Session 1: Introducing human infectious diseases
Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Thursday, 30 April 2026, 4:54 PM
Session 1: Introducing human infectious diseases
Introduction
Most people on Earth experience at least one episode of an infectious disease every year. Although the majority recover, hundreds of millions suffer severe or long-term health effects as a direct result of an infection and around 10 million people – many of them children – lose their lives. In the 1960s, it was widely believed that the threat to health from infectious diseases would be overcome by advances in methods of prevention and treatment. Unfortunately these predictions have proved to be optimistic because of the rapidly increasing threat from ‘emerging infectious diseases’.
This first session of the course presents an overview of infectious diseases and discusses emerging infectious diseases.
In the following video, Dr Claire Rostron, Senior Lecturer in Health Sciences at The Open University, and one of the course authors, will introduce some exciting concepts to be covered in the course.

Transcript
CLAIRE ROSTRON: Infectious diseases are diseases that can be passed between people and sometimes between people and animals by infectious agents known as pathogens. An example could be influenza, commonly known as the flu, or meningitis or smallpox. In contrast, there are other diseases known as non-communicable diseases, such as arthritis or asthma, that cannot be transmitted between people and between people and animals. There isn't a risk of catching arthritis just by being next to someone who already has arthritis.
Sometimes it's obvious that there is a risk of infection. For example, in places where there is a lack of clean water and sanitation. Pathogens don't have to be transmitted directly from one person to another or from an animal to a person.
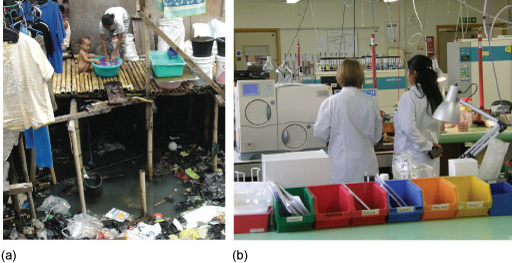
Often, however, the risk of infection is less obvious. This hospital laboratory tests for the presence of pathogens and may appear to be perfectly clean. But the lab coats which are being worn for protection are also potential carriers of infectious agents. Any non-living object in the environment that could transmit an infectious agent is known as a fomite.
The possibility of pathogens being transmitted via this route is why hospital doctors in the UK now rarely wear neckties that could drape across a person during a medical examination. In fact, it would be good laboratory practise for the individuals in this image to routinely wear and change gloves and to routinely clean and change their protective clothing.
In this Open Learn course, you will learn about some of the different routes of transmission as well as some examples of the pathogens that are transmitted via these different routes. But now, let's make a start by looking at some of the categories of infectious diseases, as well as how we go about diagnosing them.
Before you start, The Open University would really appreciate a few minutes of your time to tell us about yourself and your expectations of the course. Your input will help to further improve the online learning experience. If you’d like to help, and if you haven't done so already, please fill in this optional survey.
1.1 What are infectious diseases?
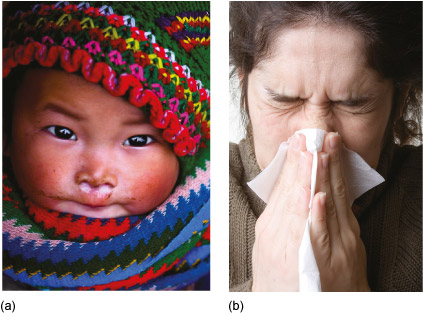
Infectious diseases are distinguished from other illnesses and disorders because they can be transmitted from someone who is ill either directly or indirectly to other individuals, who then develop the same infectious disease and are also able to pass it on. A familiar example is the ‘common cold’ which almost everyone has experienced at some time in their lives (Figure 1). Non-human animals and plants also suffer from infectious diseases, which cause massive losses to food crops and livestock, but our focus in this course is on infection in humans.
By contrast, health problems that cannot be transmitted between individuals, such as heart disease, diabetes, lung cancer, arthritis and depression, are known as non-communicable diseases (or NCDs). However, a few NCDs also have an infectious component, for example:
- in most cases of cervical cancer there is evidence of infection with a specific virus (the human papilloma virus, or HPV)
- hepatitis viruses cause liver disease and cancer of the liver
- a bacterium (Helicobacter pylori) causes stomach ulcers.
These examples illustrate the point that there is some overlap between some infectious and non-communicable diseases. The biology of bacteria and viruses is the subject of Session 3 Pathogens and infectious diseases.
For completeness, we should mention here that the third major category of diseases, disorders and disabilities is termed injuries, i.e. physical damage to the body caused by accidents or violence.
1.2 Symptoms and signs of infection
Symptoms are sensations in the body that only the person who is unwell can experience; for example, a headache, pain in the abdomen, blurred vision and nausea are all symptoms, because no one but the sufferer can experience them. Lay people, including children, can usually describe their symptoms accurately or report them if asked the right questions, but symptoms are subjective experiences that others cannot observe or verify.
By contrast, the signs of a disease are indicators of illness that other people can observe (e.g. a runny nose and frequent sneezing). Considering the symptoms and signs together may give enough information for a trained health worker to make a diagnosis, i.e. identify the underlying cause of the illness and give it a definite name. An example will illustrate this point.
You probably agree that the children in Figure 2 look ill, but how did you decide this?
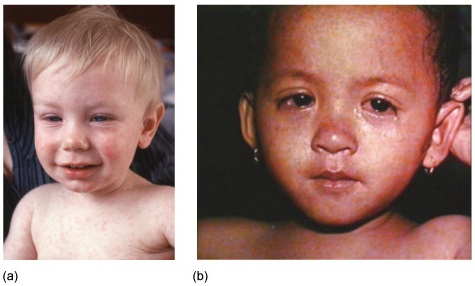
What signs of disease can you identify from their photographs? Did the name of any infectious diseases spring to mind when you looked at these children?
We expect that you noted the numerous tiny red spots on the children’s faces and shoulders and that their eyes look sore. Some of you (especially if you have children or much younger siblings) may have wondered if the cause could be roseola, or perhaps chickenpox or measles?
A trained health worker would first note the rash and sore eyes and ask the caregivers about other observable signs of disease, for example ‘Does the child have a cough or a fever?’ However, these signs alone are not enough to make a diagnosis. In this example, the health worker would look for clusters of tiny white spots inside the mouth (so-called Koplik spots), which are not always present, but if visible are a definite sign of measles. Combining all the information leads to the diagnosis that the children in Figure 2 do in fact have measles – an infectious disease caused by a virus.
However, it should not be assumed that only trained health workers can diagnose an illness. Most adults and parents at some stage make a ‘good enough’ diagnosis of what ails them or their children. Lay people very often decide on the basis of their own symptoms or the signs of disease they observe in family members whether to treat an illness at home with simple remedies, or seek advice from a trained health worker.
1.3 Acute or chronic conditions
Two useful terms that are equally relevant to infectious and non-communicable diseases (NCDs) refer to the time course of the illness. Knowing how long the symptoms of a disease have persisted and how quickly they are worsening or improving can help in making a diagnosis.
An acute condition is characterised by symptoms that develop rapidly and reach their peak within a few days or weeks. The patient either recovers relatively quickly or dies! Note that acute means ‘fast’ and ‘short-term’ – it does not necessarily mean ‘serious’. Some acute infections are mild and resolve in a short time without any treatment.
Can you identify an acute infectious disease that you or someone you know has suffered from in the past year, resulting in complete recovery within a week or two?
You may have suggested the common cold, or perhaps a stomach upset with an episode of diarrhoea. There are other possible examples.
By contrast, a chronic condition develops slowly and may take many months or years to reach its most severe extent. The term ‘chronic’ comes from Cronos, the Greek god of time. People with a chronic condition may cope well with its effects, but they may not fully recover the health they previously enjoyed. If left untreated, chronic diseases usually progress (get worse) and some conditions may result in permanent disability or loss of life. Tuberculosis (TB) is an example of a chronic infectious disease caused by bacteria that most often affect the lungs, but can also invade other parts of the body. TB progresses slowly but inevitably unless specific drugs are taken consistently every day for three-to-six months (Figure 3).

Most NCDs are chronic conditions, but some can have an acute episode – for example, people with cardiovascular disease (a chronic disease of the heart or blood vessels) can have a heart attack (an acute event).
1.4 What causes infectious diseases?
Infectious diseases are transmitted between individuals by infectious agents, known as pathogens [path-oh-jens], from the Greek word pathos (to suffer) and genès (to produce). Pathogens produce a lot of human suffering and disability across the world, including in relatively wealthy nations like the United Kingdom (UK). Most people have heard of at least some types of pathogen, for example bacteria or viruses.
The wider causes of infectious diseases range from insanitary living conditions in impoverished communities, to inadequate hygiene in the high-tech environments of modern hospitals (Figure 4). The impact of infectious diseases is therefore unequally distributed around the world, not only between countries, but also between individuals and groups within the same population.
Human biology is another factor to consider in explaining the cause of infectious diseases. Infancy and old age, inadequate nourishment, other illnesses and some types of medication can all create conditions in the body in which infection is more easily established.
In addition, there are individual human behaviours, habits and traditional practices that contribute to the causes of infectious diseases by spreading pathogens from one person to another.
Can you suggest any behaviours that can cause pathogens to spread?
There are many possible answers, but we thought of:
- not washing hands after using the toilet or before preparing food
- not covering the nose and mouth when sneezing or coughing
- spitting in the street
- leaving food uncovered where flies can settle on it
- not cooking raw meat thoroughly or inadequate reheating of cooked food.
These behaviours give some clues about the routes by which pathogens can be transmitted, as the next section describes.
1.5 Direct person-to-person transmission of pathogens
A new infection begins when pathogens leave the body of their host – the infected individual in which the pathogens are multiplying – and enter a new host. They may be repelled by defence mechanisms in the new host as discussed in Secion 4 ‘Immune defences against infectious diseases’, or they may survive and reproduce in sufficient numbers to cause an infectious disease.
Transmission of pathogens can occur directly between people, or indirectly in the air, water or food, or via other animals to humans, or from sources in the environment. In this section we explore direct transmission.
Figure 5 represents the three ways in which pathogens can be transmitted by direct person-to-person contact.
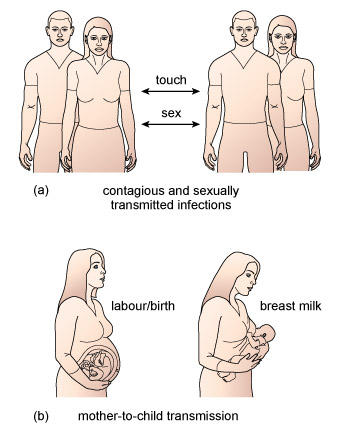
They are:
- Contagious infection, when touch, such as a handshake, transfers pathogens to a susceptible person; they may enter the new host through a cut or graze, or be transferred from hand to mouth.
- Sexually transmitted infection (or STI) involving infected semen, vaginal secretions, saliva or blood transmitting pathogens to the infected individual’s partner during unprotected sex. This is the most common route for the worldwide spread of HIV (the human immunodeficiency virus), which causes AIDS (acquired immune deficiency syndrome). Sexual transmission is more likely if the partner’s genitals, mouth or rectum are inflamed, for example, by another STI such as gonorrhoea [gonn-or-ree-ah] or syphilis [siff-ill-iss].
- Mother-to-child transmission, when pathogens pass from mother to baby during labour and delivery, or via breast milk.
1.6 Indirect person-to-person transmission of pathogens
Indirect person-to-person transmission occurs when the original host sheds pathogens into the air, water, food or objects in the environment, which then infect someone else (Figure 6).
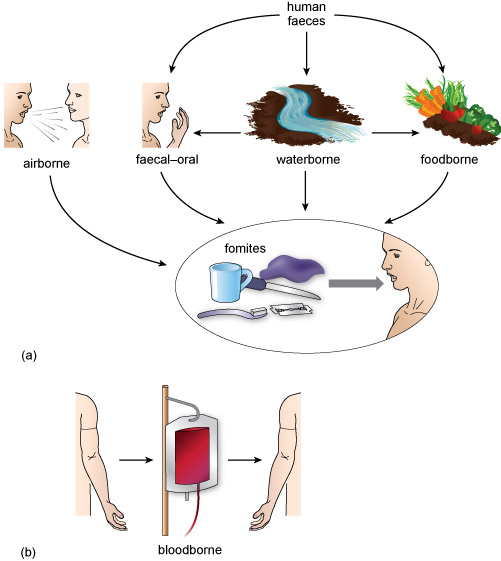
Most airborne infections are transmitted when a cough or sneeze expels fine droplets of water (known as an aerosol) containing millions of bacteria or viruses (Figure 7). The aerosol droplets may be inhaled by a susceptible person, or settle on surfaces where the pathogens contaminate hands, utensils, clothing, water or food, which are then touched or consumed by someone else.

Waterborne infections are particularly common in parts of the world where large numbers of people don’t have access to clean drinking water or safe disposal of sewage. Infected urine and faeces from humans and animals can wash into lakes and streams, where the pathogens multiply and reinfect people when they drink or bathe in contaminated water. Some pathogens (including the bacteria that cause cholera [koll-err-ah], a serious diarrhoeal disease) live naturally in environmental water sources, so they will always pose a threat to health.
Faecal–oral infections (‘faecal’ [fee-kal] and ‘faeces’ [fee-seez] refer to solid waste, or excrement) occur when pathogens from faeces enter the mouth (‘oral’ [orr-ahl]) and multiply in the gut. Transmission occurs when unclean hands, dirty cooking utensils or food contaminated by faeces enters the mouth. Flies can transfer pathogens from faeces to food via their feet. Contact with faeces is unavoidable when people are forced to defecate in the open because there is no sanitation. In these cases, people can get contaminated soil on their hands and the pathogens are easily transmitted from hand to mouth if there is no clean water or soap for handwashing.
Diarrhoeal diseases are often transmitted via the faecal–oral route, and some (e.g. cholera) are mainly waterborne. But they may also be due to foodborne infections caused by pathogens that originated in food components, for example, pathogenic bacteria in raw meat, eggs and on salad leaves.
Non-living objects in the environment, such as cups, spoons and door handles that people routinely touch, can also transmit infection and are known collectively as fomites [foh-mytz]. Clothing can also act as a fomite, which is why hospital doctors in the UK now rarely wear neckties that could drape across a patient during a medical examination and pick up infection that the next patient might acquire (Figure 8).

Can you identify the fomites in Figure 8 that could undermine infection prevention and control in this hospital?
In addition to the neckties worn by the two male doctors, all three doctors have stethoscopes, long-sleeved clothing, staff badges worn at waist height where they could brush against a patient, and the nurse is wearing a wristwatch. (If you go into a hospital in the UK nowadays, all staff must have their arms bare below the elbows, and wristwatches, rings and neckties are banned. Stethoscopes still touch a lot of patients on ward rounds and can’t be sterilised.)
Medical procedures can also transmit bloodborne infections; for example, before the transmission of HIV was understood, thousands of infections occurred from HIV-contaminated blood transfusions. Bloodborne pathogens can also spread via shared needles and syringes among people who inject illegal drugs, such as heroin.
1.7 Animal-to-human transmission of pathogens
Pathogens are often transmitted from animals to humans ‘accidentally’, for example via infected meat or water contaminated with animal faeces. But there are two transmission routes in which the animal is an essential agent in the transfer of pathogens to humans.
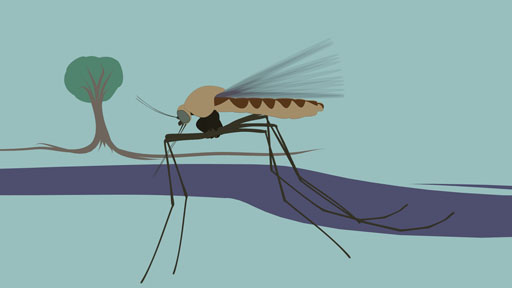
You can learn more about these in the following animation which focuses on malaria. Note that for simplicity in this animation we have referred to the pathogen that causes malaria as the ‘malaria pathogen’ or ‘malaria parasite’ but it should be remembered that the name ‘malaria’ refers to the disease and not the pathogen. The correct name for the parasite pathogen is Plasmodium and it has several different species including Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale and Plasmodium malariae.
Transcript
INSTRUCTOR: Zoonoses refers to diseases that are spread from animals to humans. It's possible for humans to catch diseases from a range of invertebrate and vertebrate animals. The term vertebrate refers to animals that have a backbone, like cows, pigs, bats, and birds. The term invertebrate refers to animals that do not have a backbone, like ticks, mosquitoes, and sand flies.
It's also possible for humans to transmit diseases to animals. And in this context, the zoonosis is termed a reverse zoonosis.
The risk of infection with zoonoses increases as the human population continues to grow and people live in greater proximity to animals. While the term zoonoses applies to all diseases that are spread from animals to humans, the term vector borne diseases applies only to those spread by an intermediate carrier.
An example of an intermediate carrier is a mosquito. An example of a vector borne disease is malaria. The mosquito bites an infected animal, such as a cow shown here, and becomes a carrier of the malaria pathogen. At this point, the mosquito is referred to as a vector.
When a mosquito bites, it releases a chemical into the circulation to stop the blood clotting. During this process, it could also release one or more of the malaria parasites it has been carrying into the circulatory system of the human it has bitten. If it does this, the person becomes infected. Once in the circulation of the infected human, the malaria parasite travels to the liver and multiplies. After multiplying, the malaria circulates again in the blood.
It is possible to take action to prevent infection with the malaria parasite. For example, you can use insect repellent and you can use insect nets while sleeping. You can also avoid travelling to countries where malaria is a known risk. These are simple prevention methods that avoid contact with the vector.
[MUSIC PLAYING]
An example zoonosis that may be familiar is influenza originating in pigs (swine flu) or poultry (bird flu). The influenza viruses that cause these diseases can sometimes be transmitted from animals to humans during the slaughter or handling of livestock. Some zoonotic [zoo-not-tik] influenza viruses pose a much greater health risk than the airborne seasonal influenza viruses that commonly circulate in human populations every winter.
Can you think of any other zoonoses that have made news headlines, at least in the UK?
You may recall that cattle can be infected with the bacteria that cause tuberculosis (TB), which can then be transmitted to humans. Badgers can also host TB bacteria, although there are no known cases of badger-to-human transmission. The mosquito borne Zika virus has also made news headlines because of its increasing incidence and the effects that have been observed on babies whose mothers have been infected. This virus may have originally been transmitted to the human population from monkeys.
A zoonosis that is well known in India and some other parts of the world is rabies [ray-beez]. The rabies virus can infect many warm-blooded vertebrates including squirrels, raccoons and bats, but the main route of transmission to humans is via dogs. Every year, over 3000 people in India die from rabies transmitted by a dog bite (Figure 9). The majority of these deaths are among children because they are more likely to try to play with unfamiliar dogs (Chatterjee, 2009).

Another route of transmission from animals to humans results in vector-borne infections. They differ from zoonoses in that they are transmitted by an invertebrate animal (without a backbone), mainly biting insects and ticks. The term ‘vector’ [vek-torr] comes from the Latin word for ‘carrier’, so in this context it means a carrier of an infectious disease. The pathogen must complete part of its life cycle in the vector, so transmission to humans may be prevented if the vectors can be killed. For example, Lyme disease is caused by a bacteria transmitted from birds or small mammals (such as deer) to humans by a type of tick.
Can you suggest why aeroplane cabins are sprayed with insecticide before take-off from a country where malaria is common?
The spray is to kill any mosquitoes that may have got onto the plane in the clothing or luggage of passengers. Mosquitoes are the vectors of malaria and transmit the pathogen when they bite humans to take a blood meal.
There are many other vector-borne infections, including bubonic plague [byoo-bon-nik playgg] transmitted by rat fleas, typhus [ty-fuss] transmitted by ticks, and yellow fever transmitted by mosquitoes. In 2014, the World Health Organization (WHO, pronounced ‘double-you-haitch-oh’ rather than ‘who’) – the branch of the United Nations responsible for coordinating and directing international policy and actions on health – devoted its annual ‘World Health Day’ to publicise the risk from vector-borne infections (Figure 10).

1.8 The end of infectious diseases?
In 1967, William H. Stewart (1921–2008), the Surgeon General of the United States of America (USA) – a role equivalent to the Chief Medical Officer in the UK – is alleged to have announced:
It is time to close the book on infectious diseases and declare the war against pestilence won.
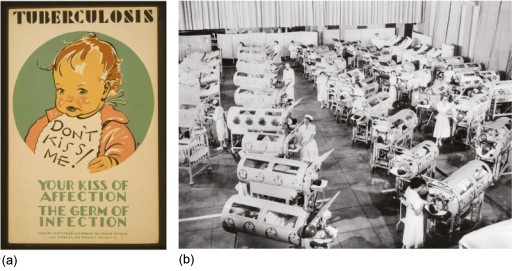
Less than 40 years before this woefully optimistic claim, at least 20 million people had died in 1918–19 from influenza, most of them young adults in the UK, USA and Europe. Public health officials in the USA in the 1940s were actively campaigning to halt the spread of tuberculosis (TB) in ways that may surprise you (Figure 11a), and in the decade ending in 1960 more than 102 000 people in the USA – many of them children (Figure 11b) – were paralysed by polio (data from Post-Polio Health International, n.d.; note that ‘n.d.’ indicates that no date was given).
So what gave public health officials like Stewart such confidence that the threat from infectious diseases was really over in 1967? The belief that infection had been vanquished in the USA and would ultimately be conquered in the rest of the world was based on the success of two innovations in medical science in the early 20th century:
- The development of new and more powerful antibiotics – a type of drug that kills bacteria, which dramatically cut the death rates in the 1950s and 1960s from bacterial infections such as pneumonia.
- Mass vaccination programmes after World War 2, where new vaccines containing substances derived from pathogens were given to children in injections or by mouth. In the 1950s and early 1960s, new vaccines gave effective protection for the first time against polio, diphtheria [dipp-thear-ree-ah], whooping cough (pertussis [purr-tuss-is]) and tetanus [tett-ann-us].
Unfortunately, Stewart was fundamentally wrong in predicting that infectious diseases would disappear as a cause of human suffering. They are still very much with us in the 21st century. New infectious diseases are emerging at an accelerating rate and pathogenic bacteria are developing resistance to antibiotics, so in some ways the threat is increasing, not decreasing as the next section briefly explains.
1.9 Emerging infectious diseases
Emerging infectious diseases (EIDs) is the collective term for a group of conditions that pose new threats to human health. EIDs can be distinguished into three types:
New infectious diseases caused by previously unknown pathogens:
Many of the diseases in this category are caused by zoonotic viruses, i.e. the viruses originated in other vertebrate animals, but at some point in the past they changed in ways that made them infectious to people. The best known ‘new’ infectious disease is AIDS but the virus that causes AIDS (HIV) may have originated in monkeys. Since HIV was identified in 1984, several other new infectious diseases caused by potentially fatal viruses have been identified. They include SARS (Severe Acute Respiratory Syndrome, Figure 12), which may have originated in poultry, MERS (Middle East Respiratory Syndrome), which may have originated in camels, and zoonotic strains of influenza (swine flu and bird flu).
 Figure 12 Doctors in Toronto struggled to contain SARS in 2002; the highly infectious virus was spread to Canada by a passenger on a flight from Hong Kong.
Figure 12 Doctors in Toronto struggled to contain SARS in 2002; the highly infectious virus was spread to Canada by a passenger on a flight from Hong Kong.Infectious diseases that have spread far outside their original range:
One example is Ebola virus disease (EVD), a ‘haemorrhagic’ [hemm-orr-adj-ik] fever, which means it causes severe internal bleeding, among other symptoms. Cases have occurred from time to time in remote villages in West Africa, but the first urban cases were detected in the capital of Guinea in February 2014 and from there Ebola quickly spread to neighbouring Liberia and Sierra Leone. A few travellers or health workers caring for Ebola patients developed the disease in other countries, including Nigeria, Mali, Senegal and the USA. By October 2015, over 11 000 deaths had occurred from over 28 000 suspected, probable and confirmed cases (Centers for Disease Control and Prevention, 2015). Many of these cases have not been confirmed in a laboratory, so the ‘case fatality rate’ (the proportion of confirmed infected people who die) is unknown; however, it is likely to fall within the range of 30 to 60 per cent.
Previously declining infectious diseases that have resurged:
Tuberculosis and some other infections caused by bacteria are a growing health concern because the causative pathogens are becoming increasingly resistant to antibiotics, which previously treated them successfully. So-called ‘hospital super-bugs’ are bacteria that have developed resistance to antibiotics in health care facilities, where antibiotics are heavily prescribed. An additional factor in countries where HIV/AIDS is common is that infection with HIV suppresses the body’s immune defences, so people with AIDS are more susceptible to other infections, including TB.
Session 1 quiz
This quiz allows you to test and apply your knowledge of the material in Session 1.
Open the quiz in a new window or tab then come back here when you're done.
Summary to Session 1
In this first session of the course you have learned about infections, which along with non-communicable diseases and injuries, are one of the three types of diseases, disorders and disabilities suffered by humans. You have learned that infections are diagnosed by health workers on the basis of signs and symptoms. Signs are consequences of the infection that are readily observable by other people, like raised temperature; symptoms are consequences of infection that can only be reported by the patient, like a headache.
You have also been introduced to pathogens. Pathogens are the biological agents that cause infectious disease and can be passed between people directly or indirectly, and can also come from animals and the environment. Importantly, however, you should now be aware that pathogens are everywhere, although if sensible measures are taken their transmission can be minimised and the incidence of the diseases they cause can be reduced considerably. Indeed, as we have outlined, the success of some early prevention strategies led scientists in the 1960s to predict that all infectious diseases would soon be defeated. As you are aware, this prophecy has not come true.
The shortage of clean water, sanitation and adequate health care in some parts of the world, the continual emergence of new infectious diseases and the capacity of some pathogens to adapt and become resistant to disease prevention measures, means the study of infectious disease is as critical to human health as it has ever been.
You can now go to Session 2.
References
Acknowledgements
This course was written by Basiro Davey, Carol Midgley, Claire Rostron and Daniel Berwick.
Except for third party materials and otherwise stated in the acknowledgements section, this content is made available under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 Licence.
The material acknowledged below is Proprietary and used under licence (not subject to Creative Commons Licence). Grateful acknowledgement is made to the following sources for permission to reproduce material in this unit:
Course image: James Gathany/Center for Disease Control and Prevention
Figure 1a: Bùi Linh Ngân. This file is licensed under the Creative Commons Attribution-Share Alike Licence http://creativecommons.org/licenses/by-sa/2.0/
Figure 1b: © iStock.com/nazira_g
Figure 2a: Anthea Sieveking/Wellcome Images
Figure 2b: CDC/Barbara Rice
Figure 3: WHO/TBP/Gary Hampton
Figure 4a: Marshall, J. (2005) ‘Megacity, mega mess’, Nature, vol. 437, Nature Publishing Group
Figure 7: James Gathany/Center for Disease Control and Prevention
Figure 9: Image taken from ‘Clinical Signs’, Virology Department, University of Saskatchewan
Figure 10: © World Health Organization (WHO), 2014. All Rights Reserved
Figure 11a: Work Projects Administration Poster Collection, Library of Congress
Figure 11b: © Everett Collection Historical/Alamy
Figure 12: BBC News Magazine
Every effort has been made to contact copyright owners. If any have been inadvertently overlooked, the publishers will be pleased to make the necessary arrangements at the first opportunity.