Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Thursday, 23 April 2026, 11:23 PM
Communicable Diseases Module: 32. General Features of Faeco-Orally Transmitted Diseases
Study Session 32 General Features of Faeco-Orally Transmitted Diseases
Introduction
In Parts 1 to 3 of this Module, you have learned the general principles of how communicable diseases are transmitted, the specific features of the bacterial and viral vaccine-preventable diseases, and about malaria, leprosy, tuberculosis (TB) and HIV/AIDS. In Part 4, you will learn about other diseases of major public health importance in Ethiopia, beginning with faeco-orally transmitted diseases, i.e. diseases in which the infectious agents are found in faeces (stool) and enter the body through the mouth (oral route). The mode of transmission may be in contaminated food or water, on the hands, or on objects such as bowls, spoons and cups. For simplicity, we will sometimes refer to these diseases as faeco-oral diseases.
In this study session, you will learn about the general features of faeco-oral diseases: the main types commonly found in Ethiopia, their general symptoms and signs, how to treat mild cases and when to refer patients with severe conditions for specialised treatment, or laboratory tests to confirm the diagnosis. You will also learn about the importance of giving effective health education to your community on ways to prevent and control faeco-oral diseases. This general understanding forms the basis for the more detailed discussion of specific faeco-oral diseases in Study Sessions 33 and 34.
Learning Outcomes for Study Session 32
When you have studied this session, you should be able to:
32.1 Define and use correctly all of the key words printed in bold. (SAQs 32.1, 32.3 and 32.4)
32.2 Name the common types of faeco-orally transmitted diseases in Ethiopia, the infectious agents that cause them, and the main routes of transmission. (SAQs 32.1, 32.2 and 32.4)
32.3 Describe the characteristic symptoms and signs of faeco-oral diseases, and explain why diarrhoea can be life-threatening. (SAQ 32.3)
32.4 Describe how you would treat mild cases of faeco-oral disease, and when you would refer severe cases for laboratory investigation and/or specialised treatment. (SAQ 32.3)
32.5 Suggest effective ways to prevent and control faeco-oral diseases at the community level. (SAQs 32.2 and 32.4)
32.1 Classification of faeco-oral diseases and their infectious agents
Faeco-oral diseases can be caused by a wide range of infectious agents, including bacteria, viruses, protozoa (single-celled parasites) and helminths (parasitic worms). All human parasites, whether they are single-celled or many-celled, live inside the human body: some are harmless, but others cause disease. In this study session, we are concerned with infectious agents which are transmitted via the faeco-oral route.
Can you think of a viral disease that you learned about in Part 1 of this Module, which is transmitted faeco-orally?
Poliomyelitis (polio) is a viral faeco-orally transmitted disease, which was described in detail in Study Session 4.
You already know about polio, which has become rare in Ethiopia thanks to the immunization programme, so we will not discuss it again here. Table 32.1 lists the common faeco-oral diseases and where they are described in detail later in this Module. You may already know about some of them from your own experience in your community.
| Faeco-oral disease | Infectious agent | Study Session |
|---|---|---|
| Bacteria: | ||
| Cholera | Vibrio cholerae | 33 |
| Shigellosis (bacillary dysentery) | Shigella species | 33 |
| Typhoid fever | Salmonella typhii | 33 |
| Viruses: | ||
| Viral diarrhoeal diseases | Rotavirus (most cases) | 33 |
| Amoebiasis (Amoebiasis is pronounced ‘am-mee-bya-sis’) (amoebic dysentery) | Entamoeba hystolica | 34 |
| Giardiasis (giardiasis is ‘jee-arr-dya-sis’) | Giardia intestinalis | 34 |
| Helminths: | ||
| Ascariasis (ascariasis is ‘ass-kar-rya-sis’) | Ascaris lumbricoides | 34 |
| Hookworm | Necator americanus or Ankylostoma duodenalis | 34 |
| Taeniasis (taeniasis is ‘tee-nya-sis’) m(tapeworm) | Taenia saginata (most cases) | 38 |
32.2 Direct and indirect faeco-oral transmission
As we mentioned in the Introduction to this study session, faeco-oral transmission means ‘from faeces to mouth’. But the route can either be direct transmission from contaminated hands touching the mouth and transferring the infectious agents directly; or indirect transmission through consumption of food or water, or using utensils, contaminated with the infectious agents.
How could a person’s hands become contaminated with faeces?
You may have thought of several ways, including:
- Using the toilet and not washing the hands afterwards
- Cleaning a child’s bottom after defaecation
- Shaking hands with someone whose hand is already contaminated (Figure 32.1)
 Figure 32.1 Contaminated hands can easily transmit infectious agents directly to the mouth. (Photo: Basiro Davey)
Figure 32.1 Contaminated hands can easily transmit infectious agents directly to the mouth. (Photo: Basiro Davey)- When flies rest on the hand after they have crawled on faeces
- Accidentally touching faeces in the soil where people or animals have defaecated in the open fields.
Faeces can also contaminate food or water, indirectly transmitting the infectious agents when a person eats the food, or drinks the water, or some gets into the mouth during washing. Diseases transmitted indirectly by food or water are called foodborne diseases and waterborne diseases respectively (see Box 2.2 in Study Session 2).
Can you suggest some ways that food could become contaminated with faeces?
You may have thought of several ways, including:
- Contaminated hands touching food during preparation or eating
- Using contaminated water to prepare food (e.g. washing fruit)
- Using contaminated utensils (knife, spoon, bowl, etc.) to prepare or eat food
- Feeding a baby with contaminated milk, or using a contaminated bottle
- Flies resting on food after crawling over faeces
- Serving inadequately cooked fruit and vegetables grown in soil contaminated with faeces.
How could water become contaminated with faeces?
The correct construction of latrines is taught in the Hygiene and Environmental Health Module.
You may have thought of several ways, including:
- Sources of water (streams, wells, etc.) can be contaminated with faeces washed out of the soil by heavy rain if people defaecate in open fields, or in poorly constructed latrines
- Hands or utensils for eating or drinking may be washed in contaminated water
- Contaminated containers may be used to fetch or store water.
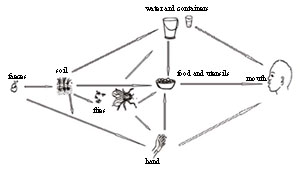
The examples given above illustrate faeco-oral transmission via the six Fs: food, fingers, flies, fluids, faeces and fomites. Figure 32.2 illustrates the different ways that faeco-oral transmission can occur.
Fomites (‘foh-mytz’) is the term given to non-living things (e.g. bowls, water containers, soil) that can transmit infection indirectly.
32.3 Symptoms and signs of faeco-oral diseases
Most – but not all – faeco-oral diseases have diarrhoea as their main symptom, and for this reason these conditions are also known as diarrhoeal diseases. Other common symptoms are vomiting, abdominal pain, and sweating or shivering. A high-grade fever is a sign of some faeco-oral diseases, i.e. a temperature of 38.5oC or above, measured with a thermometer. Of the diseases listed in Table 32.1 earlier, all except typhoid fever, ascariasis and taeniasis are characterised by diarrhoea. As it is such a common symptom of so many faeco-oral diseases, we will focus on diarrhoea in more detail.
32.3.1 Diarrhoea
Diarrhoea is the passage of loose faeces (liquid stool) three or more times a day, or more than is normal for the individual. If the diarrhoea continues for less than 14 days, it is referred to as acute diarrhoea; if it lasts for more than 14 days it is said to be chronic or persistent diarrhoea. Diarrhoea is also distinguished into acute watery diarrhoea (sometimes abbreviated to AWD), which typically occurs in cases of cholera, and bloody diarrhoea (also known as dysentery), which typically occurs in cases of shigellosis and amoebiasis.
![]() Severe or some dehydration in a child is life-threatening. Refer the child urgently to the nearest health centre or hospital, telling the carer to feed sips of fluid to the child on the way.
Severe or some dehydration in a child is life-threatening. Refer the child urgently to the nearest health centre or hospital, telling the carer to feed sips of fluid to the child on the way.
Diarrhoea results in dehydration – the rapid loss of body fluids and important salts required for proper control of body functions, particularly in the brain, nerves and muscles. Children are highly susceptible to dehydration if they have diarrhoea, even after only one day; they can quickly die if the fluid loss is continuous and cannot be replaced by drinking fluids. A sign of some degree of dehydration in a child with diarrhoea is if it seems restless and irritable (easily upset), and drinks eagerly if offered fluids. If the dehydration is severe, the child may be too lethargic to drink, the eyes often appear sunken, and if you pinch the skin on the child’s abdomen it may take two seconds or more for the pinched skin to go back to the normal position.
32.3.2 How common are diarrhoeal diseases?

Diarrhoeal diseases are the second largest cause of death globally among children aged under five years – only pneumonia and other acute respiratory infections (ARIs, the subject of Study Session 35) account for more child deaths worldwide. The World Health Organization (WHO) estimates that 1.5 million children in this age group die from diarrhoeal diseases every year, almost half of them in Africa. The most vulnerable children are the youngest ones, particularly before their second birthday. In Ethiopia, 23% of deaths in children aged under five years is due to diarrhoeal diseases – around 73,000 such deaths every year. Diarrhoeal diseases kill more children than malaria, HIV/AIDS and measles combined.
Why do you think children are especially likely to be infected with the organisms that cause diarrhoeal diseases?
There are many reasons, but you may have suggested that children are less likely than adults to wash their hands after defaecating, and more likely to put their fingers or dirty objects into their mouths, and also more likely to play in soil where they may come into contact with faeces.
32.4 Diagnosis and treatment of faeco-oral diseases
32.4.1 Diagnosis
The diagnosis of diarrhoeal diseases in children is further discussed in the Module on the Integrated Management of Newborn and Childhood Illness (IMNCI).
To be certain that the cause of a faeco-oral disease has been correctly diagnosed, identified the infectious agent can only be done using laboratory techniques. However, identification of the infectious agent is not needed for the correct treatment of most cases of children with mild episodes of watery diarrhoea, which is evident in the majority of the faeco-oral diseases you will come across in your work.
For adults, laboratory examination is required to diagnose faeco-oral diseases accurately. At Health Post level, you should base your diagnosis on the specific symptoms and signs, for example, whether there is diarrhoea and (if yes) is it watery or bloody, and does it have a foul smell? Is the patient vomiting or complaining of abdominal pain? Does the patient have a fever? If your diagnosis is ascariasis, you can treat the adult patient as described in Study Session 34. But if you suspect other types of faeco-oral diseases (e.g. cholera, typhoid fever), refer the patient to the nearest higher level health facility, sending a referral note stating that further diagnosis is needed before specific treatment can begin. How to make or suspect a diagnosis of specific faeco-oral diseases will be discussed in Study Sessions 33 and 34, when we talk in more detail about types that you may encounter in your community.
32.4.2 Treatment
The treatment of any faeco-oral disease depends on whether the patient has diarrhoea or not. Patients without diarrhoea are treated depending on the type of infectious agent responsible, and you will learn more about the specific treatments for each condition in Study Sessions 33 and 34.
For patients with diarrhoea, especially children, the core measure in the treatment is rapid and adequate rehydration – fluid replacement – usually by drinking fluids. In the most severe cases the fluid has to be given intravenously (directly into a vein). Rehydration is the most important component of treatment for diarrhoea and it should be started as soon as possible and continued for as long as necessary. The best fluid to use to avoid the dangers of dehydration is a solution of oral rehydration salts (ORS) – a packet containing sugar and salts in the correct amounts, which the caregiver dissolves in clean drinking water. The sugar and salts are absorbed into the child’s body, replacing what it has lost in the diarrhoea; the salts also help water to be absorbed across the inflamed lining of the gut, where it has been damaged by the action of infectious agents. WHO Guidelines on the Treatment of Diarrhoea now also emphasise the importance of giving zinc supplements to young children with diarrhoea, in addition to ORS.
For children with diarrhoea, the measures that you need to undertake during treatment are briefly summarised in Box 32.1. However, the WHO estimates that less than 40% of children with a diarrhoeal disease receive the correct treatment.
Box 32.1 Summary of the main measures to treat a child with diarrhoea
In order to treat a child with diarrhoea effectively, you have to learn the detailed descriptions of each of these measures, which are discussed in the IMNCI Module, Study Session 5.
- First, you have to assess the degree of dehydration and classify the child as having ‘no’, ‘some’ or ‘severe’ dehydration, depending on specific symptoms and signs.
- Select and apply the appropriate treatment for the degree of dehydration.
- Check for other general danger signs indicating other major health problems, such as malaria, malnutrition or pneumonia, and treat them; e.g. if the child has malaria, give appropriate antimalarial drugs (refer back to Study Session 8 of this Module).
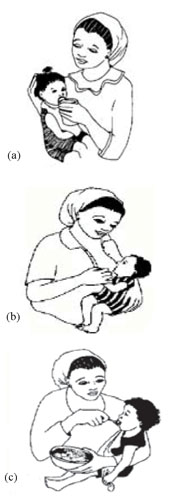
- Counsel the mother on how to give ORS at home (Figure 32.3a); if she does not have ORS, the child should be encouraged to drink as much clean fluids as possible.
- If the child is breastfed, the mother should go on breastfeeding during diarrhoea episodes (Figure 32.3b); weaned children need additional nourishing meals to help them recover their strength (Figure 32.3c).
For adults with diarrhoea, assess whether the patient can take fluids orally, and if they cannot, refer them immediately to the nearest higher level health facility. If the patient is able to take fluids orally, give ORS and tell them to drink 200–400 ml after each loose stool. You should also advise the patient to take other fluids in addition to ORS and to continue eating. For most cases of diarrhoea in adults, additional treatment (other than rehydration) is generally required – mainly giving an antibiotic or other medication appropriate for the specific infectious agent. However, laboratory examination of stool samples is required before making the diagnosis, which can’t be carried out at Health Post level. Therefore, give ORS to adults with diarrhoea and refer them. Advise the patient that early treatment is important because the disease could worsen rapidly.
32.5 Prevention and control of faeco-oral diseases
Effective prevention and control measures can interrupt faeco-oral transmission of infectious agents by targeting the different routes of transmission mentioned earlier and summarised in Figure 32.2. As you remember, the sources and modes of transmission to be targeted are: hands, food, water, utensils, soil and flies contaminated with faeces. Most of the prevention and control measures are relatively simple and easy to apply. You have an important role in educating your community by explaining what simple steps can be taken to reduce the risk of faeco-oral diseases. So, in addition to the effective treatment of cases, you need to help families put into effect the measures outlined below.
32.5.1 Prevention of faeco-oral transmission
Give clear health education messages in ways that motivate people in your community to undertake the prevention and control measures described below. Each measure has been given a distinguishing letter, so you can relate it to the questions that follow the descriptions.
Ways to prevent faecal contamination of hands
| A | Wash hands with soap and clean water: | |
| A1 | After defaecation, or cleaning the bottom of a child, or changing an infant’s nappy (diaper). | |
| A2 | After working with soil, or after children have been playing on soil, where there has been open defaecation by people or animals. | |
| A3 | Before preparing food or eating. | |
| B | Cut fingernails and avoid putting fingers into the mouth. | |
Ways to prevent contamination from unsafe food
| C | Prepare and eat food safely: | |
| C1 | Observe thorough hand hygiene before and during any contact with food | |
| C2 | Ensure that all utensils are completely clean; allow them to ‘air dry’ after washing (don’t wipe with a cloth) | |
| C3 | Wash raw vegetables and fruits thoroughly in clean water | |
| C4 | Cook other food items thoroughly, particularly meat and fish | |
| C5 | Eat cooked food while it is hot and reheat food thoroughly if it has cooled | |
| C6 | Cover food so it cannot be exposed to flies. | |
| D | Promote exclusive breastfeeding of infants under six months old: | |
| D1 | If babies or young children are fed animal milk or formula, the bottle and teat, or cup and spoon, should be thoroughly washed with clean water and soap before every feed | |
| D2 | Animal milk should be boiled and cooled before drinking | |
| D3 | Formula milk should be mixed with boiled cooled water. | |
| E | Control flies: | |
| E1 | Cover food to prevent contamination by flies | |
| E2 | Dispose of faeces and other wastes safely, so flies cannot land on sewage. | |
Ways to prevent contamination from unsafe water
| F | Protect water sources from contamination with faeces: | |
| F1 | Use a properly constructed latrine and safe disposal of faeces | |
| F2 | Avoid open defaecation in the fields (Figure 32.4) | |
| F3 | Avoid direct contact of hands with drinking water | |
| F4 | Install protected water sources, such as covered wells with pumps | |
| G | Boil water before drinking, or using in preparation of food or fluids | |
| H | Use clean drinking cups and clean covered containers for storing water. | |
Which of the measures described above will help to prevent the transmission of infectious agents by flies? Use the letters assigned to each measure to indicate your answers.
Measures C6, E1, E2, F1 and F2 will all reduce the risk of faeco-oral diseases transmitted by flies.
Which of the measures described above are most important when preparing milk for feeding to young children?
Measures A1, A2, A3, B, C1, C2, D1, D2, D3, G and H.
32.5.2 Other ways to reduce the risks of faeco-oral diseases
Feeding young children before, during and after illness is described in detail in the Nutrition Module.
In addition to interrupting the direct and indirect transmission of infectious agents, the risk of faeco-oral diseases can be reduced by other ways of protecting and promoting general health, particularly of children. Malnutrition increases the susceptibility of children to develop severe symptoms if they are exposed to infection. Therefore, exclusive breastfeeding until the age of six months and good nutrition after weaning can help to protect children from infection and increase their resistance to the most severe symptoms if they become ill. Eating additional nourishing meals also aids recovery after illness.
Immunization is described in Study Sessions 3 and 4 of this Module, and in the Immunization Module
Immunization against all the vaccine-preventable diseases also promotes the general health of children and helps to protect them from faeco-oral diseases (Figure 32.5). A child who is suffering from a condition such as measles or pneumonia is also more vulnerable to develop a faeco-oral disease, because their immune system is overloaded by infection. Giving vitamin A supplements with the measles vaccine at the age of nine months, and every six months thereafter until the age of five years, also helps to promote health and increase resistance to infection. So, ensuring that parents and other caregivers know about and follow all these good practices can help to reduce the risks to children from faeco-oral diseases. A vaccine to protect children against rotavirus infection – the main cause of viral diarrhoeal disease – is expected to be added to the routine Expanded Programme on Immunization (EPI) in the near future.

In the next two study sessions, we will discuss specific types of faeco-oral diseases caused by bacteria and viruses (Study Session 33) and protozoa (Study Session 34); helminths that cause faeco-oral diseases are described in Study Sessions 34 and 38.
Summary of Study Session 32
In Study Session 32, you have learned that:
- Faeco-oral diseases are caused by infectious agents whose route of exit from the body is in the faeces, and whose route of entry to new hosts is via the mouth.
- Faeco-oral diseases can be caused by bacteria, viruses, protozoa and helminths.
- Transmission of the infectious agents that cause faeco-oral diseases can be by the direct route, when hands contaminated with faeces make contact with the mouth. Indirect transmission is via contaminated food, water, soil, utensils or flies.
- The common symptoms and signs of most faeco-oral diseases can include diarrhoea, vomiting, abdominal pain and fever or shivering.
- Diarrhoea in different faeco-oral diseases may be acute or persistent (chronic), watery or bloody.
- Young children are particularly vulnerable to dehydration (loss of body fluids and salts) due to diarrhoeal diseases. Diarrhoea is the second most important cause of death among children aged under five years.
- The key to the treatment of diarrhoeal diseases is rehydration with oral rehydration salts (ORS), which should be given to the patient until all diarrhoea has ceased. Zinc supplements for affected children are also recommended by the WHO.
- Prevention and control measures include handwashing with soap and clean water; safe preparation and serving of food; thorough cleaning of all cooking, drinking and eating utensils, and containers for drinking and storing water; safe disposal of faeces and other wastes, use of latrines, and protection of water sources from contamination (e.g. by avoiding open defaecation in fields); and control of flies.
- Other protective measures include exclusive breastfeeding for all infants until the age of six months, feeding children adequate nourishing food to prevent malnutrition and immunization against vaccine-preventable diseases.
Self-Assessment Questions (SAQs) for Study Session 32
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering the questions below. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 32.1 (tests Learning Outcomes 32.1 and 32.2)
Which type of infectious agent is the cause of each of the following faeco-oral diseases?
| A Poliomyelitis | E Cholera |
| B Shigellosis | F Taeniasis |
| C Giardiasis | G Amoebiasis |
| D Ascariasis |
Answer
A Poliomyelitis is caused by the poliovirus
B and E Shigellosis and cholera are both caused by bacteria
C and G Giardiasis and amoebiasis are caused by protozoa parasites
D and F Ascariasis and taeniasis are caused by helminths (worms).
SAQ 32.2 (tests Learning Outcomes 32.2 and 32.5)
Suppose that in the community you are working in, most people defaecate in the open fields.
- a.How will this increase the transmission of faeco-oral diseases?
- b.What prevention measures would you encourage this community to apply to reduce the risks?
Answer
- a.Defaecation in the open fields increases the risk of faeco-oral diseases occurring because the soil becomes contaminated with the causal infectious agents. Infection can be transmitted to susceptible members of the community in several ways: via unwashed hands after defaecation, working or playing in the soil; unwashed or inadequately cooked fruit and vegetables grown in contaminated soil; and via flies crawling on faeces and then landing on food, utensils or hands.
- b.The prevention measures that this community could apply to reduce the risks are to build latrines for every household, dispose of faeces and other wastes safely, avoid open defaecation in fields, and adopt hygienic practices such as thorough handwashing and safe preparation of food.
SAQ 32.3 (tests Learning Outcomes 32.1, 32.3 and 32.4)
A mother brings a two-year-old boy to your Health Post and tells you that he has been passing loose watery stools several times a day for the last ten days. She has not seen any blood in the stools. The child appears lethargic, his eyes are sunken, he is not interested in drinking, and when you pinch the skin of his abdomen it takes more than two seconds for the skin to return to the normal position.
- a.How should this child’s condition be classified?
- b.What actions should you take?
- c.What will you explain to the mother about her child’s condition?
Answer
- a.This child is suffering from acute watery diarrhoea with signs of severe dehydration.
- b.You should advise the mother to take him to a health centre or hospital urgently. Give her enough ORS solution for the journey and tell her to feed sips of it to the child on the way. Go with them if you can, or send a clearly written referral note.
- c.Explain to the mother that the child’s body has lost so much fluid and salts that his body systems are no longer functioning normally and his condition is potentially life-threatening. This is why he appears lethargic, his eyes are sunken, and his skin doesn’t go back quickly when pinched.
SAQ 32.4 (tests Learning Outcomes 32.2 and 32.5)
A village proudly installs a protected pump to improve the safety of its water source. What other measures could they take to reduce the indirect transmission of faeco-oral diseases via contaminated water?
Answer
In addition to installing the protected water pump, the villagers should also use clean containers to collect and store water and clean drinking cups; wash their hands regularly and avoid their hands touching drinking water; and boil water before drinking it, or using it to wash fruit and vegetables, or mixing formula milk for babies. These measures will reduce the indirect transmission of faeco-oral diseases by contaminated water.