Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Tuesday, 28 July 2026, 8:13 PM
Labour and Delivery Care Module: 6. Active Management of the Third Stage of Labour
Study Session 6 Active Management of the Third Stage of Labour
Introduction
In the final study session of this Module, you will learn about postpartum haemorrhage (PPH), which is a leading cause of maternal mortality, responsible for about a quarter of all maternal deaths. Worldwide, around 127,000 women every year die of postpartum haemorrhage. The majority of these fatal cases of excessive bleeding occur in the first 24 hours after delivery of the baby, as a result of complications arising during the third stage of labour. To minimise the risks of PPH in this critical stage of labour, a set of procedures have been developed that all birth attendants should follow, called active management of third stage of labour (AMTSL). Correctly applied, AMSTL can reduce the risk of postpartum haemorrhage by more than 60%.
In this study session, you will learn what is meant by AMTSL and the procedures you will conduct during each of its six steps. This knowledge will help you to identify the complications that may arise during the third stage of labour and manage them more effectively.
Learning Outcomes for Study Session 6
When you have studied this session, you should be able to:
6.1 Define and use correctly all of the key words printed in bold. (SAQ 6.1)
6.2 Explain the natural physiological process of placental delivery. (SAQ 6.1)
6.3 Describe the six steps of active management of third stage of labour (AMTSL). (SAQ 6.2)
6.4 Summarise the regimens for each of the uterotonic drugs used in AMTSL. (SAQs 6.2 and 6.3)
6.5 Explain how you would examine the placenta and membranes for completeness. (SAQ 6.3)
6.6 Describe the warning signs for complications that may arise during the third stage of labour. (SAQ 6.4)
6.1 The third stage of labour
The third stage of labour begins with the birth of the baby and ends with the delivery of the placenta and fetal membranes. Normally, it should last less than 30 minutes.
6.1.1 Natural processes during the third stage
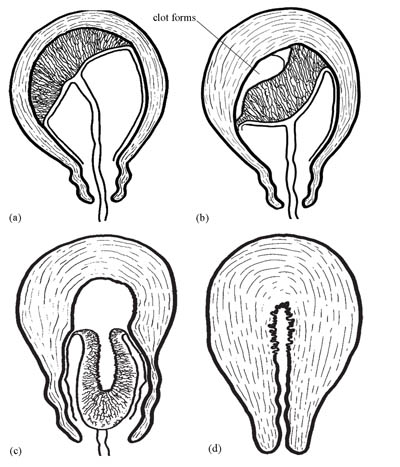
In a complication-free labour, the third stage is when natural physiological processes spontaneously deliver the placenta and fetal membranes. For this to happen unproblematically, the cervix must remain open and there needs to be good uterine contraction. In the majority of cases, the processes occur in the following order:
- Separation of the placenta: The placenta separates from the wall of uterus (see Figure 6.1a and b). As it detaches, blood from the tiny vessels in the placental bed begins to clot between the placenta and the muscular wall of the uterus (the myometrium).
- Descent of the placenta: After separation, the placenta moves down the birth canal and through the dilated cervix (see Figure 6.1c).
- Expulsion of the placenta: The placenta is completely expelled from the birth canal (see Figure 6.1d).
This expulsion marks the end of the third stage of labour. Thereafter, the muscles of the uterus continue to contract powerfully and thus compress the torn blood vessels. This, (together with blood clotting) quickly reduces and stops the postpartum bleeding.
6.1.2 Complications occurring during the third stage of labour
Study Session 11 of this Module will tell you in detail about postpartum haemorrhage and atonic uterus; the other terms in Box 6.1 are covered in this study session.
Women who give birth unattended by a skilled healthcare provider (like you) are more likely to experience complications at all stages of labour, including the third stage. These complications are listed in Box 6.1 below. They can arise even in a delivery where the placenta was implanted in a good position in the top two-thirds of the uterus, labour was not prolonged and the birth was normal. In such cases, while a normal and spontaneous delivery of the placenta during the third stage might be expected, complications can still arise unpredictably. You should always be prepared for the unexpected emergency.
Box 6.1 Common complications of third stage of labour
All these complications are much more likely to occur if the third stage is not properly managed, using the AMTSL approach.
Retained placenta
The placenta remains inside the uterus for longer than 30 minutes after delivery of the baby, usually due to one or more of the following:
- Uterine contractions may be inadequate to expel the placenta
- The cervix might have retracted too fast and partially closed, trapping the placenta in the uterus
- The bladder may be full and obstructing placental delivery.
Excessive bleeding (PPH)
PPH is the loss of more than 500 ml of blood following delivery of the baby. Most bleeding comes from where the placenta was attached to the uterus, and is bright or dark blood and usually thick. PPH occurs when the uterus fails to contract well, usually due to:
- Partially separated placenta (it remains partly attached to the uterine wall
- Completely separated placenta, but retained inside the uterus
- Atonic uterus; the muscular wall of the uterus could not contract powerfully enough to arrest the natural bleeding which occurs when the placenta separates.
Uterine inversion
The uterus is pulled ‘inside out’ as the baby or the placenta is delivered, and partly emerges through the vagina.
6.2 Active management of third stage of labour (AMTSL)
A birth attendant applying active management of third stage of labour (AMTSL) is the key to reducing the risk of the complications set out in Box 6.1. The term ‘active management’ indicates that you are not waiting for spontaneous placental delivery. Rather, you will intervene in a carefully programmed sequential manner, as follows:
- As soon as the baby is delivered, put it on the mother’s abdomen in skin-to-skin contact with her. Cover them with a blanket.
- Clamp the baby’s umbilical cord at two sites and cut it in between, as you learned to do in Study Session 5.
- Then follow the steps in Box 6.2. We describe each of them in detail in the next section.
Box 6.2 The six steps of AMTSL in sequence
- Check the uterus for the presence of a second baby.
- In less than one minute, administer a uterotonic drug (a hormone-like chemical that makes the uterus contract more powerfully).
- Apply controlled cord traction.
- After delivery of the placenta, immediately start massaging the uterus.
- Examine the placenta to make sure it is complete and none of it has been retained in the uterus.
- Examine the woman’s vagina, perineum and external genitalia for lacerations and active bleeding.
Step 1 Check the uterus – is there a second baby?
Immediately after the birth of the baby, check for the presence of a second baby by palpating the uterus through the mother’s abdomen. When you feel certain that the uterus does not contain a second baby, and you can feel that it has reduced in size to no larger than at 24 weeks of gestation, go to step 2. The reason for checking so carefully is because the drug you will administer to the mother in step 2 will make the uterus contract so powerfully that it will damage a baby that remains inside it. If you find that there is a twin, give the the uterotonic drug after the birth of the second baby.
Step 2 Administer a uterotonic drug to help the uterus contract
The commonly used uterotonic drugs in obstetric practice are:
- misoprostol (tablets)
- oxytocin (injectable)
- ergometrine (injectable).
These drugs help the uterus to continue contracting strongly and rhythmically after the baby is born: they facilitate placental delivery and help to prevent excessive bleeding from a relaxed (atonic) uterus. Although there are three possible drugs, for deliveries in low-resource settings, such as homes in rural areas of Ethiopia, on many occasions misoprostol may be the only one of these drugs that you will be able to use. Oxytocin is the drug recommended by the World Health Organization (WHO), but it may not be practical for the following reason:
Health Posts are supplied with a refrigerator and mobile icebox for transport of vaccines to outreach events, as described in the Immunization Module.
Oxytocin and ergometrine always have to be kept refrigerated at 2–8°C, so they are not suitable for a home delivery unless the household has a refrigerator, or you have a mobile icebox. They also have to be protected from exposure to light.
Dosages of uterotonic drugs
In less than one minute after the delivery of the baby, and after clamping and cutting the umbilical cord, give the mother one of the following:
- misoprostol 600 micrograms (µg), i.e. three 200 µg tablets by mouth with a drink of water.
OR (if you carry this in an icebox)
- oxytocin 10 international units (IU) injected deep into the woman’s thigh muscles (intramuscular injection, IM).
OR
- ergometrine 0.4–0.5 milligrams (mg) injected deep into the woman’s thigh muscles (intramuscular injection, IM).
When the uterus is well contracted it will feel very hard. This should occur between 2–7 minutes after the administration of the drug, depending on which one is given.
Note that ergometrine is not recommended for use by rural Health Extension Practitioners.
Advantages and disadvantages of the uterotonic drugs
Misoprostol is less effective than oxytocin and has more side-effects. However, in many rural situations you will have no other option but to use it because of the need to store oxytocin in a refrigerator or icebox. It will be important therefore to advise the mother that while it will be effective in preventing bleeding, she may also experience some side-effects. This applies whichever uterotonic drug you are giving, but especially in the case of misoprostol, which causes side-effects in a significant proportion of women. They are:
- Shivering: this may start 1 hour after taking misoprostol and will subside after 2–6 hours. Ask the family to offer the mother warm tea or ‘atmit’, as well as blankets.
- Fever: this is rarer, but may start after the shivering. It is not necessarily a sign of infection and it will disappear within 2–8 hours after taking the drug.
- Diarrhoea: may also occur and normally lasts less than a day.
- Nausea and vomiting: can also occur, but will subside 2–6 hours afterwards.
What is the great advantage that misoprotol has compared to the other uterotonic drugs?
It comes in tablet form, so injection equipment (syringes, needles) are not required, and it does not need to be stored in a refrigerator so it can be used where there is no way of keeping drugs very cold.
Oxytocin is the recommended uterotonic drug in all situations where it is feasible to use it, because it is more effective than the other drugs and has fewer side-effects. Oxytocin is a naturally occurring hormone in the woman’s body, which is involved in the onset and progression of uterine contractions during labour. Manufactured oxytocin is given after the delivery to ensure that the uterus goes on contracting rhythmically, like natural uterine contractions. However, it does not have a sustained action (the effect subsides quite quickly) and it must be stored in a refrigerator and protected from light.
Ergometrine is less widely used because it is such a strong uterotonic drug that it may hasten the closure of the cervix before the delivery of the placenta. It takes longer to act than oxytocin (6–7 minutes when given intramuscularly) and it causes marked spasm of the uterus by a series of rapid sustained contractions, which are unlike the natural uterine contractions. However, it is long-lasting, with an effect over approximately 2–4 hours.
![]() It is not planned to use ergometrine in the rural Health Extension Service. It must never be given to a woman with pre-eclampsia, eclampsia or high blood pressure, because it causes the blood vessels to constrict, forcing her blood pressure even higher.
It is not planned to use ergometrine in the rural Health Extension Service. It must never be given to a woman with pre-eclampsia, eclampsia or high blood pressure, because it causes the blood vessels to constrict, forcing her blood pressure even higher.
Step 3 Apply controlled cord traction with counter-pressure
When the uterus is well contracted it will feel very hard. This should occur 2–3 minutes after the administration of one of the uterotonic drugs. Then controlled cord traction with counter pressure is used to help to expel the placenta (see Figure 6.2 and Box 6.3).
![]() To avoid inversion of the uterus (turning inside out and coming out of the vagina), controlled cord traction should NEVER be applied without counter-pressure to the abdomen.
To avoid inversion of the uterus (turning inside out and coming out of the vagina), controlled cord traction should NEVER be applied without counter-pressure to the abdomen.

Box 6.3 How to do controlled cord traction with counter-pressure
- Clamp the umbilical cord close to the perineum (once pulsation of the blood vessels stops in the cord of a healthy newborn) and hold the cord in one hand.
- Place the other hand just above the woman’s pubic bone and stabilise the uterus by applying counter-pressure to the abdomen during controlled cord traction.
- Keep slight tension on the cord and await a strong uterine contraction (usually every 2–3 minutes).
- With the strong uterine contraction, encourage the mother to push and very gently pull downward on the cord to deliver the placenta. Continue to apply counter-pressure to the uterus.
- Between contractions, gently hold the cord and wait until the uterus is well contracted again.
- With the next contraction, repeat controlled cord traction with counter-pressure.
- If the placenta does not descend during 30–40 seconds of controlled cord traction do not continue to pull on the cord.
The following actions complete the rest of the delivery of the placenta.
As the placenta is delivered, it should be caught in both hands at the vulva to prevent the membranes tearing and some being left behind. Hold the placenta in two hands and gently turn it until the membranes are twisted (see Figure 6.3). Slowly pull to complete the delivery of the placenta.

Delivery of the placenta marks the end of the third stage of labour. At this time the uterus should be hard, round and movable when you palpate the abdomen. You should be able to feel it midway between the mother’s umbilicus (belly button) and her pubic bone. There should be no bleeding from the vagina. The bladder should be empty.
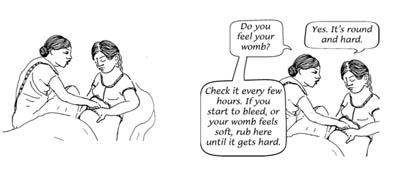
Step 4 Massage the uterus
Right after the placenta is delivered, rubbing the uterus is a good way to contract it and stop the bleeding. Many women need their uterus rubbed to help it to contract (Figure 6.4).
Step 5 Examine the placenta and fetal membranes
You must look carefully at the placenta to be sure that none of it is missing.
From your knowledge of the anatomy of the placenta (Antenatal Care Module, Study Session 5), which is the ‘maternal’ surface — the top side where the umbilical cord emerges, or the underside (bottom) of the pelvis?
The maternal surface of the placenta is the underside, opposite to the side where the umbilical cord emerges.
If a portion of the maternal surface (bottom of the placenta, see Figure 6.5) is missing, or there are torn membranes with blood vessels, suspect that retained placenta fragments remain in the uterus and refer the mother quickly.
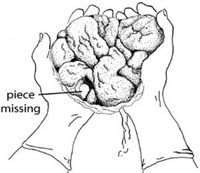

Can you explain why?
She is more at risk of postpartum haemorrhage if a piece of the placenta is retained in the uterus.
The irregular rounded shapes on the underside of the placenta are called lobes (some textbooks call them cotyledons). By contrast the top of the placenta (the side that was facing the baby) is smooth and shiny. The cord attaches on this side, and then spreads out into many deep-blue blood vessels that look like tree roots (Figure 6.6).
Checking the placenta for completeness
- Hold the placenta in the palms of your hands, with the maternal side facing upward. Make sure that all the lobules are present and fit together.
- Then hold the cord with one hand, allowing the placenta and membranes to hang down.
- Place the other hand inside the membranes, spreading the fingers out, to make sure that the membranes are complete (Figure 6.7).
 Figure 6.7 Hold the membranes open like this to check they are complete.
Figure 6.7 Hold the membranes open like this to check they are complete. - Ensure that the position of cord attachment to the placenta is normal, and inspect the cut end of the cord for the presence of two arteries and one vein (Figure 6.8).
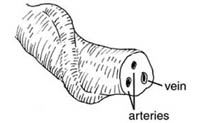 Figure 6.8 The cut end of the cord has two arteries and one vein.
Figure 6.8 The cut end of the cord has two arteries and one vein. - Safely dispose of the placenta by either burying it where it will not be dug up by animals, or incinerate it if you have the facilities to do so in your community.
- If the membranes tear, gently examine the upper vagina and cervix of the woman. You must wear sterile/disinfected gloves and use a sponge forceps to remove any pieces of membrane that are present.
It is dangerous for the mother if any parts of the placenta or membranes are left behind in the uterus.

Step 6 Examining for cuts, tears and bleeding

The anatomical terms in this section were all explained and illustrated in Study Session 3 of the Antenatal Care Module, Part 1 (see Figure 3.2). To complete the management of the third stage of labour, do the following:
- Gently separate the labia and inspect the lower vagina and perineum for lacerations that may need to be repaired to prevent further blood loss (Figure 6.10).
- Gently cleanse the vulva and perineum with boiled (then cooled) warm water or a weak antiseptic solution.
- Apply a clean pad or cloth with firm pressure to the area that is bleeding for about 10 minutes. If bleeding continues after this time, refer the woman immediately, keeping the pressure applied to the wound.
- Monitor the woman every 15 minutes - this means measuring her vital signs, massaging her uterus to ensure that it is contracted and checking for excessive vaginal bleeding.
Why is it important to complete the six steps of AMTSL in a particular order and what is that order?
Keeping to the exact order of actions is important, because the evidence on which AMTSL is based shows that if it is correctly applied (including in the right order) it can reduce the risk of PPH by 60%. Refer back to Box 6.2 if you can’t remember the order of the six steps.
6.3 Intervention in complications after applying AMTSL
6.3.1 Excessive bleeding (postpartum haemorrhage or PPH)
You will learn the definition of excessive bleeding and the actions to take if the woman has postpartum haemorrhage (PPH) in Study Session 11 of this Module; it also describes the interventions you can take during and after the third stage of labour to reduce the risk of PPH. The main points are summarised briefly here.
- Rubbing the uterus and (if you have been trained to do it) using the two-handed pressure method (Study Session 11).
- Giving a second dose of oxytocin 10 IU by intramuscular injection, or a second dose of misoprostol 400 µg rectally (by pushing the tablets gently into the rectum through the woman's anus), or by putting the tablets under her tongue where they can slowly dissolve.
- Initiating breastfeeding immediately after delivery: the contractions that expel the milk will also make the uterus contract.
Remember not to exceed 1,000 µg of misoprostol (5 tablets). If the woman has already taken 600 µg (3 tablets) after the birth of the baby, and she needs a second dose because of excessive bleeding, it should be no more than 400 µg (2 tablets) via the rectum. This way, the woman will have fewer side-effects. If she did not take 600 µg of oral misoprostol after the birth of the baby and has signs of excessive bleeding, give her 1,000 µg of misoprostol via the rectum in one dose.
Do not give additional misoprostol if oxytocin was the drug used originally.
![]() If excessive bleeding occurs, the mother should be taken to the health facility immediately. You will learn what to do on the journey in Study Session 11.
If excessive bleeding occurs, the mother should be taken to the health facility immediately. You will learn what to do on the journey in Study Session 11.
If the bleeding does not stop quickly after the second dose of misoprostol, then refer the woman to the nearest health facility urgently. Sometimes, bleeding comes from a torn vagina, a torn cervix, or a torn uterus. Usually this bleeding comes in a constant, slow trickle. The blood is usually bright red and thin. Actions to take while waiting for transport:
- Lie the mother down with her feet higher than her head and her head turned sideways; keep her warm with blankets.
- Secure an intravenous (IV) line and begin fluid infusion with Normal Saline or Ringer’s Lactate solution. (You learned how to do this in Study Session 22 of the Antenatal Care Module and your practical skills training.) You may be trained to add a further dose of oxytocin to the fluids in the IV bag, but this is only possible if you can keep the drug refrigerated until needed.
- Keep the area of the vulva and perineum clean.
- Arrange to accompany the mother to the hospital if at all possible.
- Also ask family members or friends to go with the mother and look after the baby (and to be possible blood donors).
6.3.2 Retained placenta
Retained placenta is when the placenta remains in the uterus beyond 30 minutes after the birth of the baby. If this happens:
- Do not attempt further controlled cord traction to separate the placenta.
- Follow the instructions for pre-referral treatment as given above for PPH and get the woman to a health facility for emergency care as quickly as possible.
Summary of Study Session 6
In Study Session 6 you have learned that:
- Active management of third stage of labour (AMTSL) is the best intervention to reduce the risk of PPH by more than 60%. Therefore, AMTSL has to be applied routinely (to all delivering mothers).
- The sequential physiological changes in the third stage of labour are: separation of the placenta, descent of the placenta, expulsion of the placenta and control of bleeding.
- Common complications that can occur during third stage of labour include retained placenta, postpartum haemorrhage and uterine inversion.
- The components of AMTSL in sequential order are checking for a second baby, administration of uterotonic drugs, controlled cord traction, uterine massage after delivery of the placenta, placental examination for completeness, and examining the genital area for lacerations and active bleeding.
- Oxytocin, ergometrine and misoprostol are commonly used uterotonic drugs. Because ergometrine is a very strong drug, it is not recommended for use in Ethiopia’s rural Health Extension Service. Oxytocin and ergometrine must always be kept in a refrigerator until needed; misoprostol comes in tablet form.
- Administer misoprostol or oxytocin within one minute of the delivery of the baby.
- A well-contracted uterus is felt as firm to hard, well delineated and with no active vaginal bleeding, unless the source of bleeding is due to tear or lacerations of the lower genital area.
- Missed placental lobe, retained placenta, relaxed enlarged soft uterus, bleeding continuing despite the repeat administration of uterotonic drugs and uterine massage are all indications for setting up an intravenous line for pre-referral IV fluid infusion and immediate referral to a health facility.
Self-Assessment Questions (SAQs) for Study Session 6
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering the following questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 6.1 (tests Learning Outcomes 6.1 and 6.2)
- a.How do you define the third stage of labour?
- b.What physiological changes happen during the third stage of a normal uncomplicated labour?
Answer
- a.The third stage of labour begins with the birth of the baby and ends with the delivery of the placenta and its attached membranes.
- b.The physiological changes are:
- As the placenta separates from the wall of uterus blood from the vessels in the placenta bed begin to clot between the placenta wall and the myometrium (the muscular wall of the uterus).
- The placenta moves down the birth canal and through the dilated cervix before being expelled.
- Once expelled, the muscles of the uterus contract and compress the torn blood vessels so that any postpartum bleeding is stopped, and the uterus becomes hard and round.
SAQ 6.2 (tests Learning Outcomes 6.1 and 6.3)
Alemitu is a Health Extension Practitioner (HEP) in a village Health Post. She has just delivered a baby at her Health Post and the mother is in the third stage of labour, and has begun breastfeeding. Alemitu has been trained to use AMTSL. What, in detail, are the six steps that she must follow in order to do this?
Answer
Six steps to follow:
1 Check: is there a second baby?
2 Give a uterotonic drug to help the uterus contract:
- Misoprostol 600 μg (micrograms) tablets given orally with water, or
- Oxytocin 10 IU injected intramuscularly.
- Do NOT give ergometrine.
3 Deliver the placenta by controlled cord traction with counter-pressure (see Box 6.3 for details of how to do this).
4 Massage the uterus.
5 Examine the placenta and fetal membranes to check nothing is missing (i.e. check the maternal surface and the lobules, put your hand inside the membranes to make sure they are complete, and check that the position of the cord is normal).
6 Examine the women’s vagina and external genitalia for signs of tears and active bleeding.
SAQ 6.3 (tests Learning Outcome 6.3)
Imagine that you have managed the third stage of labour for a woman in your community by correctly using AMTSL, but she has developed continuous bleeding.
- a.Do you provide additional misoprostol? If yes, what dose should you give her and in what form?
- b.What else could you do?
- c.What should you do if the woman continues to bleed?
Answer
- a.Yes, so long as you do not exceed 1,000 μg of misoprostol in total, you can give up to a further 400 μg if you have already given 600 μg. You should give the second dose by inserting the tablets into the rectum.
- b.As the mother has already begun breastfeeding, rub the uterus using the two-handed pressure method to stimulate contractions.
- c.If the bleeding does not stop quickly after the second dose of misoprostol, you need to refer the woman to the nearest health facility as quickly as possible, starting her on IV fluids before you go.
SAQ 6.4 (tests Learning Outcome 6.6)
What are the warning signs for the complications that may arise during the third stage of labour?
Answer
Warning signs of potential complications during the third stage of labour are:
- A retained placenta or a placenta that has only been partially expelled
- A cervix which has closed before the delivery of the placenta
- Weak uterine contractions
- A soft uterus felt on palpation
- Third stage of labour lasting over 30 minutes
- Perineal, vaginal or cervical tearing
- Excessive bleeding (postpartum haemorrhage).