’, most – 79 per cent – said yes. Interestingly, those who admitted feeling confused knew slightly more (4.9 to 4.7) than the 21 per cent who claimed they did not!
When it came to self-assessment in relation to three issues, people were a little more self-aware. In each case, those who felt well informed about the issues did better than those who felt ‘partly informed’, with those saying they felt ‘not very well’ informed scoring lowest.
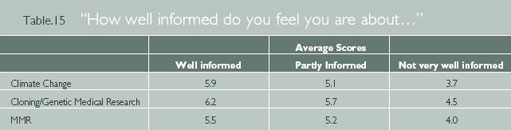
Once again, however, the differences are not great, all of those groups claiming to be well informed scoring an average less than 50 per cent. This highlights the problems in testing knowledge purely through self-assessment (an increasingly common practice) revealing as it does the gap between claiming to be informed and actually being informed. While self-assessment might be useful in measuring people's self-confidence, such measure do not, on their own, tell us what or how much people know.
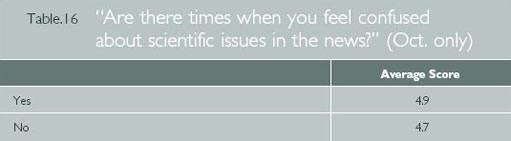
If most people are sometimes confused about scientific issues, who do they blame? Chiefly, according to half the people in our survey, the complexity of the scientific issues themselves. Yet how difficult is most of the basic science that makes it into the news? While science can, like any discipline, be very difficult, most of the questions in our public understanding index were at a fairly basic level. So, for example, the ‘greenhouse effect’, in which greenhouse gases accumulate to prevent heat from escaping from the Earth's atmosphere, is a fairly simple concept to understand. As an idea, it is not much more complex than understanding, say, the offside rule in football (let alone the difference between, say a 4–4-2 and a 3–5-1-1 formation). And yet most people (16 per cent in the April survey, 17 per cent in the October survey) were simply unaware of the workings of the greenhouse effect, assuming, instead, that greenhouse gases thinned the ozone layer (a response we shall look at in more detail when we look at the public understanding of climate change).
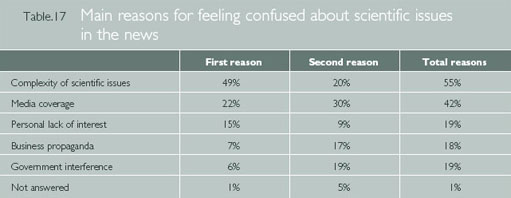
The second most nominated source of confusion was the media, and it is to the role of the media that we now turn.
1 This is followed by 22 per cent who nominate newspapers as their main source, seven per cent say radio, five per cent the internet, four per cent magazines, two per cent books and two per cent say their friends. Newspapers top the list of second favoured sources (45 per cent, followed by television (25 per cent), radio (11 per cent), friends (five per cent), the internet (five per cent), magazines (four per cent) and books (three per cent).
10.6 What did we learn from media coverage between April and October?
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
The simple answer would appear to be simple – we did not learn very much that we didn't know before. As Figure 9 suggests, patterns of knowledge or ignorance are remarkably consistent across both surveys.
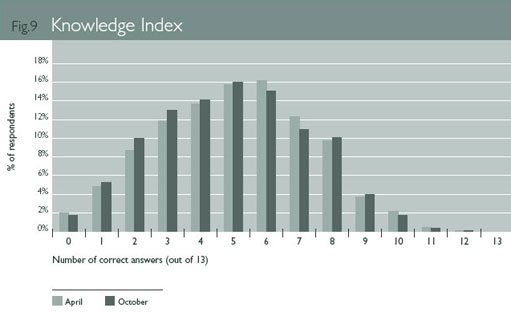
In terms of question by question comparisons, most differences between the two surveys fall within a three per cent range. Only five knowledge questions showed shifts of five per cent or more from April to October. We found:
-
a seven per cent increase of those who correctly identified a forest as an example of a ‘carbon sink’ (up from 51 per cent to 58 per cent);
-
a five per cent increase of people incorrectly identifying ‘less rainfall in winter’ as a predicted outcome of climate change (from 19 per cent to 24 percent), although correct responses (‘more rainfall in winter’) only dropped by one per cent (from 53 per cent to 52 per cent);
-
a seven per cent drop in those who correctly stated that the bulk of evidence suggested no link between the MMR vaccine and autism (from 30 per cent to 23 per cent), with a 14 per cent increase in those stating incorrectly that there was ‘equal evidence on both sides of the debate’ (up from 39 per cent to 53 percent);
-
a seven per cent drop in those incorrectly stating scientists had recently cloned a human being (from 16 per cent to nine per cent – although the shift here was a seven per cent increase in ‘don't knows’ rather than towards a correct response);
-
a six per cent increase in those correctly identifying the treatment of disease as the main focus of stem cell research (from 60 per cent to 66 per cent), with a five per cent drop in those incorrectly identifying the creation of identical copies of human beings as the main focus (from 11.5 per cent to 6.5 per cent).
Most of these shifts are still too small to be anything other than mildly suggestive. The only discernible pattern in these responses is a small shift in the understanding of stem cell research, away from fears about the cloning of human beings, and towards an awareness of the use of stem cell research for treating disease (a point we shall take up shortly).
Overall, however, most increases and decreases in knowledge are minor and scattered fairly arbitrarily. This suggests that, despite fairly persistent media coverage of these issues, there is no significant increase in public understanding. This does not imply, however, that the media coverage has had no impact on public understanding, merely that any impact on knowledge is fairly consistent over time. This finding is very much in line with other studies of public opinion, which tend to find that, unless subject to major media campaigns, changes are gradual and long-term (see, for example, Page and Shapiro 1992). For those wishing to influence public understanding, this not only requires remaining (to use current political jargon) ‘on message’, but doing so in way that establishes or fits within the overall framework of news reporting.
We shall develop our understanding of the media's role when we look in more detail at knowledge of the three issues, when some interesting patterns emerge. As we shall see, the framework for understanding an issue may develop fairly quickly in a burst of coverage (as with MMR), or with repetition of longer periods of time (as with the other two issues). This presents a real challenge for anyone seeking to influence public opinion.
10.7 The media and public understanding of climate change
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
Our analysis of media coverage suggested that this was an issue that received more attention in the broadsheets than the tabloids, with The Guardian and The Sun/News of the World being at the two ends of the spectrum. It is notable, then, that in the October Survey 83 per cent of Guardian/Independent readers felt that climate change ‘was something we should be concerned about’, compared with only 55 percent of Sun readers. A significant proportion of readers would therefore appear to be following their newspaper's lead in their levels of concern, or else have selected a newspaper in line with their own preoccupations.
More profound, perhaps, is the way media content is generally reflected in the public understanding of climate change. In short, people are aware of the issue, and most people are able to link climate change to the destruction of forests and carbon dioxide emissions. But few people can explain the process behind this link, and as a consequence, see climate change as a consequence of a whole hotch potch of environmentally sensitive issues. Whether this matters or not, in terms of people's ability to contribute to discussions about the climate change, is an issue we shall take up later. Our concern at this point is the way in which media coverage is reflected in public understanding.
As we have seen, media coverage does pay attention to the proposed causes of climate change (55 per cent of stories make some reference to the causes), but only in cursory way. So while greenhouse gases are mentioned in four out of ten newspaper articles, the greenhouse effect itself is rarely explained. It is perhaps not surprising then, that confronted with a list of possible causes, most people tend to respond with a rather cavalier list. Most of the issues on this list are matters of environmental concern, but some have little to do with climate change (see also Bell 1991: 239, for a discussion of knowledge of the causes of climate change).
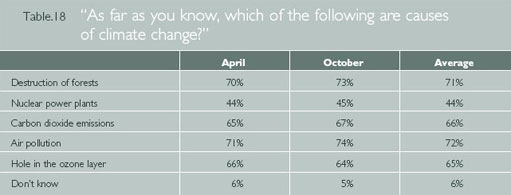
On the surface, the number of people who see the hole in the ozone layer or nuclear power plants as causes of climate change is difficult to explain: this is not, after all, a claim made in media coverage. But the fact that so many people make these links tells us something about the way people learn from the media.
Other research on the relationship between news and public understanding suggests that most people consume news rather inadvertently, and hence only take in certain aspects of a story. They also find it hard to follow the often truncated narratives of news – which unlike other stories, tends to start with the climax of a story before giving any history or background – and hence a great deal of information passes people by. The information that does stick, in this context, is often based on often repeated associations (Lewis, 1992; 2001). People then use what information they have to make sense of the world – what has been called ‘low information rationality’ (Sniderman, Brody and Tetlock, 1991) or ‘information short-cuts’ (Popkin, 1991).
In the case of climate change, this involves turning associations (between environmental problems like the thinning ozone layer and global warming) into causal links. In the last few years, media reports have often mentioned global warming and the ozone layer in the same breath:
“A new satellite which will provide scientists with a kind of health check forthe earth was launched today. The satellite, costing £1 and half billion, will orbit earth forthe next 5 years studying things like the hole in the ozone layer and global warming” (ITV News, 1st March, 2002).
“WHEN British engineers pioneered the industrial revolution and the world's first great factories 200 years ago, their eye was on progress and profit – not pollution. But scientists now believe it put us on a collision course with nature, which will see the destruction of many aspects of life on earth. Hundreds of millions of cars now spew out poisonous gases. Cities belch smoke up into the ozone layer, while distant conferences sit and discuss what to do about it. At the heart of the debate is the effect of ‘global warming’ and the ‘greenhouse effect’, caused by us producing too much carbon dioxide from burning fossil fuels. If addressed quickly enough, we might start to slow the process of the planet getting hotter” (The Daily Mirror, 29th March, 2002).
Neither of these examples assert a causal connection, and yet in the absence of any other explanation offered, most people tend to assume one. This is suggested more clearly by the response to a question asked in both surveys about the greenhouse effect. The erroneous idea that greenhouse gases effect the climate by thinning the ozone layer outnumbers correctly responses (they ‘prevent heat from escaping out of the earth's atmosphere’) by more than three to one. Bell also found that people often attributed rising temperatures to ozone depletion, which he describes as a ‘classic case of meltdown between events with similar mental scripts’ (1991: 245).
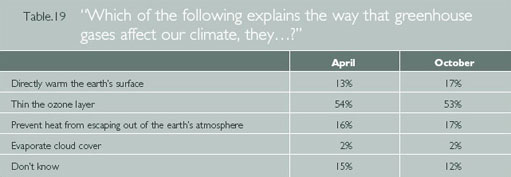
While those with more science education were more likely to get the answer right, the figure still rises to only 24 per cent for those with a formal qualification in science (GCSE or above). And the percentage of correct responses overall is notably lower than the 25 per cent who claimed to be ‘well informed’ about this issue.
One could argue that ignorance of the technicalities here are less important than a more holistic understanding of the environment. Thus, for example, one could argue that people are right to understand the thinning ozone layer and the greenhouse effect as linked, in the sense they are both environmental problems caused by industrialisation and human Activity. We shall return to this issue in our Conclusion: for the time being, what interests us about these responses is what they reveal about way media coverage (whether it means to or not) creates explanatory frameworks.
Interestingly, the age group most likely to get this particular question right was the one with the lowest scores overall – the 18–25 year olds. Those in this age group with more education did particularly well, 22 per cent those with A-Levels and 37 per cent of those with a degree answering correctly. This suggests that schools have recently included a scientific explanation of global warming in their teaching, with a considerable degree of success.
General lack of certainty about the causes of global warming is also reflected in the difficulty people have in connecting the local with the global, thereby understanding how the daily choices in their own lives might be linked to climate change. So, for example, although a number of stories linked global warming to the phrase ‘fossil fuels’, few explained what this meant, and less than two per cent of the articles mentioning climate change in our study made any reference to how the public might contribute to reducing the rate of climate change.
A rare attempt in our sample to deal with this type of issue is made by The Observer's travel editor Jeannette Hyde, as follows:
“one seat on a flight from the UK to the US is responsible for as much global warming from carbon dioxide emissions as one average driver using a car in the UK for a year” (17th April, 2002).
While it is very difficult to be definitive about environmental impacts, many climate change scientists have argued that flying goods around the world tends to involve the burning of more fossil fuels than buying local produce, thereby contributing to climate change. Since this is a good example of how people's everyday choices may have an impact on the issue, as well as one which reveals a degree of understanding of what fossil fuels are, we asked people in our surveys to make such a choice.
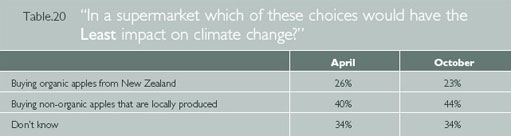
The word ‘organic’ is undoubtedly a source of confusion in this respect, since it is generally associated with environmentalism, suggesting, once again, that for around a quarter of our sample, associations may be standing in for causal relationships2. The answers do suggest, nonetheless, that more people (more than four in ten) were aware enough of the role of fossil fuels to make the hypothetical choice for local produce.
In some instances, ‘low information rationality’ does push a majority towards the correct response. The concept of a ‘carbon sink’ may have been familiar to a minority following post-Kyoto negotiations between the US and Europe, but it is not a term widely used in media coverage. Nonetheless, there was enough information in the following question for most people to work out what it meant.
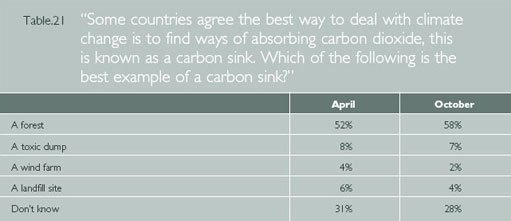
Since the association between deforestation and climate change is already well established (partly by long-running campaigns to save rain forests), ‘forests’ become the most plausible response for a majority of respondents.
Our news study also suggested that the news media pays considerable attention to the consequences of global warming, particularly in the British context. To test how widespread knowledge of these consequences is, we asked a question with a correct response that is, in some ways, counter intuitive. Hence the predicted increase in winter rainfall might seem, for some, to contradict the idea of ‘global warming’ (for British people, wet and cold weather are often seen to go together). Nevertheless, most people in both surveys gave the correct response.
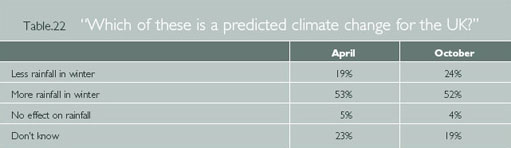
So if the news tends to ignore the processes behind global warming, it appears to be much more instructive in creating an association in people's minds between climate change and increased rainfall. This fits, once again, with news values, in which the dramatic flooding in recent years has been linked with climate change.
Climate change has become a major international political issue in recent years, and the surveys included a question to examine whether one of the main points of conflict in international negotiations on climate change is common knowledge.
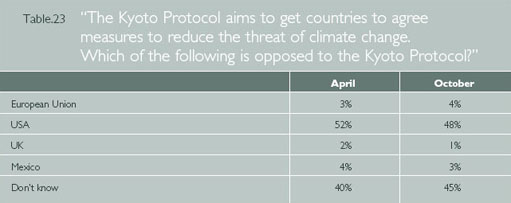
This is an issue that has received a moderate amount of media coverage, and around half our respondents get it right. Answers here might also be influenced by attitudes to the Bush presidency. What is more notable about this response is the comparative absence of incorrect assumptions. This appears to be one of those areas that people either feel they know or they don't – over 90 per cent of responses are either correct or ‘don't know’. The fact that this is unusual is indicative of the process by which people learn from news: this is one of the few questions that does not involve answers where associations people draw from media coverage might steer them in the wrong direction.
Overall, the relationship between media coverage and public understanding on this issue demonstrates both the media's power to inform and, inadvertently, to misinform. On the one hand, most people have clearly learnt a number of things from the media coverage of this issue, but the way people absorb information from the news means that they are also inclined to mistake thematic links for causal links. This, in turn, has made people concerned about climate change, but much less clear how it works.
2 We are aware that the use of fossil fuels in the production and transportation of pesticides in the production of the non-organic apples may complicate this comparison. While it is possible that those choosing the organic option were making such a calculation, we think it more likely that those who are aware of the role of fossil fuels in global warming would have picked the first option.
10.8 The media and public understanding of the MMR controversy
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
As we saw in the coverage of the story itself, the MMR issue is often compared to the BSE/CJD crisis, both stories involving potential risks to the public initially denied by both government and mainstream science. And there is no doubt that the BSE controversy framed much of the MMR coverage. Andrew Wakefield may be something of a voice in the wilderness, but, pitted against a phalanx of government officials and experts, journalists were also unwilling to discount the possibility that he may be right.
We found, first of all, that many of the key moments in the narrative did get across. Indeed, in many ways this story was the most successful of the three at communicating key themes. In particular, the specific link between MMR and autism was repeated in most stories on this issue, and most people (two out of three of our respondents in both surveys) were consequently aware of it.
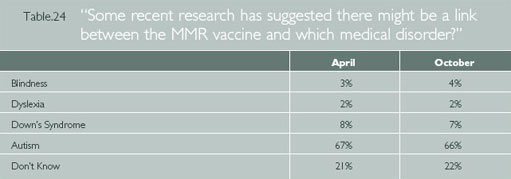
Leo Blair's role in the story was also widely covered and widely known – producing one of the highest percentages of correct answers in both surveys (66 per cent in April and 70 per cent in October)3.
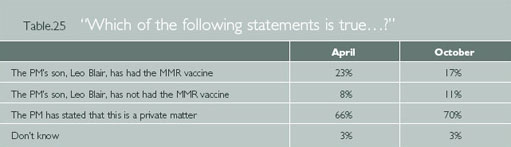
Quite why the Prime Minister's involvement produced such a high percentage of correct responses is less obvious. While mentioned in many stories (32 per cent in our sample overall), it was by no means the most prominent aspect of the coverage. It is possible that the human interest value of the Prime Minister's personal involvement in the story made this information more memorable. But we should not overlook the importance of Tony Blair's position in the story. For people confused about who to trust, this was an important indicator of the government's faith in its own position. In a nutshell, was the government's support for MMR deeply felt or merely tactical and strategic? Leo Blair might, therefore, be reasonably seen as a test of the government's confidence in its own position.
This point alerts us to the importance of narrative in communicating information. Tony Blair's involvement was significant because it came at a key stage in the narrative, made all the more compelling by the degree of suspense surrounding it4. If Leo Blair had been given the MMR vaccine, our findings suggest that the Prime Minister's refusal to disclose this information (while understandable on a personal level) was, in public health terms, a mistake. It kept open the possibility that the Prime Minister had reviewed the evidence and decided against the MMR jab, which can only have added to people's fears.5
As we have established, many media reports gave voice to both sides in the ensuing debate about the safety of the vaccine. This was sometimes a debate between scientists, and sometimes a debate between scientists or public health officials and concerned parents. The role of parents in this balancing act allowed anecdotal evidence from parents with autistic children to enter the discussion – which, while not authoritative as scientific evidence, is powerful rhetorically. Indeed, scientists or public health officials cannot have relished debating people who not only commanded immediate public sympathy, but whose own children were, apparently, testimony to the risks involved with vaccination.
If some media reports did point out that the weight of scientific evidence suggested the safety of MMR, this was not, apparently, the impression created by the coverage. When asked about the scientific evidence, many people (25 per cent in April, falling to 20 per cent in October) felt that Wakefield's speculative claim was actually backed (rather than contradicted) by most research, while the most popular response was to say that there was ‘equal evidence on both sides’.
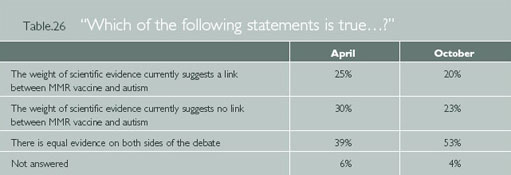
This indicates that the traditional ‘balanced’ approach taken by many reports seems to have been what lingered in most people's minds: indeed, the impression of an equally divided body of research on the controversy hardened between April and October, rising from 39 per cent to 53 per cent. This increase of 14 per cent was the biggest overall shift in our knowledge index, and suggests a degree of confusion early on in the story, with the ‘balanced’ framework becoming more dominant as the story developed.
What we see here, once again, is a distinctive pattern of learning, whereby people absorb a dominant media framework, and then use it to make suppositions. So even where reporters spell out the relative weight of evidence, as this BBC report did:
“ parents… have to decide who to trust – either the vast array of medical experts here and abroad who are convinced MMR is safe or Dr Wakefield who has the vocal support of a minority of parents” (BBC News, 7th Feb, 2002).
What appears to get heard is merely that there are two bodies of evidence. In this instance, this encourages a movement away from both the correct answer and the most obviously incorrect answer, and towards a misleading and decidedly uncertain middle ground.
Another often repeated aspect of the story – the idea that the take up of MMR was falling fairly rapidly – also seems to have hit home. When asked how much take up was falling (at a time when evidence suggested a fairly small overall decline), a plurality overestimated, with less than one in six people giving the correct response. Once again, this suggests that people are not necessarily responding to the details of media content – claims about the overall decline were rarely technically inaccurate – but to a simpler association in which the repetition of the theme of declining take-up (the third most prominent theme in our sample of the coverage) led to an assumption over-estimating that decline.
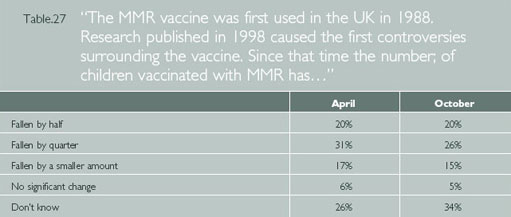
We do not know, as yet, what the longer-term implications of this story are for the decline in take-up of the MMR vaccine, although our survey offers some clues. When respondents were asked what choice they would make, about half opt for the MMR vaccine. For many respondents, of course, this is merely a hypothetical choice. Nevertheless, this does suggest that while it remains the most popular option, there has been a serious loss of confidence in the vaccine. The decline from 53 per cent in April to 47 per cent in October is, perhaps, a particularly worrying trend for public health professionals.
The ‘separate vaccines’ option – the second most recurrent theme in media coverage – is the most popular alternative, favoured by around a third of respondents in both surveys.6
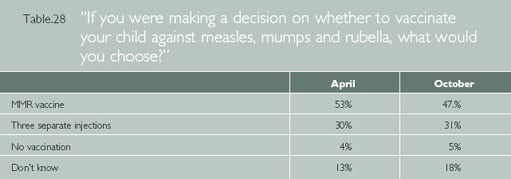
What lessons might be leaned from this? Journalists clearly felt that they acting in the public interest, while the desire to question officialdom, in whatever form it takes, is manifestly a healthy one. And the popularity of the ‘separate vaccines’ option suggests that journalists were aware of the public health risks of non-vaccination.
The problem, in retrospect, was that the debate was not, on the whole, about the key scientific aspects of the controversy. The fact that the empirical evidence provided by Dr Wakefield did not involve the vaccine at all (implicating the measles virus, not the MMR combination) received very little discussion. In short, the subsequent publicity given to the single vaccine occurred despite there being no empirical evidence to support it. The use of anecdotal evidence from a selective (and unrepresentative) group of parents might also be regarded as unhelpful for such an important matter of public policy.
These points matter, because the coverage clearly shaped the way many people understood the issue, and appears to have led to a loss of confidence in the vaccine in Britain – while confidence remains high elsewhere. And the public health consequences of an increase in measles, mumps and rubella infections are very serious indeed.7
Given the risks involved following a loss in public confidence, should journalists subject the claims of maverick scientists like Wakefield to more scrutiny before reporting them? This raises a more general question about the coverage of science, which we put to people in our October survey.
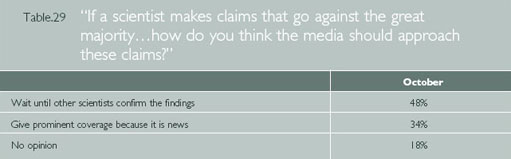
Perhaps surprisingly, nearly half felt that when scientists go against the grain (as Wakefield has), the media should wait until other studies confirm those findings before covering it. This reticence may seem odd, particularly since this issue does not involve issues of privacy, and since such work may already be in the public domain through publication in reputable journals. But it speaks to the degree to which many people feel the need for expert guidance on scientific issues. As this parent put it, writing in The Sunday Times (on February 10th): ‘I hadn't gone on the internet and surfed my way across every single website on MMR. I don't have a science degree either, so I hadn't read every study ever published in a medical journal.’ The choice, for her, came down to trusting advice from her GP, who she felt was in a better position to evaluate the evidence than she was.
This brings us, perhaps, to the difficulty at the heart of coverage of a health scare like MMR. The story appears to have created doubts in many people's minds about the safety of the MMR vaccine. And yet, unlike a decision to avoid beef, eggs or any other ‘suspect’ foodstuffs, avoiding the MMR vaccine increases the risk of potentially harmful disease. It was difficult, in this context, for most parents to know what to do for the best (other than opt or campaign for single jabs, a solution without any empirical evidence to justify it) or who they might to seek guidance from. Tony Blair's refusal to disclose his own decision on MMR, in this context, made the gap between confusion and guidance much more difficult. While for many science stories this might not be a problem, in this case there are direct consequences for public health.
For the purposes of this study, however, what is striking is how successfully the main themes of the media coverage formed the building blocks for public understanding. This was not, after all, a major, headline grabbing story. Yet the consistency of the coverage, the coherence of the narrative, and the connection to a broader public interest made much of it memorable – a point we shall take up later in the Conclusion.
3Because this question is not, strictly speaking, knowledge of science or science related policy, it was not included in our public understanding index.
4 See Lewis, 1991, for an analysis of the importance of narrative codes in communicating news.
5 One should not forgot, of course, the way in which John Gummer's attempt to assuage fears about beef by feeding his children burgers during the BSE crisis appeared to backfire. The Prime Minister's standing and image is, however, probably more credible and authoritative.
6 Although it is worth adding that respondents were not asked to pay more for this option.
7 A point graphically made in February 2002 by Dr Liam Donaldson, the Chief Medical Officer, and later by a science museum exhibition and website on the issue.
10.9 The media and public understanding of cloning and genetic medical research
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
The topic of cloning and genetic medical research has received a great deal of research in terms of the public understanding of science. The Wellcome Trust, in particular, (an independent research-funding charity that aims to improve human and animal health) has played a key role in researching public attitudes towards cloning.
Like many such studies, we found a high degree of public uncertainty. Of the three issues under scrutiny in our study, this would appear to the one most people find esoteric. While most people claimed to be ‘well’ or ‘partly’ informed about climate change and MMR, more than two thirds in our October survey (68 per cent) admitted to feeling not very well informed about this area of scientific research.
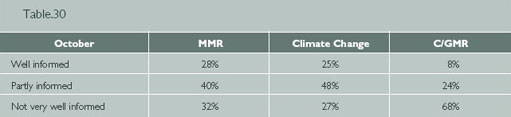
This may well be partly a response to the way the fact that this remains very much a ‘science’ story. Our media analysis suggested that the cloning/genetic medical research story is the most likely of the three to involve scientists as sources and the least likely to provoke engagement in newspaper editorials or letters pages.
Interestingly however, when asked questions about the scientific aspects of the story our respondents did not do conspicuously worse in this area than the other two. What does stand out, in terms of our knowledge index, is the consistently high number of ‘don't knows’, in response to questions on this issue. In our October survey, for example, the percentage of ‘don't knows’ in response to questions on this issue never dropped below 26 per cent (while three questions on the other two issues produced ‘don't knows’ of five percent or less). In short, if people are more confident than they should be about their knowledge of climate change and MMR, they are much more tentative about cloning and genetic medical research.
So, for example, close to half our respondents were aware that one the key developments in biotechnology in recent years has been the mapping of the human genetic code.
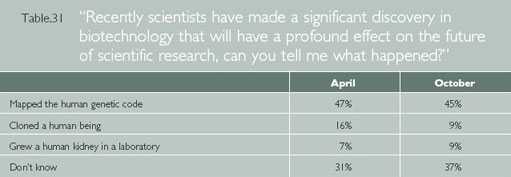
And most people are aware that the main aim of stem cell research is to create cells to research the treatment of disease.
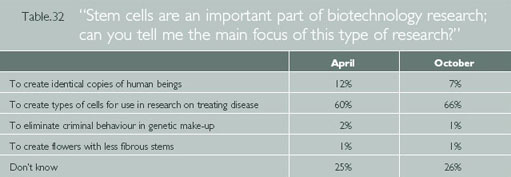
Both the questions also indicate a small but interesting shift, between April and October, away from the association with the more stereotypical images of cloning. Thus the percentage assuming that the key development in biotechnology was to have ‘cloned a human being’ dropped from 16 per cent to nine per cent, while those assuming the main focus of stem cell research was to ‘create identical copies of human beings’ dropped from 11.5 per cent to 6.5 per cent. By contrast, those associating stem cell research with the treatment of disease increased from 60 per cent to 66 per cent.
This suggests that some progress may have been made since the Wellcome Trust's 1998 report Public Perspectives on Human Cloning, which used focus groups and in-depth interviews to see how attitudes were ‘influenced by the provision of extra information’. They found that the public's acceptance of research on cloned embryos was ‘dependent on there being direct medical benefits’ – something our study suggests there is now an awareness of.
Overall, our analysis of media coverage found the presence of both the ‘concern’ and ‘great promise’ frameworks in the coverage (Kitzinger and Reilly, 1997). It is possible that while they do not appear to be capturing the public imagination, the sheer repetition of ‘great promise’ stories is beginning to seep through, thereby strengthening the association between cloning and genetic medical research and the treatment of disease.
The presence of the ‘concern’ framework, on the other hand, is most clearly revealed in relation to questions of public policy, in which public ignorance is widespread. The House of Lords decision to permit experimentation on cloned embryos in late February was covered by all the major media, and yet most people were not only unaware of this, they assumed that such things were not legal in Britain. In both surveys we asked whether the government allowed UK scientists to ‘clone human embryos’, and only around a quarter said yes (28 per cent in April, dropping to 22 per cent in October), while around twice as many (46 per cent and 48 per cent) said no.
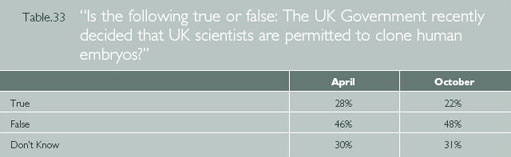
Thus not only are most people unaware of public policy in this area, the presence of the ‘concern’ framework is still palpable enough for many people to assume the government could not have sanctioned this kind of research. Indeed, in this case, recourse to the ‘concern’ framework appears to have increased slightly between April and October.
We were aware that the phrase ‘clone human embryos’ is particularly powerful in triggering the concern framework, so in October, we also asked essentially the same question using different, less obviously evocative phrasing (removing the words ‘clone’ and ‘embryo’ and substituting it with phrase ‘make exact copies of human cells’). While this did appear to reduce the assumptions of the concern framework somewhat (by around six per cent), the overall direction of responses remains the same.8
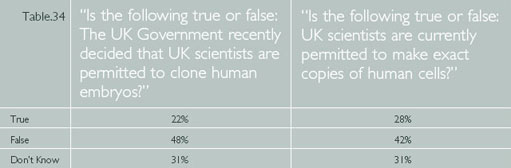
Thus it appears that while the ‘great promise’ framework informs an understanding of where the science is moving, the ‘concern’ framework comes to the fore in discussions of public policy. This suggests that many people have some way to go in connecting the realms of science and policy, the former being seen as generally positive, the latter being burdened by images of cloned human beings (a development most people clearly oppose).
Policymakers in the public understanding of science movement often argue that the more science the public knows, the more supportive they will be on this issue (a point debated in some of the academic literature). Either way, it seems likely that since most people have such little confidence about their knowledge in this area, attitudes are clearly far from entrenched. They appear to depend on whether people are thinking with the ‘concern’ framework in mind, or whether the ‘great promise’ framework is more to the fore. To test this, both surveys contained two questions to gauge people's attitudes towards genetic science. In April, these were asked first; whereas in October, they were both deliberately placed immediately after the question in which a majority had stated that the main aim of stem cell research was the treatment of disease.
What we found was that a fairly small change in question order produced a significant shift in response away from the concern framework towards the great promise notion. In the first survey, when asked out of the blue, ten per cent more people found these trends worrying than encouraging. In the second survey (two thirds having just answered a question linking genetic research to the treatment of disease), the change in context appears to reverse the response, with ‘encouraging’ outscoring ‘worrying’ by nine per cent.
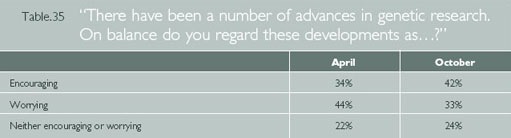
Similarly, the number of people concerned about the regulation this research drops by 12 per cent in the second survey, from 50 per cent to 38 per cent.9
In both cases, it appears that the more knowledge people have of the overall drift of this research, the more encouraged they are by developments in this area. This is confirmed when we break down responses to these questions. In the April survey, for example, when most people were more worried than encouraged, those with any science education were 19 per cent more likely to find the research ‘encouraging’ rather than worrying. (54 per cent versus 35 per cent).
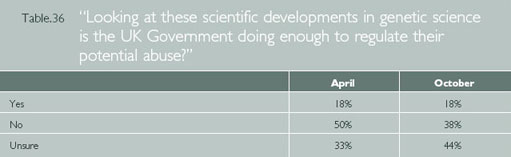
This does not mean that the media or the public have no cause for concern: the ethical boundaries of such research are clearly important matters for public discussion. What matters here is that the concerns people have are based on a broad understanding of the risks and potential of medical science. And despite people's lack of confidence about their knowledge of this issue, our survey suggests that the coverage has reported the medical benefits of such research and that this coverage shows signs of forming part of the public understanding.
The challenge, for scientists, policy makers and journalists, is to move away from the dichotomies of the great promise and concern frameworks towards a more integrated approach, whereby we can decide what kind of scientific research we should support and which we should not. To this end, we would make the following suggestions:
-
Scientists, policy makers and journalists should find ways of engaging the public more in this story without resorting to ‘wacky science’ stories about things such as the cloning of prehistoric creatures. Some television and newspaper articles, for example, have attempted to inject stories about the medical science with human interest.
-
At the same time, there is still much to be done before people feel confident about this issue. While media – including the tabloids – have attempted to explain the science (and to connect the dots between words like ‘stem cells’ and ‘cloning’), these points will bear a great deal of repetition if the public are able to construct a coherent set of associations with which to make sense of it all.
8 Ignorance of policy in this area was also reflected in a question about the ownership of genetic information, only a quarter of respondents being aware that such information is in both the public and private domain.
9 Needless to say, in both surveys most people are clearly unaware of what the Government is or is not doing, and their answers must be seen in that context.
10.10 Conclusions
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council.
We now return to three questions central to our inquiry. First, what do we, as a public, need to know about climate change, MMR and genetic media research? Second, what have most of us learnt from media coverage about these issues? And third, to what extent does our study suggest a model of media and public understanding which might be used to create a more informed public? Since the science based stories we have tracked each have their own distinctive features, we will begin by considering them case by case, before suggesting some more general Conclusions.
Climate change is part of a long running news story, told by a mix of scientists, politicians, environmentalists and interest groups. If the idea of the greenhouse effect in causing global warming was once seen as controversial, we now see the weight of scientific opinion confirming it. This movement towards consensus is generally reflected in media coverage (with a few dissenting voices).
Media coverage of climate change often refers to its causes, and there is a fairly high degree of public awareness that human activities such as deforestation and fossil fuel emissions are said to cause climate change. What is less apparent in news coverage is a focus on the scientific process involved, such as the nature of the greenhouse effect. The absence of this explanation is reflected in public understanding: most people clearly don't know what the greenhouse effect is or how it works.
This is not, perhaps, surprising. What is more interesting is how people use information to construct an explanation. Ideas with little media presence – such as the mechanics of the greenhouse effect – are unlikely to filter through, and yet many people still feel able to make knowledge claims. They appear to do so on the basis of the presence of often repeated associations in media coverage: in this case, between the thinning ozone layer and the greenhouse effect. Thus what is, in media coverage, merely a juxtaposition (under the general heading of human-made environmental problems) undergoes a cognitive leap in public understanding, so that it is understood as a casual relationship.
Many scientists would feel that this is a problem, and that people ought to know the simple mechanics of the greenhouse effect. But does it really matter if they don't? From the perspective of democratic citizenship, it could be argued that such knowledge is unnecessary. For citizens to understand and act on the issue, they only need to be aware of the causes and consequences of climate change, so that they are in a position to judge what measures might be taken to combat it.
On this count, our study does suggest that certain repeated themes about causes and consequences are filtering through, although there is also a degree of confusion that appears to come from lumping environmental problems together. This may make it difficult for many people to judge the specific merits of climate change proposals. Some policy makers might argue, for example, that the connection many people make between nuclear power and climate change is fallacious and thus profoundly unhelpful.
But one could also argue that if people are somewhat undiscriminating in their assessment of the relationship between environmental problems – from air pollution to nuclear waste – the rather muddled picture that emerges does have a certain coherence. Most people are able to make links between a range of human activities that have a negative environmental impact. If past generations happily embraced industrial consumerism in blissful ignorance of the environmental consequences, they no longer do so with quite the same disregard.
And yet it remains questionable how far this awareness translates into active citizenship. Most people, when prompted, express concern about climate change and felt the government should do more to tackle it. However, when polls ask people to say, unprompted, which issues concern them, environmental issues barely register (in a Mori survey in December 2002, environmental issues came 19th on the list of issues facing Britain, below trade unions and inflation). In this context, we would suggest that if there is a gap in media coverage and public understanding of climate change, it is not a simple absence of scientific understanding. The problem, we would suggest, is more a question of emphasis.
Firstly, while the predictions coming from the UN committee on climate change (amongst others) are dramatic and catastrophic, most of the misery is likely to fall on countries in the third world. The effects of climate change on Britain are seen as far less alarming. While the media often discuss the consequences of climate change, media coverage on this issue – as on many others – is often somewhat parochial, with many casual references to its more benign effects. This may explain why the issue of not generally seen as as important. This may also partly explain why broadsheet readers, whose newspapers have a more international focus, are more concerned about this issue. The challenge here is to make the sheer scale of potential global damage that climate change may inflict a major and recurrent news story. An emphasis upon the specifics of the science of global warming is not likely to be especially helpful in this context.
Second, most people need practical rather than technical information. The widespread use of scientific shorthand – notably terms such as ‘greenhouse gases’ or ‘fossil fuels’ – assumes rather than communicates an understanding of the causes of climate change. At the risk of simplifying the complexities of environmental impacts, it would be more helpful to use more direct language, to specify the kinds of activities that most contribute to climate change and what might be done to limit them.
Of the three stories we looked at, the MMR debate most clearly became a news story in its own right. The story's script was undoubtedly influenced by the ghost of the BSE controversy. Was this another case, reporters’ asked, of mainstream science and the government rushing prematurely to the defence of the status quo? The story followed a widely repeated pattern, in which a maverick researcher and concerned parents questioned scientific officialdom, with the Prime Minister and his young son becoming personally involved as the government resisted calls, amidst declining public confidence, to offer an alternative to the MMR jab.
Our study revealed that the main elements of this story – the alleged link between MMR and autism, the Prime Minister's refusal to disclose whether his son Leo had been given the MMR jab and subsequent the fall in public confidence -became widely known. Indeed, the extent of public knowledge on this issue demonstrates the power of the news media to inform. What made this story stick, we would suggest, was the consistency of the messages across different media and the speed with which it became a matter of public interest rather than simply a debate between scientists.
The downside, in this instance, was that the overall framework used to tell the story was so powerful that it created a perception of a divided scientific community with two conflicting bodies of research. This perception was undoubtedly exacerbated by Tony Blair's refusal to comment, which, however justified, made the Government's endorsement of the MMR jab ring hollow. Most people were thus unaware of the flimsiness of the link between MMR and autism (based, as it is, on a speculative claim rather than any empirical research) and that the great weight of research has failed to find any such link.
There is much to debate here about the media coverage of an issue in which a decline in public confidence (unlike the BSE case) actually creates new public health risks from outbreaks of measles, mumps or rubella. It seems fair to say, in retrospect, that the scrutiny of those supporting MMR was not matched by a rigorous examination of the case against it. Our main concern here, however, is what it tells us about the role of the media in public understanding. In short, the consistent telling of a story – particularly one with echoes of other stories – clearly influences public understanding.
And it is the broad themes of the coverage – rather than the details – that establish the building blocks for people's understanding and opinions. There are also important questions about the way in which the government and others arguing in favour of the single jab pursued their argument. Did they make best use of individual and ‘emotive’ cases, like their opponents. Were scientists willing to set aside their distaste for the cruder aspects of the debate in order to convey their point of view not only clearly, but consistently and repeatedly?
We saw much less consistency in the media coverage of cloning and genetic medical research. Coverage here, by contrast with MMR, tends to be dichotomous, focusing on either the medical potential of stem cell research or the ethical risks associated with cloning. The ‘great promise’ or ‘concern’ frameworks both have their own well-rehearsed conventions, one focusing on cutting edge medical breakthroughs and the promise of healing currently untreatable conditions, the other pointing with alarm to the Frankenstein excesses of irresponsible scientists. Accordingly, although many people confess to a lack of confidence about this issue, they appear to be aware of both potential and risk.
When it comes to public understanding of Government policy on this issue, our survey suggests widespread ignorance of what is or is not permitted – even though the House of Lords ruling on this issue in 2002 was given modest but fairly widespread media coverage. Indeed, public ignorance on this issue demonstrates the extent to which details of a story can pass people by. As we have seen with the other two stories, public understanding comes from the generality of often repeated media frameworks rather than one-off stories.
Are the public well informed enough to contribute to the debate about what the Government should sanction in this field? Since public opinion on this issue is clearly influenced by the context in which it discussed (we were able to manufacture a significant shift towards an optimistic view simply by a small alteration to the order in which we asked questions), it would not appear to particularly well-grounded. And yet surely this is an issue in which society as a whole – rather than a group of experts – should decide where to draw the line?
The irony is that this was, in many ways, the most science-driven story of the three we looked at. It was much more likely to be reported by a science or specialist correspondent, and much more likely to include scientists as sources. And although there were more stories, overall, on this issue than the other two, the public don't feel informed as a consequence. What this strongly suggests is that more science in the media does not leads to greater public understanding. On the contrary, it may be that, for better or worse, the best way to engage the public is actually to make it less of a science story.
What emerges from our analysis of all three stories is a much clearer sense of the relationship between the media coverage of science and public understanding.
-
The news media clearly play a role in informing the way people understand science. Our study suggests that most people are aware of the main themes or frameworks of media coverage of science related stories. Information that is subsidiary to these themes, be it part of the background to a story or information that does not recur (such as the passing of legislation) is unlikely to get across.
-
These themes or frameworks are then used as building blocks for people to make sense of an issue. This can, in practice, be a fairly crude cognitive process, and while these building blocks can be put together in ways that facilitate public understanding, many people ignore the fine print and assume connections between things simply because they are often juxtaposed in media coverage. Similarly, a journalistic convention (such as the balancing of two views) may, if repeated often enough, be interpreted literally as reflecting parity of research evidence.
-
People are more likely to become engaged in a science story if it appeals to a broader public interest. This is particularly the case if the story has a straightforward and consistent narrative (as the MMR story did). In these cases, key moments in the narrative (such as Tony Blair's reluctant role in the MMR story) may be especially significant in public understanding.
-
We find little evidence to support the idea that the presence of more science, scientists and science specialists in the media will increase the public understanding of science. On the contrary, a ‘science for science's sake’ approach seems the one least likely to generate public engagement and therefore public understanding.
-
Following on from this, we would suggest that the idea of public interest is central to engaging the public in science stories. We need to ask what it is important for citizens to know about science in a democracy. In short, why should people be interested in science if what they think has no effect on a broader policy level? If there is to be greater public accountability in support for science – which most people say they want – it is therefore important to establish what kind of information is necessary for people to make a valid contribution. What matters here, we would suggest, is not so much the science itself, but establishing clear connections between science, policy and the broader public interest.
11 Reading 4: The lessons of MMR
11.1 The lessons of MMR
Horton, R. (2004) ‘The lessons of MMR’, The Lancet, 363, 6 March 2004, pp 747–749 Elsevier. Copyright © 2004 Elsevier.
This week, The Lancet prints a partial retraction – a retraction of an interpretation1 – from the majority of authors of a paper published in February, 1998, by Andrew Wakefield and colleagues.2 Wakefield and one other co-author, Peter Harvey, have not signed this retraction statement. We hope to publish their response very shortly. The original report2 made clear that the authors “did not prove an association” between measles, mumps, and rubella (MMR) vaccine and a newly described syndrome of bowel disease and autism. But the authors did raise the possibility of a link, on the basis of parental and medical histories, and they suggested that “further investigations are needed to examine this syndrome and its possible relation to this vaccine”. This interpretation of their data, together with a suggestion made by Wakefield during a separate press conference held at the Royal Free Hospital that there was a case for splitting the MMR vaccine into its component parts, triggered a collapse in confidence in the UK's MMR vaccination programme. It is the interpretation expressed about a connection between the vaccine and the new syndrome that is now being retracted. Today's retraction comes after debate following the release of new information 2 weeks ago about the circumstances surrounding the publication of this work.3 An enormous amount of effort has gone into reviewing and analysing the events before and after publication of the 1998 article. It is now time to look forward.
11.2 Autism research
Horton, R. (2004) ‘The lessons of MMR’, The Lancet, 363, 6 March 2004, pp 747–749 Elsevier. Copyright © 2004 Elsevier.
In 1943, Leo Kanner described 11 children with a condition that differed “markedly and uniquely from anything reported so far”.4 He believed that the characteristics of these children, the fundamental feature of whom was their “inability to relate themselves in the ordinary way to people and situations from the beginning of life”, constituted a syndrome, one that he described as “an extreme autistic aloneness”. The recognition of such a distinct clinical entity was important, even urgent at that time. Kanner described how several of the children who had been introduced to him were inappropriately labelled as “idiots or imbeciles”. One lived in a “state school for the feebleminded, and two had been previously considered as schizophrenic”.
Since Kanner's report, autism and autism-like conditions have become common diagnoses5 and exercise much media attention.6 There is a strong underlying genetic basis to autism. But the idea of a “late-onset” variant7 raised a possibility that there might be psychological and organic factors contributing to autism's cause and course. One unexpected consequence of the debate surrounding MMR has been a redirection of public attention to a condition that has often been neglected by medicine. In a review of the epidemiology and causes of autism, for example, the UK's Medical Research Council (MRC) summarised existing knowledge and identified strategic themes deserving further investigation (panel).8 There are large and surprising gaps in our knowledge of a condition that affects as many as 6 per 1000 young children.
The UK Government announced a further £2–75 million of new and ring-fenced money for autism research in 2002. The first funding decisions by the MRC are expected in May this year. The MRC is strongly committed to autism research, presently funding seven research projects at a cost of over £4 million. To make the best of what are still limited resources, it is important that the Council's steering group set up to implement the findings of its 2001 report, together with other major national and international grant-giving bodies, establish a funders’ forum for autism research to fine-tune strategy and avoid unnecessary duplication of research effort. The UK Government should extend its initial and welcome commitment to autism by pump-priming research with a further ring-fenced lump sum to the MRC of at least £12.5 million – £2.5 million annually over 5 years. Such sustained investment is vital if properly designed longitudinal studies to examine genetic and environmental factors in autism are to be constructed. Compare these modest sums of funding, for example, with the US National Institute of Health's budget for autism research of $70 million by 2003. NIH is also committed to creating STAART (Studies to Advance Autism Research and Treatment) centres – eight of which have been launched in the past 2 years, at a cost of $65 million, spread over 5 years. This approach might well have merit in the UK.
Future strategic themes in autism research8
-
Case definition: Improving phenotypic identification
-
Epidemiological frameworks: Pinpointing environmental and genetic influences
-
Integrated research strategies: Developing a comprehensive neurosciences approach
-
Hypotheses about abnormal physiology: Requiring experimental rigour and independent replication
-
Research capacity and the service interface: Promoting collaboration, career development, and child-care and support service expansion
-
Lay participation: Strengthening research networks through partnership
11.3 Research integrity
Horton, R. (2004) ‘The lessons of MMR’, The Lancet, 363, 6 March 2004, pp 747–749 Elsevier. Copyright © 2004 Elsevier.
The latest debate surrounding Wakefield and colleagues’ paper has been enormously confusing. Public inquiries have been sought into the way ethics committees operate, how the legal services commission makes its decisions, and even, once again, into the safety of vaccines. A preliminary investigation by the UK's General Medical Council is underway. A furious debate about the actions of almost all protagonists has taken place. The press has become the courtroom for this very public dispute. But the media cannot be the only place to charge, investigate, prosecute, defend, judge, and pass verdicts on those who have been accused of research misconduct.
In 2000, a group representing the UK's Committee on Publication Ethics (COPE) drew attention to a collective institutional failure to take allegations of research misconduct seriously.9 The absence of formal mechanisms within many universities and at a national level to investigate claims with visible due process means that publicly aired allegations leave everybody involved scrambling to respond in the best way they can. COPE has produced helpful guidance on how to deal with allegations of misconduct. But with no national body to which one can refer these allegations, the danger is that in any ensuing media furore good people are hurt by smear and innuendo. The appearance of institutions investigating themselves, while accepted as the norm in science and medicine, does little to strengthen public trust in a system that has such critical societal influence, and thus which requires transparent lines of accountability.
Present scientific and medical institutions have failed to act after years of encouragement and embarrassment. It is now up to Government to step in to create Britain's first Council for Research Integrity. Please, ministers, do so and do it now.
11.4 Vaccine safety
Horton, R. (2004) ‘The lessons of MMR’, The Lancet, 363, 6 March 2004, pp 747–749 Elsevier. Copyright © 2004 Elsevier.
In a review of the unintended effects associated with MMR, Jefferson and colleagues10 found that the reporting of safety outcomes in MMR vaccine studies was inadequate. Here is a constantly repeated scenario in health-technology assessment (another example: the row over the safety of calcium-channel blockers). A product undergoes limited testing for efficacy and safety. It is licensed. A signal of concern is thrown up.
There is no valid set of safety data to which one can turn to answer these queries. Public concern grows and confidence in the technology may be jeopardised. Appropriate studies are hastily completed to confirm or refute the original signal of potential risk. An answer eventually comes, but too late to have prevented a great deal of anxiety.
Jefferson has suggested a solution to this problem.11 He recognises that vaccines pose particular challenges to investigators given their frequently universal coverage, which precludes the possibility of any controlled long-term experimental assessment. Instead, he proposes creating a library of evidence, drawing together widely dispersed data from published papers, manufacturers’ technical reports, and researchers’ personal files. In this way, loss of crucial information would be minimised and gaps in existing evidence could be identified and filled early on. This idea is sensible and deserves further consideration.
11.5 Public engagement
Horton, R. (2004) ‘The lessons of MMR’, The Lancet, 363, 6 March 2004, pp 747–749 Elsevier. Copyright © 2004 Elsevier.
Many doctors and public-health officials have been frustrated by the debate over MMR. I have shared this frustration. One newspaper fancifully called our recent statement about the 1998 Lancet paper part of an “orchestrated campaign” to bolster MMR programmes.12 In fact, the events leading to today's partial retraction were sudden, sparked by an investigation by a newspaper, The Sunday Times. Our response was to determine answers to very specific allegations. We have had no contact with anybody at the Department of Health or elsewhere in Government, vaccine manufacturers, or lawyers involved in ongoing litigation. There was no orchestrated campaign.
But there are fair questions to be asked about the style of government and expert response to claims about the safety of MMR. Three reactions have been discernable. First, there has been an appeal to evidence. The Department of Health's http://www.mmrthefacts.nhs.uk website contains a superb collection of materials designed to help parents make the “decision in your own time and on your own terms”. The difficulty is that in a post-BSE era, where government advice is no longer immediately taken on trust, the weight of accumulated evidence carries less force if it comes from government than it once did.
Second, public-health officials have disparaged as “poor science” evidence that appears to contradict their official message. This approach has a cost. The reason that today's retraction is partial and not total is that the discovery of a possible link between bowel disease and autism is a serious scientific idea, as recognised by the MRC,8 and one that deserves further investigation. Although dismissing the entire 1998 Lancet paper as poor science gives a clear and correct message to the public about the status of any claim regarding the safety of MMR, in scientific and clinical terms it is both wrong and damaging. The autism-bowel disease link was considered part of a series of physiological observations judged by the MRC to be “interesting and in principle worth investigating”. Subsequent research has yielded conflicting findings.13, 14 This work should be supported.
Third, there has been an effort to starve critics of legitimacy by refusing to engage them face-to-face. For example, when the drama Hear the Silence was broadcast on British television in December last year, there was a boycott of a subsequent discussion by many of those who could have best articulated the case for MMR. The reason advanced was that rational debate would not change the minds of an extreme few who believed MMR to be unsafe no matter what the evidence presented to them. Also, the composition of the panel discussion did not reflect the large measure of consensus that MMR is safe. Instead, it portrayed the issue as a finely balanced scientific exchange, when in truth there is very little scientific uncertainty.
How should we debate and discuss matters of public health concern? Certainly, with all the evidence before us. But perhaps this evidence is best provided by neutral and trusted third parties – not the Government. In the UK, one might turn to the Consumers’ Association, which publishes the respected Drug and Therapeutics Bulletin. Certainly, with strong public-health messages. But care must be taken not to dismiss important work that deserves continued support. And certainly robustly. But also directly, recognising that wider public trust is best fostered neither by referring to abstract evidence alone nor by official pronouncements of reassurance, but by explaining face-to-face15 in transparent, human, even anecdotal terms with personal stories, why a particular course of action is being advocated.
Persuading the public to support vaccination is not only a matter of winning an argument. It is also about understanding the reasons why parents are and are not inclined to take their children for immunisation.16 The complexity of this decision demands a more nuanced response from the public-health community than it has so far received.
11.6 Publishing controversial new ideas
Horton, R. (2004) ‘The lessons of MMR’, The Lancet, 363, 6 March 2004, pp 747–749 Elsevier. Copyright © 2004 Elsevier.
It seems obvious now that had we appreciated the full context in which the work reported in the 1998 Lancet paper by Wakefield and colleagues was done, publication would not have taken place in the way that it did. These are difficult judgments to make in hindsight. For example, our sensitivity to potential conflicts of interest is very much higher today than it was in 1998.17-19 What we will not do is to become profoundly conservative in our decision making about original ideas. A forum to raise new and sometimes unpopular thinking, even on the basis of what at first might appear flimsy evidence, is important20– and often vitally so for clinical medicine and public health.21 How we discuss this new thinking then becomes the central question to answer,22 not whether we should publish it or not.
Information that once could be confined to a small community of professionals is now open to wider distribution and comment – accurately or otherwise. No matter how many qualifying phrases or parallel reassuring editorials an editor might run, a new finding or a controversial claim is impossible to control. This places great responsibility on editors, scientists, and press and public-relations professionals to avoid encouraging anybody to go beyond the data or interpretations described in a paper. It is the job of journalists to tempt scientists to do otherwise. But we can all do better to adjust the volume of our message according to the validity of the information before us. Editors have a responsibility to be involved in all aspects of a paper's dissemination, whether in the pages of a medical journal or on the platform of a press conference.
Finally, what of the calls for a public inquiry into this entire affair? An inquiry would certainly provide an opportunity to investigate, once again, all the issues that have made this matter such a troubling one for so many. To that extent it would be welcome. But public inquiries are easy to demand, and less easily able to deliver on expectations. They can sometimes entrench division rather than relieve it. Would it not be better to create a more positive process that emphasises reconciliation, progress, and partnership? A collaborative consultation, perhaps, between equals: members of the autism lay community (including parents and possibly in conjunction with the Consumers’ Association, which has a strong interest in public information and, through the DTB, MMR23), clinicians responsible for the care of children with autism and related disorders, the MRC, and the Health Protection Agency. Call it, say, “MMR and autism: learning the lessons”. For there are, indeed, lessons to be learned.
Richard Horton
11.7 References for Reading 4
Horton, R. (2004) ‘The lessons of MMR’, The Lancet, 363, 6 March 2004, pp 747–749 Elsevier. Copyright © 2004 Elsevier.
-
Murch, SH, Anthony, A, Cassen, DH, et al. ‘Retraction of an interpretation’. Lancet 2004; 363:750.
-
Wakefield, AJ, Murch, SH, Anthony, A, et al. ‘Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children’. Lancet 1998; 351:637–41.
-
Horton, R. ‘A statement by the editors of The Lancet’. Lancet 2004; 363: 820–21.
-
Kanner, L. ‘Autistic disturbances of affective contact’. Nervous Child 1943; 2: 217–50.
-
Volkmar, FR, Pauls, D. ‘Autism’. Lancet 2003;362:1133–41.
-
Goode, E. ‘Autism cases up; cause is unclear’. New York Times Jan 26, 2004: A1.
-
Volkmar, FR, Cohen, DJ. ‘Disintegrative disorder or “late onset” autism’. J Child Psychol Psychiatry 1989; 30:717–24.
-
MRC review of autism research: epidemiology and causes. London: MRC, 2001.
-
Farthing, M, Horton, R, Smith, R. ‘UK's failure to act on research misconduct’. Lancet 2000; 356:2030.
-
Jefferson, T, Price, D, Demicheli, V, et al. ‘Unintended events following immunisation with MMR: a systematic review’. Vaccine 2003; 21:3954–60.
-
Jefferson, T. ‘Informed choice and balance are victims of the MMR-autism saga’. Lancet Infect Dis 2004; 4: 135–36.
-
Editorial. ‘This orchestrated campaign must not be allowed to stifle real debate on MMR’. The Independent Feb 24, 2004: 16.
-
Torrente, F, Anthony, A, Heuschkel, RB et al. ‘Focal enhanced gastritis in regressive autism with features distinct from Crohn's and Helicobacterpylori gastritis’. Am J Gastroenterol (in press).
-
DeFelice, ML, Ruchelli, ED, Markowitz, JE, et al. ‘Intestinal cytokines in children with pervasive developmental disorders’. Am J Gastroenterol 2003; 98: 1777–82.
-
Shapin, S. A social history of truth. Chicago: University of Chicago Press, 1995.
-
Roberts, KA, Dixon-Woods, M, Fitzpatrick, R, Abrams, KR, Jones, DR. ‘Factors affecting uptake of childhood immunisation: a Bayesian synthesis of qualitative and quantitative evidence’. Lancet 2002; 360: 1596–99.
-
Davidoff, F, DeAngelis, CD, Drazen, JM, et al. ‘Sponsorship, authorship, and accountability’. Lancet 2001;358: 854–56.
-
James, A, Horton, R. ‘The Lancet policy on conflicts of interest’. Lancet 2003;361: 8–9.
-
James, A, Horton, R, Collingridge, D, McConnell, J, Butcher, J. ‘The Lancet's policy on conflicts of interest-2004’. Lancet 2004; 363:2–3.
-
Editorial. ‘Dissent must be aired’. Times Higher Educational Supplement Feb 27, 2004: 14.
-
McBride, WG. ‘Thalidomide and congenital abnormalities’. Lancet 1961; ii: 1358.
-
Calman, KC. ‘Communication of risk: choice, consent, and trust’. Lancet 2002;360:166–68.
-
Anonymous. ‘MMR vaccine-how effective and how safe?’ Drug Ther Bull 2003; 41: April, 1–6.
Keep on learning

Study another free course
There are more than 800 courses on OpenLearn for you to choose from on a range of subjects.
Find out more about all our free courses.
Take your studies further
Find out more about studying with The Open University by visiting our online prospectus.
If you are new to university study, you may be interested in our Access Courses or Certificates.
For reference, full URLs to pages listed above:
OpenLearn – www.open.edu/ openlearn/ free-courses
Visiting our online prospectus – www.open.ac.uk/ courses
Access Courses – www.open.ac.uk/ courses/ do-it/ access
Certificates – www.open.ac.uk/ courses/ certificates-he
Newsletter – www.open.edu/ openlearn/ about-openlearn/ subscribe-the-openlearn-newsletter
References
Acknowledgements
The author would like to acknowledge with gratitude the advice and assistance of Julia Garritt, Felicity Mellor, Jeff Thomas and Christine Marshall in bringing this case study to fruition.
The material acknowledged below is Proprietary (see terms and conditions) and is used under licence (not subject to Creative Commons licence).
Grateful acknowledgement is made to the following sources for permission to reproduce material:
Course image: UMDNJ School of Nursing in Flickr made available under Creative Commons Attribution-NonCommercial 2.0 Licence.
Fitzpatrick, M. (2004) MMR and Autism, Routledge. Copyright © 2004 Michael Fitzpatrick;
Bellaby, P. (2003) ‘Communication and miscommunication of risk: understanding UK parents' attitudes to combined MMR vaccination’, British Medical Journal, 327, 27 September 2003, pp. 725–28. Reproduced by permission from the BMJ Publishing Group; Mary Evans Picture Library Ltd; P A Photos;
Hargreaves, I., Lewis, J. and Speers, T. ‘Towards a better map: Science, the public and the media’, Economic and Social Research Council;
Horton, R. (2004) ‘The lessons of MMR’, The Lancet, 363, 6 March 2004, Elsevier. Copyright © 2004 Elsevier.
Every effort has been made to contact copyright holders. If any have been inadvertently overlooked the publishers will be pleased to make the necessary arrangements at the first opportunity.
Don't miss out:
If reading this text has inspired you to learn more, you may be interested in joining the millions of people who discover our free learning resources and qualifications by visiting The Open University - www.open.edu/ openlearn/ free-courses