

1.4.2 ADHD and the environment
Because ADHD appears early on in life, there has been particular interest in prenatal environmental risk factors (Sciberras et al., 2017). Numerous things have been proposed as prenatal risk factors, but they do not all carry the same level of risk. They can be compared by examining their relative risk.
Absolute and relative risk
The absolute risk of a condition or disease occurring in an individual is the probability of developing the disease over a particular time period. It can be expressed either as a fraction (e.g. 3 in 100), or as a decimal number (0.03) or as a percentage (3%). Everyone has some level of absolute risk of developing a condition, but the absolute risk will be greater for some people than for others, depending on the presence of various risk factors.
When it comes to working out the effects of risk factors, investigators often use relative risk, which compares the absolute risk of people who have been exposed to a risk factor with the absolute risk of people who have not been exposed to the risk factor. For example, suppose the absolute risk of developing ADHD for a child whose mother smoked during pregnancy is 7 in 100, or 7%, and the absolute risk of developing ADHD for a child whose mother had not smoked is 3 in 100, or 3%. The relative risk of developing ADHD that is attributable to smoking during pregnancy can be calculated by dividing the smoker’s child’s risk (7%) by the non-smoker’s child’s risk (3%), which is 2.3. This means that children of mothers who smoke when pregnant are over twice as likely to develop ADHD as children of mothers who do not smoke when pregnant.
-
If the absolute risk of developing ADHD for a child born at full term is 3% and the absolute risk for a child born prematurely is 7.92%, what is the relative risk of premature birth?
-
The relative risk can be calculated by dividing 7.92 by 3 to give 2.64. This value means that a baby born prematurely is almost three times more likely to develop ADHD than a baby born at full term.
Various studies examining the relative risk of prenatal risk factors were reviewed and summarised by Sciberras et al. (2017). Those factors with more consistent findings in the research literature are shown in Figure 5.
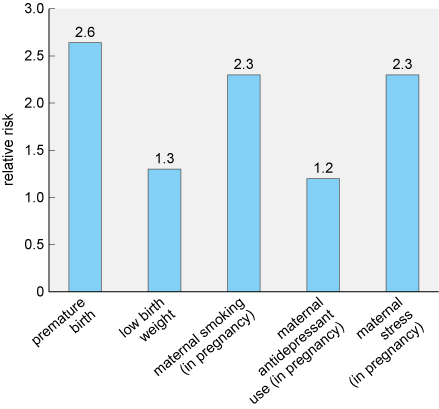
The risk factor conferring the greatest risk in Figure 5 is premature birth. Research has shown that this risk appears to increase with the degree of prematurity. For example, if a baby is born at less than 29 weeks the relative risk can increase to 5, meaning they are five times more likely to develop ADHD than babies born at full term.
-
Which of the factors shown confers the lowest relative risk?
-
The lowest risk is from maternal antidepressant use, which has a relative risk of 1.2.
When reviewing Figure 5, you may have recognised that some of the risk factors may be linked. For example, a premature baby is more likely to weigh less than a full-term baby. However, the researchers were able to take this into account in their analysis and so the figures reflect the risk conferred by each risk factor independently.
It is important to note that none of the risk factors discussed so far have a clear causal connection to ADHD. They are associated with increased risk of developing the condition, but exactly why this happens is unknown. Additionally, not all cases of ADHD can be explained by these accepted risk factors.
The fact that not all cases of ADHD can be explained by the risk factors which, based on research evidence, are generally accepted by the scientific and medical communities means that the search for other risk factors continues. For example, you may have read about concerns that exposure to screen technologies could increase the likelihood of developing ADHD. However, at present, evidence to support screen technology use as a risk factor for ADHD is lacking.
The studies that do exist at the time of writing (2019-2020) include relatively small sample sizes and are correlational studies, which means that they cannot demonstrate causality. An example of one such study conducted with children found that time spent watching television and playing video games was associated with attentional problems, with the video games being more problematic than television (Swing et al., 2010). However, this study relied on self-reported measures of time spent engaging in the activities, which can be unreliable, and only measured ‘attention’, and not ADHD symptoms specifically.
A much larger study by Montagni et al. (2016), conducted with adults without a diagnosis of ADHD, collected self-reported measures of attention and hyperactivity using a standardised scale, the Attention Deficit Hyperactivity Disorder Self-Report Scale (ASRS). They then related this to a self-reported measure of screen time covering the use of smartphones, televisions, computers and tablets. This study found a significant positive association between screen time and attention problems and hyperactivity levels. Compared to the lowest screen time category (never using screens), those in the highest exposure category (more than 8 hours per day) had a relative risk of 1.57.
-
Can you identify any limitations of the study in terms of what it can tell us about ADHD from the information provided?
-
You could have come up with several different limitations here. For example:
- The study was conducted with adults without ADHD and it is quite possible that the data may not generalise to adults with ADHD, or to children with or without the condition.
- The use of self-reporting can be unreliable for various reasons, including people simply misremembering information.
- The study found only an association, and so it is very important to be aware that this does not prove causality. It is possible that the direction of the relationship is actually the reverse, for example, those who struggle with attention may be more inclined to use screens.
As you have seen in this section, there are several possible genetic and environmental risk factors for ADHD. It is important to note that these risk factors can interact with each other and may confer a greater risk in combination.