Challenging ideas in mental health
Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Saturday, 13 June 2026, 5:31 PM
Challenging ideas in mental health
Introduction
This free course, Challenging ideas in mental health, takes you on a journey of discovery where you are invited to challenge ideas, both new and old, in relation to mental health. It is made up of a series of three sections. The first section, ‘Boundaries of explanation’, sets out the theme of boundaries: boundaries within and between groups; within and between explanatory frameworks; and within and between experiences of mental health and distress. The second section, ‘Whose risk is it anyway?’, considers a critical account of the increasing focus on risk (particularly risk to others) in policies and professional practice in the last 40 years. The third section, ‘The business of madness’, looks at two controversial areas of mental health: the growth of mental health as a business, driven in part by market forces, and the profit motive.
This OpenLearn course provides a sample of Level 2 study in Health and Social Care. You might be particularly interested in the Open University course K240 Mental health and community.
Learning outcomes
After studying this course, you should be able to:
understand the complexity and dilemmas of diverse perspectives in the field of mental health and distress
understand the importance of service users/‘survivors’ experiences and perspectives
understand how mental health issues can affect everyone
understand the range of potential risks faced by service users/‘survivors’ in their everyday lives.
1 Boundaries of explanation
This section looks at what we are calling ‘boundaries of explanation’. It tackles key issues such as:
What are mental health and distress – and who decides or defines these?
What are the views of people who have acquired a label or have been diagnosed with a ‘mental illness’?
What are the views of those who determine – and often ‘patrol’ – the boundary between mental distress and ‘normality’?
The section looks at language and terminology and the differences between people. It looks at medical and social models, and some of their competing claims, and introduces a holistic model which embraces key aspects of both approaches.
1.1 Boundaries of exclusion
The first idea to come under critical consideration is that of boundaries. Boundaries can be helpful and, indeed, we use them here as a means of exploring different, and competing, explanations of mental health and distress. However, they can also be limiting and excluding, emphasising the differences between people, some of which run very deep. At their simplest, boundaries put limits on tasks so that they appear manageable. They help to mark out personal space in a shared office, or indicate the extent of someone’s home and garden. Boundaries are often physical, represented by partitions or walls or fences, to show who is allowed in and who is not (and under what terms).

The sorts of boundaries we consider here are more social than physical. They also define ‘who’s in and who’s out’.
In many ways, social boundaries are the most pervasive. That is because they can serve to exclude people who look or behave differently, and they are much harder to shift than a single garden fence.
1.1.1 Boundaries and terminology
In another context Shakespeare asked, ‘What’s in a name?’, and suggested by way of an answer that a rose may smell as sweet whatever it is called. In the context of social boundaries, however, the language used is actually very important in determining ‘who’s in’ and ‘who’s out’.
Activity 1: Looking at language
What is the language of mental distress? Who are the people who experience it?
Make a list of all the words you can think of (in past as well as present usage and including colloquial and slang words) that describe the condition or experience of ‘mental distress’. Then list the words used to refer to the people who have a ‘mental health condition’ or illness, again including slang terms.
Then read the influential earlier views of Dr Rachel Perkins OBE and Professor Diana Rose (Readings 1 and 2 below) and write a short summary of the authors’ views on language and terminology.
Discussion
Your list may have contained some or all of the following terms: lunacy, mania, madness, insanity, mental ill health, mental illness, mental distress, mental health problems. More specifically, you may have mentioned schizophrenia, depression, anxiety, neurosis and paranoia. You may have also suggested possession and witchcraft, as these can be associated with mental ill-health.
The two authors of the readings are themselves users of mental health services as well as being involved in mental health research and practice. Perkins dismisses the word ‘distress’ as being too inclusive. Her argument is that everyone experiences distress but not everyone experiences ‘madness’, and to claim they do is to diminish and trivialise the latter experience. She suggests that service users should ‘embrace mad pride’ and celebrate their differences. Rose accepts that some service users regard their experience as an illness that can be treated. She argues, however, in favour of the term ‘mental distress’. At the same time, she suggests that this should be linked with a more positive outlook that includes valuing and learning from that experience, and connecting it with ‘the discourse of rights’.
What are we to make of this? One conclusion to be drawn is that there are no easy answers to the question of what terminology to use, nor any ready-to-use terms that are acceptable to everyone and these may be culturally dependent. However, this course aims to draw on these accounts – and the accounts of others – to use language that is acceptable and meaningful. This probably means using ‘mental distress’, but not in a way that demeans or trivialises. Instead, it means taking a positive stand – celebrating difference and diversity, valuing people’s experiences of mental distress and supporting their rights, especially their right to be included in the mainstream of society.
1.1.2 Boundaries of difference
One of the things that language does is define and give a name to differences between people – to delineate the boundaries that separate them. In the mental health field, the ‘mad’ are at one end of the social divide that separates the ‘normal’ from the ‘abnormal’. They are ‘the other’, a point made in the article by Perkins in the previous section: ‘To be mad is to be defined as “other”’.
This is a recurring theme in the mental health field. In the following passage Abina Parshad-Griffin, who at the time was the Chair of the Mental Health Action Group for the Disability Rights Commission (DRC), reflects on ‘otherness’ and what it means to be ‘the other’:
I could use different aspects of who I am that make the whole of me, as a kind of through-the-looking-glass. And I can give an example: being mixed race, if I had to fill in different forms in various countries, I’d have to tick different boxes. So in South Africa, I would have been ‘coloured’. In America, I would be ‘black’ because one drop of Black blood makes you ‘black’, and excluded. In South America, I could possibly be ‘mixed race’, or I could even pass for ‘white’ when you have the hierarchy of colour coding. But guess what I’m called in England or the UK? ‘Other’. And it’s that otherness that is part of my identity, and I believe that mental health discrimination is that otherness which is sometimes indefinable. But you pick it up – this overt and covert discrimination. I call it ‘psychophobia’: fear of mental illness. And there are certain conditions. Like somebody asks me, ‘What do you do?’ And I say, ‘Schizophrenia.’ You know that’s going to be a conversation-stopper and you will also know that it’s going to be associated with violence, with antisocial behaviour, which is not at all the case. That’s rare.
To be ‘other’, in many instances, is to be on the wrong side of the boundary. The fact that Parshad-Griffin is mixed race gives her an officially designated category of ‘other’ in the UK. In addition, of course, her experience of mental distress reinforces her ‘otherness’. To be regarded as ‘other’ is to be treated differently, which often means prejudice and discrimination. ‘Otherness’ comes into play at all levels, but especially, it seems, when mental distress triggers ‘psychophobia’ in the people around. Although Parshad-Griffin’s situation also features ‘double discrimination’ (Baxter et al., 1990; Wainwright, McKeown and Kinney, 2019) because of her dual heritage, in many ways it is typical of the experiences of people who have periods of mental distress. Psychophobia leads to prejudice and discrimination. This may be something you have experienced yourself or have witnessed first-hand.
Being seen as someone with mental health problems may result in discrimination, often of a severe kind, as many people have found to their cost. The experience of being on the ‘other’ side of the mental health/distress boundary may be accompanied by unemployment, breakdown of relationships, low income and poor housing. For Black, Asian and Minority Ethnic (BAME) groups, the ‘other’ that is associated with racism is distressing and can directly contribute towards their experiences of mental ill-health. This is illustrated in the work below from the Black British artist Ashley Straker. In this piece, they graphically depict the emotional exhaustion experienced as a result of the COVID-19 pandemic, while also simultaneously dealing with racism and news about the injustice of Black people being killed. As indicated in the artwork, these stressors are a lot to ‘carry on your shoulders’.

Activity 2: David Harewood: Psychosis and Me
In a BBC/Open University co-production, British actor David Harewood (MBE), reflects on his past experiences as a young Black man sectioned under the Mental Health Act (i.e. detained for treatment without his agreement). In the following clip he discusses his experiences with clinical psychologist, Dr Chanelle Myrie.
Watch the clip now. Then write your answers to the two questions in the text box below.

Transcript: Video 1 David Harewood: Psychosis and Me
DAVID HAREWOOD
I'm starting to wonder how much of my psychosis was connected to the racism I was dealing with. And if my experience is shared with other young Black men.
TEXT ON SCREEN
Black men in Britain are ten times more likely than white men to be diagnosed with a psychotic illness and four times more likely to be sectioned. Sources: Government Race Disparity Audit/NHS Mental Health Act statistics.
CHANELLE MYRIE
There are lots of reasons why young Black men are being sectioned more. One reason is that Black men come to the mental health system later than their white counterparts, and that's for fear of being hospitalized, fear of being stigmatized. They arrive at hospital at crisis point, really.
DAVID HAREWOOD
Let me just-- I'm going to go to for my bag here-- I want to look, show you my records from 30 years ago.
CHANELLE MYRIE
Oh, wow.
DAVID HAREWOOD
See, look at this, I mean, this is like-- this is what a doctor wrote-- lively, bit of a clown, but sly underneath.
CHANELLE MYRIE
That's awful.
DAVID HAREWOOD:
It's awful.
CHANELLE MYRIE
Absolutely awful.
DAVID HAREWOOD
Very hostile and angry, shouting, fighting, given diazepam with the help of six policemen. Do you think that authorities consider us more dangerous?
CHANELLE MYRIE
I do, and I definitely think that there's a story that exists for how Black men are seen in society and that influences people's perceptions. Images of Black men as violent, hypermasculinity, so I think when a Black man presents in crisis sometimes people's ideas about what Black men are like overshadow the person that's actually in front of them.
DAVID HAREWOOD
So you think all those negative connotations, all those negative, all that negative language, plays into that--
CHANELLE MYRIE: It can play into your perception of yourself. Exactly, exactly. And the ideas of who you want to be, and who you can be.
DAVID HAREWOOD
I guess that's the part marginalization plays of images of self. If everybody you see on TV is white and all the police are white, all the heroes are white, it can subtly seep into your--
CHANELLE MYRIE
Yes, that's exactly it. So I think sometimes it's referred to as the everyday struggle, which is just what life is like for a young Black man. Experiences of marginalization, oppression, discrimination. And I think that actually things like that, experience like that, can have a cumulative effect in the development of psychosis.
DAVID HAREWOOD
It's good to hear that what happened to me wasn't just as a result of my individual issues, problems, but that there are factors at play in people that look like me.
- Why is it thought that young Black men are sectioned more often?
- What are some of the factors, described as ‘accumulative effects’ in the clip, that contribute towards the development of psychosis for young Black men?
Discussion
- Myrie explains that Black men access mental health services later than their White counterparts. This is due to the fear of being hospitalised and the fear of being stigmatised. As a result, they arrive at hospital or services, already at crisis point (i.e. when they are extremely distressed).
- The cumulative effects include the everyday struggles frequently experienced by young Black men. For example, their experiences of marginalisation, oppression, and discrimination (including ‘double discrimination’).
1.1.3 Boundaries of ‘normality’
The origin of the ‘other’ in society is the widespread human tendency to create categories where people who don’t fit in can be placed away from the mainstream. Social categories may lead to prejudice and discrimination, but may also lead to the physical separation of people to the margins of that society. Sibley (1995), in their seminal work, traces the physical marginalisation of people in what he calls the ‘geographies of exclusion’. Part of the process of exclusion is where the ‘bad’, the ‘mad’ and the ‘imperfect’ are deemed to be ‘other’ and, often in stereotyped form, are disregarded or rejected.
Being the ‘other’ in mental health terms means being on the ‘them’ side of the normality/abnormality boundary. What does it mean to be regarded as abnormal? Indeed, what is the nature of mental distress? What does it mean to have mental health problems? It all depends on where the boundaries are drawn, and by whom. A boundary may often be drawn, for example, in a way that differentiates mental distress from ideas of what constitutes mental health and wellbeing. A person experiencing mental distress is, therefore, at least temporarily on the other side of the divide from those who are ‘normal’ or ‘sane’. Boundaries divide and define, but do they help to explain differences?
It may be more helpful, in human terms, not to think about dividing boundaries, but instead of a continuum of mental health and distress. Instead of being on one side of a social divide or the other, we are at varying points on the continuum and can move along it, back and forth, stopping and (re)starting as life changes. This is a more inclusive way of thinking about mental distress, avoiding the fixed boundary between ‘them’ and ‘us’, and allowing everyone to move between points as circumstances change and episodes of distress come and go.
This is not a view shared by everyone. In the article by Perkins (Reading 1) that you read in Activity 1, she argues against the notion of a continuum on the grounds that it disguises and diminishes real differences between people. What needs to change, in her view, is the value we give to those differences. What do you think? The next activity gives you the opportunity to reflect on what ‘normality’ means.
Activity 3: What is mental ‘normality’?
Think about what normality means to you. In what ways do you consider yourself to be normal? Note down some thoughts and, if possible, discuss your views with someone else.
Discussion
It is not easy to define normality as it differs over time and between cultures. However, there is a sense of it meaning the ordinary or everyday aspects of life. This was certainly what a selected group thought when asked what normality meant to them. One said:
Normality for me is ‘everyday’. This might cover a range of emotions and feelings, from boredom and dissatisfaction to happy and engaged. Normality includes the usual, whether that be activities such as shopping, working or driving, or the uncommon but planned-for, such as going on holiday.
Another said:
Normality means day-to-day coping and rational thoughts; an ability to look at things objectively.
By way of contrast, creative artists and inspirational leaders live at least some of their lives in ways that are not ordinary and everyday. They may not be normal in that sense. But with talents that are way beyond those of the average person, they may come to be greatly revered. Other people, on the ‘wrong side of the divide’, may fare less well.
It is interesting to think about how normality and abnormality come to be defined in society. This point is taken up by Shaw and Woodward (2017), who suggest that people are less tolerant of unhappiness. This has led to more and more medicalisation of what at other times and in other countries might be regarded as normal human distress. Another take on the pathologising of day-to-day life experiences is the (rather tongue-in-cheek) concept of happiness as something that even years ago could be classified as a psychiatric disorder (Bentall, 1992). It is abnormal (or disorder-like) in the sense that it is not commonly experienced as ordinary and everyday for the majority of people. There are, of course, dangers in extending the boundaries of abnormality ever further, and the absurdity of classifying happiness as ‘a major affective disorder, pleasant type’, for instance, is plain to see. The nature of normality is contested, and so too is the nature of mental illness or distress. In the next section, you’ll look at competing explanations of mental distress.

1.2 Ways of viewing mental distress
The first point to note is that there are two key competing ways of viewing mental illness or distress: physical and social. One of the functions of this course is to draw together aspects of these accounts in order to cross the boundaries that they create and maintain. Our aim in this respect is to devise a third way, a more rounded and holistic approach that brings together the best of both worlds. In the meantime, though, the physical and social explanations predominate. Physical explanations are based on, for example, notions of brain dysfunction or genetic predisposition. Mental distress, in those terms, is a disorder of the mind, akin to a physical illness. Social explanations, on the other hand, are based on an understanding of difference and discrimination: on structural factors in society that separate people and may come to oppress them. Another way of understanding mental distress – and this links with our ‘third way’, the holistic (whole person) approach – is to view it from the standpoint of those who have experienced it. This is an important vantage point. The next activity invites you to read, and reflect on, the personal experiences of one woman who has experienced mental distress.
Activity 4: Personal experiences of mental distress
Read the short extract below by Veronica Dewan. Make notes on how she explains the origins of her mental distress.
Veronica Dewan
I became engaged in an official system of care at birth, a system that denigrated my Indian heritage, a system that made meaningless my true identity. It was my first encounter with social services in 1957 at six weeks of age – an illegitimate, ‘mixed race’, hard-to-place baby. […]
Several inpatient admissions to an acute psychiatric ward compounded childhood and adult experiences of racism, misunderstanding and intimidation. I persisted with suicidal plans and attempts, and was severely depressed, with psychotic episodes of manifestations of my adoptive mother’s attempts to kill me as a child. The underlying requirement of the psychiatric system appeared to involve fully internalising the racism, to make me completely ill forever. […]
As I challenge more and more my own perceptions, question their origins and try to understand my place in the world, I believe that the official care system tried to silence me into living a life that was not my own. While institutional racism continues, by its insidious nature, to cause so much unarticulated pain, I have to be vigilant in holding onto my right to exist, as a Black woman of dual heritage. The people who have no interest or motive in controlling me, but only a willingness to engage through mutual love, acceptance and respect, are those who remain in my life.
Discussion
Veronica’s explanation of her mental distress includes:
admission into care as an illegitimate, mixed race, ‘hard-to-place baby’
childhood experiences of racism (combined with the denigration of her heritage)
admissions to hospital
suicide bids
breakdown of the relationship with her adoptive mother.
The author acknowledges the importance of her personal experiences and histories. Abuse, rejection and separation played a part in creating her experiences of mental distress. She also highlights how her experiences of mental health systems had a negative impact on their lives, compounding her original difficulties. She has a voice now, as a survivor and writer, but the systems of the time sought to silence her. Her accounts also point to structural factors within society – racism, discrimination and oppression.
Is mental distress a cry for help? Is it a form of resistance? Or is it a response to ‘unarticulated pain’? The answers are not so straightforward. But British artist Kingsley Nebechi skilfully highlights the impacts of distress in the artwork below. Explaining that uncertain or stressful times can make it difficult for us to stay focused on our daily tasks. In fact, what was once a simple daily routine can feel like a strenuous mental ladder.

2 Whose risk is it anyway?
Western society is increasingly preoccupied with concerns about risk, and it is argued that people in general are experiencing heightened levels of anxiety in response to rapid technological and social change. News stories in the media are filled with warnings and fairly frequent dire predictions for the future. This is particularly true when the potential consequences appear to be both catastrophic and difficult to predict, such as nuclear accidents, pandemics, global warming and so on. Intense pressure is exerted on politicians and others, particularly through the media, to prevent disasters and take the blame when they occur.

Risk has certainly become a central concept in mental health policies and practice, particularly since the implementation of community care in the early 1990s. Community care policies have been highlighted both by the media and by government as a failure, partly because they have failed to provide service users/survivors with the support they need in the community. However, they are also regarded as a failure because of the perception that they have led to an increased risk of violence by people experiencing mental health problems. The focus has been on homicide in particular. It is important to emphasise that this is a perception rather than a fact, because research evidence strongly suggests that there has not been an increase in homicides by people experiencing mental health problems. In this section you will critically examine the way risk has become a central concept in mental health policy. You will explore why this may have happened and the impact it has on the experiences of service users/survivors and on professional practice.
The next section addresses the way risk is defined, and highlights the fact that risk is a problematic concept. The extract then moves on to explore the concept of risk in mental health policies. It also looks at the impact of the new ‘culture of risk’ on both service users/survivors and mental health professionals.
2.1 What is risk?
‘Risk’ is a word which is used frequently and in many different contexts. On the face of it, it can seem as though the word has a clear meaning, but when you start to examine the different ways it is used it seems less straightforward. This is because ‘risk’ is not a real thing in the world, it is a concept, which simply means it is an idea expressed in words. In fact, the more you explore it, the more you realise risk is a problematic concept: it has been defined in a number of ways and so means different things in different contexts and to different people. There has been a lot of debate about the meaning of risk in recent times because it is seen as increasingly central to modern life. This section explores the meaning of risk and looks at the different explanations offered for its increased prominence. Examining how people use the word in everyday life may help to unpack its meaning, and so this is the focus of the next activity.
Activity 5: Exploring the meaning of risk
Take a few minutes to think about how you would define the word risk and make a note of your ideas. If you get the opportunity, ask other people what they think the word means, and make a note of what they say too. Look out for two important ideas: that risk involves the chance, likelihood, or probability (or similar words) of something happening, and it often involves the chance of something ‘bad’ happening or something ‘good’ happening, or perhaps both.
Discussion
The following are some examples:
Risk only exists when there is something to lose.
Risk involves an assessment of the likelihood of any particular outcome occurring.
Risk can lead to failure.
Risk is sometimes defined by you, sometimes by others about you.
Risk is the probability of a predicted outcome occurring.
Although your definitions of risk may be different, they are likely to involve the two ingredients of the chance of something happening and the nature of the outcome, which might be good, bad or both.
The likelihood of something happening can be assessed in two ways: in mathematical or in more qualitative terms. The mathematical approach involves measuring the probability of an event occurring and giving a figure that summarises the risk. For example, before consenting to an operation a patient might be given a figure that describes the likelihood of the procedure being unsuccessful, such as ‘a 1 in 100’ chance of ‘failure’ (with the worst-case scenario being death). This would mean for every 100 patients who had undergone the same operation, it had been a success for 99 of them. Of course, this means it had been a failure for one person. This would clearly be much better than being told there is ‘a 1 in 2’ chance of success, which would mean the operation (likely to be an experimental one with those odds) had been a success for one out of every two patients. Qualitative approaches use words instead of figures, by saying the likelihood of an outcome is, for instance, ‘quite likely’, ‘very likely’ or ‘very unlikely’. In both mathematical and qualitative approaches, some assessment of the likelihood is being made.
In the context of mental health, a similar distinction is drawn between two kinds of risk assessment: ‘actuarial’ and ‘clinical’ (Galynker and Galynker, 2017). Actuarial risk assessments use statistical information about populations to help make decisions about who may be ‘at risk’, depending on whether or not they belong to a high-risk group. For example, in suicide risk assessment it is known that higher-risk groups are middle-aged men, those who misuse substances and those experiencing major stressors, for example a sudden financial crisis (McManus et al., 2019). Clinical risk assessment is when professionals use their informed judgement to assess the level of risk. This judgement may be based on experience as much as statistical knowledge about risk factors. Most risk assessment involves some combination of these two approaches.
Closely linked to the likelihood of an outcome occurring is the second important aspect of defining risk, which is the nature of the outcome. To continue the example of a medical procedure, a patient might be making a decision about a relatively minor operation which involves only local anaesthesia. The possible outcomes associated with such minor surgery are normally far less serious than those involved in an operation under general anaesthetic, because the general anaesthetic itself carries some degree of risk. So, decisions about risk often involve consideration not only of how likely an event is to happen, but also what the consequences might be if things go wrong: whether it is ‘high consequence’ or ‘low consequence’.
Some definitions of risk incorporate the possibility of good outcomes as well as bad. For example, if you buy a lottery ticket, you might say that you are taking a ‘risk’ because there is a chance of a bad outcome (you might lose the small amount of money outlaid for the ticket purchased) or a good outcome (you might win some or a lot of the money back).
However, a number of commentators have argued that risk is not really thought of in terms of balancing good and bad outcomes any more. They argue that in Western societies risk now generally refers only to the possibility of a bad outcome and there are important reasons why it has taken on this meaning. Mary Douglas (2013) is one of the most influential thinkers in this area and she argues that risk in modern Western societies now equals danger.
Danger is clearly a word associated with negative outcomes. For Douglas, one of the reasons the word risk is more prominent is that it implies a rational, scientific capacity to measure danger accurately. It is therefore well-suited to modern industrialised societies where there is rapid technological change. This is because, as you have already seen, risk is associated with words like ‘probability’, where an estimate can be given for the chances of something occurring in mathematical terms. The appeal of risk is that it gives us the sense of dangers being measurable scientifically and therefore manageable.
Douglas has also argued that risk has become a central concept in modern life because it has a ‘forensic’ function. Blame is primarily centred on the failure of someone to assess risk accurately and then to take the steps necessary to prevent a tragic incident. So the concept of risk enables people to look back at tragic events and attribute blame for them to someone else. The media can play a key role in shaping how we all think about risk and the process of attributing blame. The next activity focuses on risk-related stories in the newspapers to explore how risk issues are presented in the media. This may help clarify further some of the complex issues to do with risk you have considered so far.
Activity 6: Exploring risk in the media
Look at two newspapers that are clearly aimed at different sectors of the population (such as the Independent and the Sun, or The Guardian and the Daily Mail) from the past few days. Scan the headlines for stories that are concerned with risk in some way. Some may actually have the word ‘risk’ in the headline, but most will not. You may find risk-related words such as danger, hazard or warning instead. Read through the articles you find and start to analyse the way risk is being presented. Look out for the dimensions of risk you have already considered in this section as follows:
the likelihood of something happening (which might be expressed mathematically, i.e. using statistics, or qualitatively)
a focus on bad outcomes as opposed to good ones
the seriousness of the outcome
whether anyone is being blamed.
Make a note of what you find under a separate heading for each newspaper.
Discussion
In analysing the articles you may well have noticed references to likelihood in some form. These may have been in the shape of quantitative risk estimates, including references to probability such as ‘twice as likely’ or ‘three times more likely’. You may also have noted more qualitative statements, such as ‘very likely’ or ‘higher risk’. In terms of the nature of the outcomes, the focus in press reports tends to be on bad outcomes rather than good. You may have noticed that some newspapers tend to go into greater depth in their reports, and often make an attempt to analyse findings in a more sophisticated way. They tend to use more complex language and discuss the implications of reports more thoroughly, although this is not always the case.
You may have commented that headlines about risk in ‘tabloid’ newspapers tended to be more sensationalist. For example, one headline simply said, ‘We Will Die’! In contrast, other newspapers seemed to try to give more factual accounts of potential outcomes.

This activity suggests another important dimension of risk, which is that risk is political. The way risks are presented in different parts of the media and elsewhere vary according to the perspective of the groups or individuals concerned. These different perspectives often come into conflict with one another. Some groups may seek to ‘play down’ a risk, while others may seek to magnify it. Some kinds of risks are given greater weight than others because of what they mean, culturally or politically, and so the amount of attention different risks receive is not always proportionate to the actual likelihood of an event occurring.
A good example of disproportionate attention given to low probability events in the media is the focus on homicide by someone experiencing mental health problems. It is argued that this has been one of the most significant contributions to the ‘fear factor’ about ‘mental ill-health’ since community care policies were introduced. In mental health terms, the negative reporting of mental illness in the news media and social media posts increases stigmatising attitudes (Ross et al., 2019). The next section further explores the central position of risk as a concept in connection with mental health and distress.
2.2 Community care, fear and the ‘high-risk’ service user

So far in this course you have seen how the concept of risk has come to suggest danger. This section explores in greater depth how the changes that have led to this situation have impacted on mental health policies and practice.
A major change in mental health policy, which occurred over a number of years, was the shift from asylum-based treatment to care in the community. There has been a great deal of debate about whether this policy has been a success or not. However, one thing is clear: the media portrayal of people experiencing mental health problems in general continues to be negative.
The debate about the supposed link between mental distress and the risk of violence to other people is also fraught with difficulty, and you have already examined some of the issues. Consider for a moment the question of how ‘violence’ itself should be defined. In some studies, violence has included relatively minor acts which have been excluded from other studies. In other words, different studies have been measuring different things. However, studies do consistently show that the vast majority of people who act violently in our society are not experiencing mental distress. The main risk factors for violence are being male, young, less well-off and under the influence of alcohol. Equally, the vast majority of people who do experience mental distress, or have a history of it, never behave violently. To this extent, the link between mental distress and violence is very weak. Furthermore, Ross and colleagues’ (2019) work has noted that the media can potentially exacerbate or exploit this weak link. For example, after systematically reviewing all research studies that explored the impact of the media on stigmatising attitudes towards those with ‘severe mental illness’ they documented some notable trends. In particular that reporting in the news media often focussed on the negative aspects of mental illness, and that there was an over-representation of negative portrayals of people with a mental illness, where dangerousness to others and violence were the most common negative depictions.
The media continues to present a picture which increasingly links mental distress with violent behaviour. The focus on the rare event of homicides in the community by people experiencing mental distress has resulted in the perception that the number of such events has increased. However, since 2009, the number of homicides committed by people diagnosed with a mental illness has actually decreased (Appleby et al., 2018). Moreover, when a detailed analysis of ‘patient homicides’ in the UK (from 1997 onwards) was conducted, certain key features were identified. Specifically, substance misuse was usually a factor, around half of the ‘patients’ were not receiving the mental health care intended for them and the ‘patients’ were also at high risk of being a victim of homicide (Appleby et al., 2018). Tellingly, the issues are not new, as in 2001 the National Confidential Inquiry into Homicide and Suicide by People with Mental Illness (DH, 2001) stated:
One of the most distressing problems facing people with mental illness is the prejudice and discrimination they face from society at large. In particular, the assumption that they are likely to be violent is painful and destructive. The Department of Health, the Royal College of Psychiatrists and others have attempted to tackle these public perceptions and pejorative press reporting through campaigns that aim to give the facts about the risks presented by the mentally ill. Key findings in this report should be used in this way. For example, the killing of strangers by people with mental illness is rare; most stranger homicides are committed by young men without mental illness who are under the influence of alcohol or drugs. The public may fear the mentally ill but they are more at risk from heavy drinkers.
The idea that mental distress can be very frightening, for both those who experience it and those close to them, is hardly new. Many people who have written about how mental health services have developed have emphasised the importance of social fears and anxieties as determining factors in the way mental health care is organised. The asylums of earlier centuries, for example, are often portrayed as institutions designed to ‘protect’ society as much as, if not more than, the people who were detained in them.
It was argued that community care policies in the 1990s (and beyond) have resulted in many of these fears being revisited with a special force because they may reflect deep-rooted cultural fears of mental distress (Pearson, 1999). Presenting the media with ‘the facts’ is likely to have little impact on such deep-rooted fears and this may explain why this strategy has so far failed to prevent negative media reporting. These fears are about what it means to be ‘mentally distressed’ in a society which is undergoing rapid change, one consequence of which, it is argued, is that ‘rationality’ and social order are valued particularly highly.
You have seen that there has been a focus in policy and the media on what individuals may experience or do to other people. However, there is good evidence in the relevant literature of important risks posed by organisations and services to service users/survivors. In other words, sometimes services are organised in a way that means service users/survivors are exposed to risks they otherwise might not encounter. A good example is the way hospital discharge planning tends to emphasise the importance of someone’s preparedness for discharge from an in-patient mental health unit. Decisions about this are often based on relatively narrow measures of someone’s fitness, relating to the treatment for whatever is identified as their primary mental health issue. Organisations tend to focus on preventing bad outcomes for which they are likely to be penalised financially. In particular, the culture of risk assessment has its origins in the increasingly litigious culture of the NHS in general. Organisations are afraid of being sued, and individual professionals are afraid of being vilified.
Different groups of service users/survivors are affected in different ways by the culture of risk and defensive practices in mental health services. One particular group that is adversely affected, and about whom a culture of fear has developed, is young men diagnosed as having schizophrenia. Within this group, Black men are particularly ‘at risk’ of being regarded with fear and mistrust. Research has shown that people from particular ethnic groups are over-represented in some psychiatric diagnostic categories compared with other ethnic groups. One of the most hotly debated issues relates to the over-representation of African-Caribbean men with a diagnosis of schizophrenia.
There is also an over-representation of African-Caribbean men in terms of the kinds of services they are likely to receive. They are more likely to experience coercive forms of intervention, such as compulsory admission to hospital or detention via the police. In terms of explaining this over-representation, one very powerful argument presented in some studies is that Black people are less likely to voluntarily seek support from services than their White counterparts. This is because of the poor experiences many Black people have had of mainstream services. Therefore they are less likely to benefit from support, from their GP for example, during the early stages of their experience of mental distress. When they do eventually come into contact with services, they are thus more likely to do so because they have become extremely distressed.
The relationship between ethnicity and violence is another good example of how the media have contributed to distorted images of particular issues. In a general sense, media reporting of crime contributes to an association between Black people – especially young Black men – and certain types of crime (particularly muggings and other forms of violence). This means that young Black men are at risk of becoming the victims of a particularly powerful cocktail of distorted images. This is an issue which has been actively addressed by some services in order to adequately meet the needs of particular groups of service users/survivors.
Fanon Care is an organisation based in south-west London which provides specialist mental health services for African and Caribbean people living in the area (Southside Partnership, n.d.). In particular, it stresses the importance of early intervention in order to avoid crises. It is a good example of an approach to services which emphasises people's needs rather than risks. The organisation's vision statement says:
Fanon Care’s vision is of:
A society that puts people first and provides them with a choice of the highest quality services aimed at promoting mental well-being, delivered by people who want to make a difference.
A society where Black people in mental distress are valued and included as equal citizens in the communities in which they live.
A society where there is much greater public understanding of the issues they face, and where diversity is valued.
A society that recognises the oppressive nature of racism and its effects on mental well-being.
The narrow focus on the risk of violence has serious implications for service users/survivors and their everyday experiences of services and professionals. As well as perpetuating a negative image of mental health service users/survivors, it also means that other risks that are just as real and pressing tend to be neglected. In part, this problem can be addressed by professionals in their practice by paying closer attention to service users’/survivors’ perspectives on risk.
3 The business of madness

In this section you’ll consider mental health as a business. This is not the way mental health services are usually regarded, as it is more common, at least in the UK, to regard them as public services. However, ideas about being more business-like in health and social care have gained prominence in recent years. What does being a business, or more business-like, mean? For one thing, it implies a profit motive: goods or services delivered to make money for private companies and their shareholders. This is quite controversial when applied to mental health services. There is a tension between mental health services as a business – a growth industry – and as a regulated public service. Caught between the two are the service users/survivors and their families. How are their needs met by the competing forces in the mental health marketplace?
Being a business also suggests the importance of delivering what customers want so that the provider stays in business and flourishes. Further, it means being efficient, systematic and practical. That, at least on the face of it, looks like a very positive attribute for mental health services.
This section takes these three issues – the profit motive, delivering what the customer wants, and efficient, systematic and practical services – as its organising framework. In Section 3.1 you begin to consider the concept of mental health as a business, and in Section 3.2 you focus on the profit motive and the controversial role of pharmaceutical companies. Section 3.3 considers ‘what the customer wants’, and Section 3.4 tackles the question of pharmaceuticals for mental health, and some specific historical examples – the National Institute for Health and Care Excellence (NICE) guidelines and the National Service Framework for Mental Health.
3.1 Mental health as business: introducing the debate
Is mental health a business? There are a number of signs that it could be, and Activity 7 presents a discussion between two people with strong views on mental health services and how they should be delivered. Dr Harvey Gordon is a forensic psychiatrist who has been a long-term consultant at Broadmoor High Security Hospital, and also a consultant at the Maudesley Hospital in London. Jim Read has worked for many years in organisations and networks of mental health service users/survivors as a consultant, trainer and writer.
Activity 7: Mental health as business
Listen to the two sequences of audio below. You might find it helpful to listen right through both, with the questions in front of you, and then make detailed notes after a second hearing.
What does ‘business’ mean to Jim and Harvey?
What are their main points of difference?
Are there any areas where they agree?
Transcript: Audio clip 1
Transcript: Audio clip 2
Discussion
What does ‘business’ mean? Examples from the clips include: ‘affected by financial factors’; ‘budget constraints’ (Gordon) contrasted with a public service (Gordon) constant reorganisation in the NHS (to make it more business-like?) (Read) choice for service users (both) the use of direct payments to put the user in charge (Read) pharmaceutical companies are motivated by financial gain, but they need to produce something that doctors will prescribe and people will benefit from (Gordon) new markets for drugs are created by identifying new conditions needing treatment (Gordon) standardising services is difficult because of geographical constraints on where people can get treatment (Gordon) and because the quality of services depends on the people delivering them (Read) community-based services, which may well be less expensive, produce better outcomes than services which rely heavily on drugs (Read).
Points of difference: the major area is over the use of drugs. Read is basically against the use of drugs to treat mental distress, while Gordon offers a spirited defence of them, for the benefit not only of service users/survivors but also of their families.
Points of agreement: both speakers agree that it is not easy to offer choice in this context. And neither of them wholeheartedly embraces the idea of mental health services run on business principles.
In the next section you’ll focus on one strand of this debate, touched on by Read and Gordon – the role of drug companies, and the lure of the profit motive.
3.2 Mental health as business: the profit motive
There is little question that the use of drugs to treat mental distress has become the dominant strategy. The historian Edward Shorter puts it graphically:
If there is one central intellectual reality at the end of the twentieth century, it is that the biological approach to psychiatry – treating mental illness as a genetically influenced disorder of brain chemistry – has been a smashing success.
Perhaps the most controversial aspect of mental health services and their relationship to business is the role of major companies which manufacture and market drugs.
3.2.1 A conflict of interest
One of the difficulties of the involvement of drug companies in the mental health field is that it produces a conflict of interest. To put it crudely, drug companies rely on a continuing supply of patients to keep them in business. This is not always congruent with people’s best interests, as you will see below. Although mental health services are intended to help people experiencing mental distress, they also have other driving forces. The market economy model of provision has encouraged the expansion of various aspects of mental health care, but has fuelled, in particular, the development and promotion of drugs to such an extent that it is now a huge business. The impact of the pharmaceutical industry is perhaps most pronounced in the USA, where the view that ‘psychiatry has been almost bought out by the drug companies’ (Mosher, 1999, p. 16) has been held for a number of years.
Concern about this conflict of interest is not new. In 1965, a journalist from the Washington Post wrote about the ‘therapeutic nightmare’ of psychiatric drugs being used to control ‘millions’ (Mintz, 1965). In 1974, the American Journal of Psychiatry raised concerns that ties between the American Psychiatric Association (APA) and pharmaceutical companies were going beyond the bounds of professionalism, compromising the organisation’s principles, and in some instances involving members in conflicts of interest (Breggin, 1993). By the 1980s a visible lobby within psychiatry was opposing the influence of the pharmaceutical companies. The main concerns were that:
Drug companies influenced individual psychiatrists’ prescribing decisions through heavy promotion at the conferences and in the academic journals they sponsored.
The dependence of university research departments on drug company funding might lead to bias in their results, particularly the results of studies evaluating the efficacy and safety of particular drugs.
More recently it can be argued that there is a growing medicalisation of aspects of everyday life, with conditions such as Attention Deficit Hyperactivity Disorder (ADHD) being treated with drugs. The use of Ritalin to treat children diagnosed with ADHD is widespread, with millions of children being prescribed this.
Whatever the cause, the trend of prescribing drugs opened the divide between the psychiatric professions and charities such as Mind that campaigned on behalf of people experiencing mental distress. The run-up to the Mental Health Act 1983 saw Mind and others arguing for stricter controls on the use of drugs for patients detained against their will. A decade later the pharmaceutical industry was rethinking its strategy for marketing to the NHS, following the creation of the internal market:
Glaxo Laboratories has an NHS Relations Unit which was set up in response to the major changes in the NHS structure […] Links are being established at managerial level in regional health authorities, district health authorities and family health services authorities.
Persuading professionals to prescribe a particular drug is vitally important to drug companies in terms of their ongoing profitability. For example, a single prescription of fluoxetine (Prozac) is £61.62 (NICE, 2019). Just how big is the market for antidepressants? Table 1 gives an indication of the market for antidepressants in England.
| Total items 2019 | Total items 2018 | Total items 2014 |
| 74,814,619 | 70,873,979 | 57,149,109 |
| Total cost 2019 | Total cost 2018 | Total cost 2014 |
| £201,729,576.00 | £202,526,719.66 | £265,008,698.97 |
As Table 1 illustrates, the ‘growth in the market’ for antidepressants has been considerable (i.e., there has been a 30.9% increase in ‘total items’ from 2014 to 2019). Such that antidepressants are now ranked as the ninth biggest expense in terms of medication purchases in England. By comparison, drugs used in diabetes care are ranked first, costing more than five times as much, at over £1 billion per year (NHS, 2020). But you will see that the total cost has decreased for antidepressants, which is not unusual given the ‘bargaining power’ of a large ‘customer’ like the NHS. The concerns associated with the growth in prescriptions of antidepressants is not new, as the following extract illustrates.
While health regulators are becoming increasingly anxious to control the use of Seroxat and other antidepressants, drug companies – equally anxious to gain as much income as possible from their medicinal cash cows – are trying to expand their uptake.
GlaxoSmithKline has made billions out of Seroxat and sees no reason why this should halt, it would appear. One of its internal marketing documents shows the company planned to double sales by targeting people who suffer from a widely recognised condition known as social phobias.

So, it can be extremely lucrative for a company to produce and successfully market a drug which is widely prescribed. Just how did this situation come about? In the next section you look at the history of the use of drugs for people experiencing mental distress by tracking the introduction of successive waves of medication, from early antipsychotics to more recently the use of selective seratonin re-uptake inhibitors (SSRIs).
3.3 Pharmaceuticals for mental health: a brief history

The ‘revolution’ in drug therapy is widely credited as a major cause of the mass closure of psychiatric hospitals which began in the 1950s and 1960s, meaning that patients who had previously been considered too much of a danger to themselves or others could be safely housed ‘in the community’. However, the trend for a reduction in numbers treated in long-stay asylums was already evident at the time the drugs in question began to be available, and academics such as Joan Busfield and Andrew Scull have previously argued that the correlation between the two is much less clear than had been suggested in the past (Busfield, 1986; Scull, 1984).
Whether or not it enabled closure of the large institutions, there is no question that medication has revolutionised the way people experiencing mental health problems are treated. Drug treatments had obvious advantages over their crude precursors, which included physical restraint and lobotomy. Although the effects of the early antipsychotics can be compared to the effects of lobotomy (Breggin, 1993), it was thought that they would have a short-term impact which would cease when the drug was no longer being administered. Combined with the impact of a series of scandals about conditions in long stay hospitals (see Scull, 1984), drugs which enabled people to leave institutions appeared highly attractive.
Activity 8: Pros and cons
Consider the advantages of antipsychotic medication in terms of the interests of service users/survivors, professionals and the state, and make brief notes.
Discussion
Antipsychotic drugs had advantages for all concerned:
For service users/survivors, they reduced the likelihood of institutionalisation and opened the possibility of a better life.
For professionals, they moved public perception away from ‘gaoler’ towards ‘doctor’, reinforcing psychiatrists’ power to understand and treat ‘madness’ because they could prescribe drug treatment.
For the state, they offered the possibility of cheap management of ‘deviant’ individuals, and a less obviously restrictive set of practices than large institutions, which might (and did) draw criticism from civil liberties campaigners.
However, there were disadvantages. From a service user’s/survivor’s perspective, the less damaging effects of the drugs had to be weighed against a long list of debilitating side effects. Since the first appearance of antipsychotic drugs in the 1950s, their side effects have become better understood. Originally termed ‘neuroleptic’ (because they attached themselves to neurons in the brain), the early antipsychotics were considered to have mainly sedative effects. (Another name for drugs in this class is ‘major tranquillisers’; examples are chlorpromazine, thioridazine and haloperidol.)
Following the thalidomide crisis in the UK in the late 1950s and early 1960s, when over 6,000 children were born with severe disabilities because of a drug administered to their mothers during pregnancy, a system of routine reporting of any adverse effects of prescribed drugs was introduced, voluntary for health professionals but obligatory for pharmaceutical companies (MHRA, 2003).
This involved doctors completing a yellow slip describing the prescription and reported side effects and submitting it to the Committee on Safety of Medicines. Since the introduction of antipsychotic drugs, critics of the medication had suspected that their adverse effects were being under-reported. It was suggested that virtually everyone for whom these drugs were prescribed experienced some unpleasant effects. In response, Mind launched its own Yellow Card scheme in 1995, encouraging service users themselves to report unwanted side effects directly to the charity. Although run as a campaign and not a scientific study, the results went a long way towards supporting the claims of under-reporting (see Cobb, 2001).
In the 1990s the drug companies themselves produced scientific evidence of the unpleasant effects of antipsychotic drugs, but only when a set of new, more expensive alternatives, the ‘atypical’ antipsychotics such as clozapine and risperidone, was available.
3.4 Benzodiazepine tranquillisers, Prozac and the SSRIs
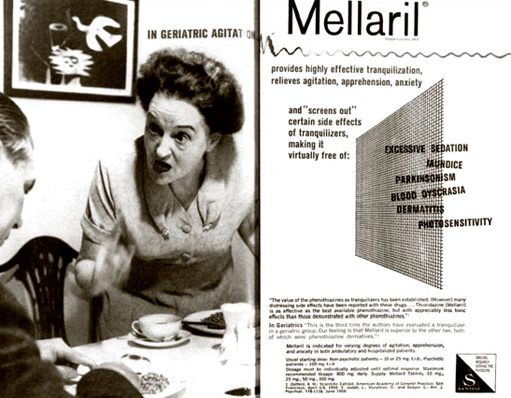
One of the most significant ranges of drugs ever produced is the benzodiazepine tranquillisers (usually classed as ‘minor tranquillisers’ or ‘hypnotics’), often prescribed as a remedy for ‘minor’ disorders such as depression, sleeplessness and anxiety. In effect, they extended the range of conditions that could be treated by medication. The best-known example is probably Valium.
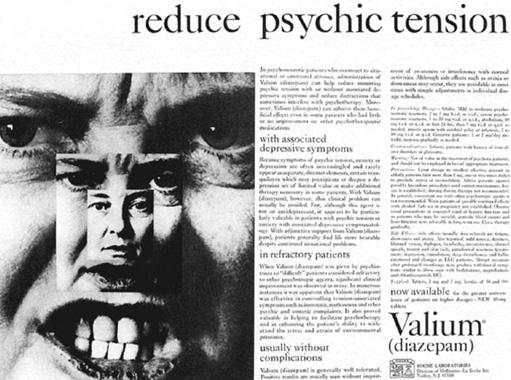
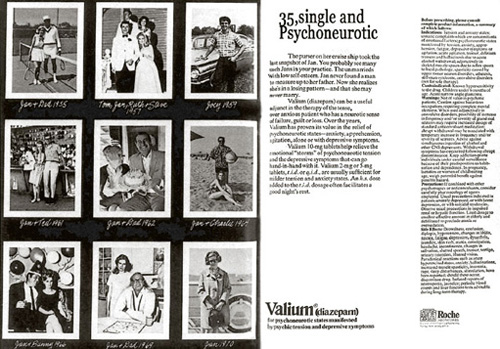
Like their predecessors, these drugs began to attract criticism from a number of different quarters. Some pointed to the dangers of addiction (Agrawal, 1978), while others said that the drugs were being used to help women endure gender oppression rather than escape it (Johnstone, 1989; Waldron, 1977). The selected adverts reproduced here certainly suggest a focus on ‘women’s problems’.
Addiction to benzodiazepines continues to be a major topic of controversy. In 2001 a study conducted for the BBC TV programme Panorama (The Tranquilliser Trap, broadcast 13 May 2001) showed that 28 per cent of people being prescribed benzodiazepines had been taking them not for the recommended four weeks, but for more than ten years. Although more recent debates have centred around the importance of legitimate use of benzodiazepines, where they should be appropriately used alongside psychotherapy (i.e. talked-based interventions) (Silberman et al., 2020).
In 1987 came Prozac (fluoxetine), one of the range of drugs known as the selective seratonin re-uptake inhibitors (SSRIs). According to trials commissioned by the drug companies, these new drugs were non-addictive and had fewer side effects. They were marketed alongside benzodiazepines for a wide range of conditions from ‘generalised anxiety disorder’ to severe depression and schizophrenia. These drugs aim to actually ‘cure’ the ‘illness’, arguably taking mental distress further out of its social and holistic context. In the USA, SSRIs have been marketed directly to the public in an effort to get people to persuade their doctors to prescribe them. SmithKline Beecham spent $30m marketing the SSRI Seroxat (Paxil) directly to customers in the USA in 1999 alone (Rogers and Pilgrim, 2003). Marketing campaigns began to hint that as well as curing depression and anxiety, SSRIs could enhance functioning in healthy people.
Such direct marketing is banned in many countries including the UK, but the media were nevertheless susceptible to stories planted about the new ‘wonder drugs’. The government responded to the problem of keeping health-related costs under control by creating in 1999 the National Institute for Health and Care Excellence (NICE) (previously called the National Institute for Clinical Excellence), a semi-autonomous body charged with deciding which interventions are evidence-based and should be used in practice.
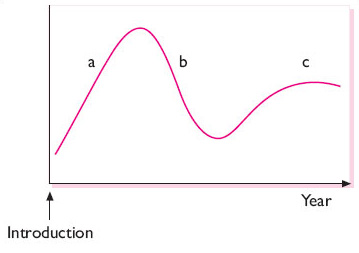
Beginning in the 1990s evidence emerged that SSRIs might not be as safe as originally thought (Breggin, 1993). The cycle of acceptance for new drugs (and health interventions more generally) such as the SSRIs, as with their predecessors, has followed the pattern shown below in Figure 6. The graph shows a peak reflecting initial enthusiasm that there will be a cure, followed by devaluation as side effects and issues become more evident, followed by stability as ‘rational use’ is established.
In summary, then, although medication has had a beneficial effect on many millions of people experiencing mental distress, there remain serious concerns in particular the influence of pharmaceutical companies on medical personnel, the research agenda, university departments and potentially even governments.
Conclusion
This free course, Challenging ideas in mental health, provided an introduction to the field of mental health, and critically explored some of the key issues in the field. It took you through a series of exercises designed to develop your approach to study and learning at a distance and helped to improve your confidence as an independent learner.
This OpenLearn course provides a sample of Level 2 study in Health and Social Care. You might be particularly interested in the Open University course K240 Mental health and community.
Sources of help
If you are looking for assistance for yourself or someone else, you can access these services in the UK.
For more urgent help:
- If your life is at risk, you need an emergency service, and can go to A&E (or dial 999).
- Your local GP surgery should be able to offer you an appointment quickly if you need urgent support.
- For telephone support you can call the Samaritans free of charge on 116 123.
For a guide on mental health supports more generally check out the resources summarised by the UK mental health charity, Mind.
References
Acknowledgements
This free course is based on materials from the Open University course K272 Challenging ideas in mental health which is no longer available. It was updated in May 2021.
The content acknowledged below is Proprietary (see terms and conditions) and is used under licence.
Grateful acknowledgement is made to the following sources for permission to reproduce material in this course:
Text
Reading 1: Perkins, R. (1999) ‘Madness, distress and the language of inclusion, Openmind, Vol 98, Jul/Aug 1999, © 1999 Mind (National Association for Mental Health).
Reading 2: Rose, D (2001) ‘Terms of engagement’, Openmind, Vol.108, Mar/Apr 2001. pp. 16–17 © 2001 Mind (National Association for Mental Health).
Images
Please Note: the use of the following advertisements in Figures 10, 13, 14 and 15 are for the purposes of educational/academic analysis and fulfilling the learning outcomes of the course. No endorsement or approval by The Open University or OpenLearn of these or any other advertisements which may be used in an educational teaching and learning context should be construed. See Terms and Conditions.
Course image: Rebecca L. Daily in Flickr made available under Creative Commons Attribution 2.0 Licence.
Figure 1: Vitezslav Vylicil/Getty Images
Figure 2: Courtesy of Ashley Straker.
Figure 3: Helena Lopes for Pexels.com
Figure 4: artist Kingsley Nebechi, courtesy BBC https://www.bbc.co.uk/bitesize/articles/zkhpf4j
Figure 5: AndreyPopov/Getty Images
Figure 6: Suzy Hazelwood for Pexels.com
Figure 7: kat wilcox for Pexels.com
Figure 8: Suzy Hazelwood for Pexels.com
Figure 9: Miguel A. Padrinan for Pexels.com
Figure 10 ‘Let me eat my peas’: Mellaril advertisement from American Journal of Psychiatry, Vol. 117 (1960-61), pp. xii–xiii;
Figure 11: freestocks.org for Pexels.com
Figure 12: https://polypath.wordpress.com/2012/08/27/warley-hospital/
Figure 13: Valium advertisement from American Journal of Psychiatry, Vol. 121 (1965), pp. xxii–xiii;
Figure 14: Valium advertisement from Archives of General Psychiatry, Vol. 22 (1970), p. 481;
Figure 15: Prozac advertisement from Self, March 1998, p. 19.
Audio-Visual
Video 1: © BBC
The extracts are taken from the course K272 Challenging ideas in mental health Copyright © 2004 The Open University.
Don't miss out:
If reading this text has inspired you to learn more, you may be interested in joining the millions of people who discover our free learning resources and qualifications by visiting The Open University - www.open.edu/ openlearn/ free-courses