

2.2 Alcohol use disorder (AUD)
AUD is the term now used for the conditions formerly referred to as alcohol abuse and alcohol dependence. AUD is the diagnosis given to someone who is showing signs and symptoms of addiction to alcohol. This is often referred to as ‘alcoholism’ and the individual concerned may be called an ‘alcoholic’. Someone with AUD would show several characteristics common to all addictive behaviours, but there are three key features:
- Tolerance – this refers to increasing engagement with the object of addiction (in this case, the ‘object of addiction’ is alcohol) in order to keep achieving the same effects. For example, an individual who might have been drinking half a bottle of spirits per day in the past may gradually escalate their drinking to consuming a whole bottle of spirits per day.
- Withdrawal – this refers to the signs and symptoms that occur when an individual refrains from addictive behaviour. The withdrawal signs and symptoms of alcohol addiction can include irritability, insomnia, shaking, and changes in heart rate and body temperature.
- Craving – this refers to the persistent nagging desire to engage in the addictive behaviour.
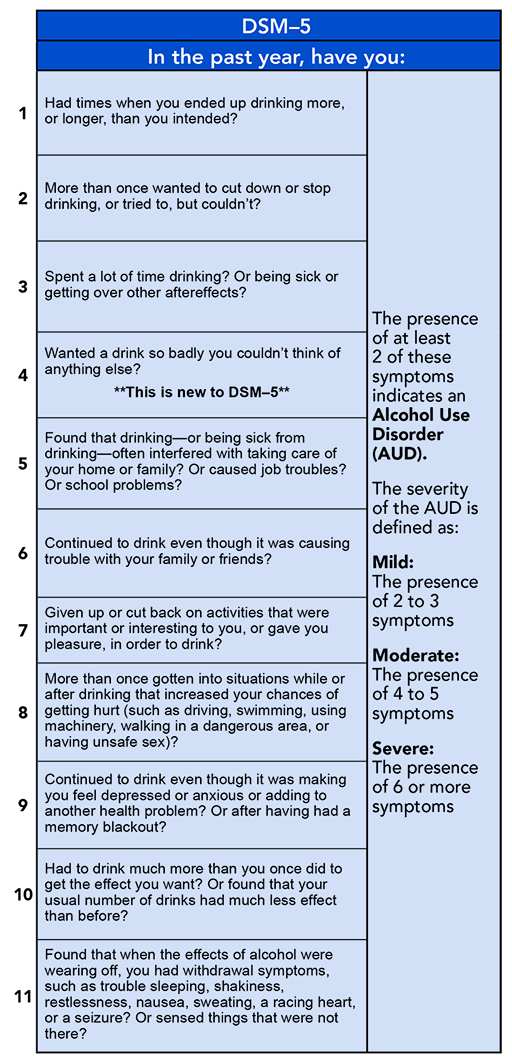
Psychologists use a series of criteria to diagnose AUD on the basis of psychological and behavioural effects. The list of considerations is seen here in Figure 7 (taken from the Diagnosis and Statistical Manual from the American Psychiatric Association [Tip: hold Ctrl and click a link to open it in a new tab. (Hide tip)] ).
It is important for diagnostic criteria to be reliable because so much depends on the process. For example, for anyone attempting to understand the nature of a condition, the prevalence or incidence rates would be misleading if diagnosis of that condition were not reliable. For anyone who might receive treatment for a condition, the implications of unreliable diagnosis might be more extreme. They may be prescribed the wrong treatment, or a treatment, such as a drug, that they do not need and which may cause other problems. Diagnosis is therefore vital, but experts do not always get the criteria right and the criteria themselves constantly evolve. It is important to be aware of this issue.
AUD can be explained through several physiological and psychological conditions.
Firstly, ethanol affects many brain regions by altering the activity of neurons. This is the underlying reason for some of the acute effects of alcohol such as reduced coordination and reduced self-restraint which you discovered in Week 5. However, as you learned in Week 5, alcohol is also able to stimulate the brain’s reward system releasing dopamine – the brain’s ‘happy’ and ‘rewarding’ messenger molecule. With frequent consumption of something rewarding like alcohol, dopamine release can start to occur earlier, so is released at the point of anticipation that something rewarding is about to happen (i.e. before the alcohol is actually consumed). Over time therefore dopamine starts to act as more of a wanting signal. In psychology this is known as classical conditioning, but you may already be familiar with this concept due to the experiment carried out by the Russian scientist Pavlov in the 1890s.