University of Dundee
| Site: | OpenLearn Create |
| Course: | Developing a Sense of Belonging in online distance learning |
| Book: | University of Dundee |
| Printed by: | Guest user |
| Date: | Thursday, 9 July 2026, 6:18 PM |
Description
Masters in Medical Education
This case study is from a completely online postgraduate programme for healthcare professionals who may be based anywhere in the world. Key to creating a sense of belonging on this programme has been creating clear student cohorts so that students move through a module together, and the use of small group exercises to allow the sharing of personal experiences and stories that are key to establishing a relationship of trust between students and staff.
Contributor: Dr Susie Schofield
1. About this programme
|
This is a postgraduate programme aimed at Health professionals, usually working full-time as clinical educators. Most students are studying part time. The cohort is approximately 70% UK-based students with others accessing the programme from overseas. We currently have a small cohort of on-campus (all international) and 1000 off-campus students (UK and overseas) The programme has three exit points – Certificate (three 20 credit modules), Diploma (Cert plus three more 20 credit modules), Masters (Diploma plus 60 credit dissertation), and students can work through all three consecutively, or graduate at e.g. Certificate or Diploma then return some time later to the next stage. Each stage is designed to be completed in one year, but students have up to two years for each, allowing them to take planned breaks between modules. There are core modules at each stage: Certificate (L &T, Principles of Assessment), Diploma (Leadership or Curriculum Planning plus Medical Education Research if student intends to progress to Masters level). In addition to the core modules there is a menu of optional modules, including specialties (e.g. surgical education) for specialty Certificate pathways. There is an overall module plan which is followed by all 20-credit modules, including the layout of the modules to help orientation. |
2. Design and delivery
|
The programme, originally a correspondence course, went online in 2010. Initially the online programme was highly flexible, allowing students to start at any point in the year, and with no fixed deadlines for assessments as a result. In 2016, this was changed to allow three entry points per year (January, May, September). This has made it possible to divide students into cohorts, and to enable them to work together and provide peer support. The programme is delivered using the School Virtual Learning Environment (VLE), Moodle which is supported by a dedicated learning technology team. Each 20 credit module within the programme takes 12 weeks to complete with an online task to be completed each week (e.g. set reading, watching videos). This is accompanied by a structured online discussion related to the material (not just “what do you think?”). Core modules will have larger student numbers than optional modules, and so within these students are split into groups of 20 for these, and online activities are undertaken with these smaller groups, rather than the larger module cohort. This is necessary in order to keep discussion forums both manageable, but also personal; many modules cover sensitive topics (e.g. end of life care) and so small group discussion forums allow the sharing of personal experiences. Every module has formative assignments. For each module, one is tutor marked, the others using peer feedback (tasks include things like sharing lesson plans and research ideas), self-evaluation or computer-marked. Not all students take up formative assessment opportunities but there is value in both giving and receiving peer feedback for those that do. Within each module there is also an assessment forum where students can ask questions about the assessment. A lot of peer support is offered here. All summative assignments, and some formative assignments, are submitted via Turnitin. There are opportunities for on-campus students to attend (face-to-face) ‘master classes’, but the vast majority will never visit Dundee. Master classes are occasional and sporadic, and set up to respond to student demand. |
3. Induction and orientation
Each student completes an online induction prior to the
start of their first module. This is provided in Moodle and is a self-study
resource including online activities and information which students work
through at their own pace. A video welcome from the programme leader is
included and students create a post in the discussion forum in response to some
prompt questions (see figure 1 below). A member of staff takes the time to
reply to every post, but often the students reply to each other.
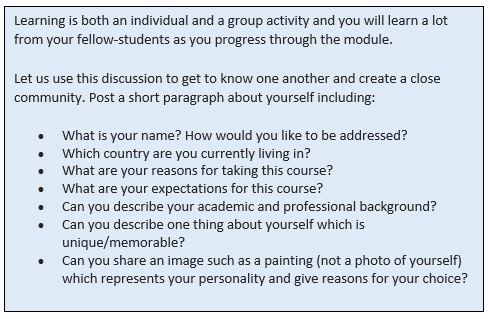
Figure 1: Discussion board induction task
After initial induction, a Moodle space (‘The Hub’) is available for all students on the programme and is used for longitudinal information e.g. selecting module options, changes to programme, additional support around academic and digital generic skills.4. Sense of belonging
|
The change to the programme in 2016 restricting students to one of three entry points was motivated in part to increase the sense of belonging for both students and our part-time tutors who are also off-campus. Students have a strong sense of belonging to the health professions, so this helps the sense of comradeship on the course. However, they are also developing a sense of belonging to the educational field. Online discussions are key to creating a sense of belonging, and finding the right size of group for creating fruitful discussion has taken trial and error. There are many international students on the programme and we had initially struggled with making the content relevant to everyone, but actually students share practice from their own settings and this can lead to rich discussion (e.g. differences in copyright law). This links the students up even though they are a disparate group. Students are not, however, forced to participate in online discussions, and some never do. If a student has not engaged in the VLE for three weeks then they are sent a supportive email just to check that they are not struggling. We are currently reviewing whether we should do this also with those who don’t engage in the discussion boards. A dialogic approach is taken to assessment and feedback in that students are expected to reflect on feedback from their assessment, and respond to the marker with any comments, and plans for development. We plan to extend this use of feedback dialogue from tutor-student to student-student. The dialogic approach is further supported by the use of Turnitin which is open to students, and which they are encouraged to use as a self-development tool. Most modules have one tutor-marked formative assessment, but other assessments are computer-, peer- and self-assessed. Synchronous activities (e.g. collaborative classroom) have not been successful due to difficulties in finding appropriate times for students to come together online: the working patterns of medical professionals and differences in timezones make it virtually impossible! However, alternative asynchronous activities have proved to be just as engaging. For example, after unsuccessful attempts to run synchronous question and answer sessions with expert speakers, Padlet was used so students were able to pose questions to the speaker. The module lead themed the questions to guide a recorded interview with the expert. This was then posted to the VLE. |
5. Student experience
Students feel much more part of a group since the change from non-cohort to cohorted. This has also had a huge impact on success, progression, completion and retention rates. Student feedback (see below) is largely positive in terms of the benefits of collaborative activities, although comments highlight how different students have different needs, with some receiving adequate peer support in their professional context, and so requiring less from peers on the programme.
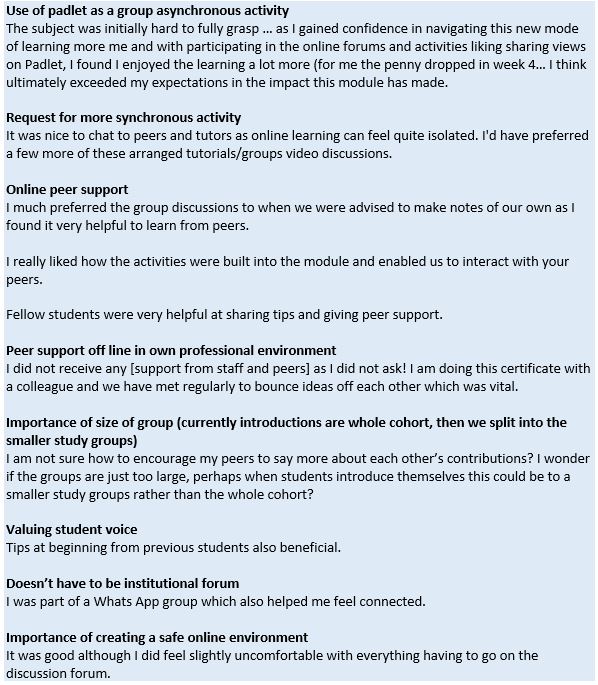
Figure 2: Student feedback from end of module surveys
6. Recommendations
- The move to cohorts was essential in developing a sense of belonging. Prior to this, it was very difficult to organise collaboration between students.
- The perennial challenge is that of including synchronous activities. On reflection this just may not work for the kinds of students on this programme (shift work, different timezones). The students don’t turn up, even when multiple times are offered, so they are perhaps voting with their feet and telling us that they are just unable to engage with this kind of educational experience.
- Finding the right number for group work took some trial and error, and around 20 seems to be ideal, at least for first years; smaller numbers don’t work, as not all students engage all of the time. However, as students progress they become more confident and smaller groups may work at higher levels.
- We would like to introduce more longitudinal elements as a next step to developing the programme. Some students find it difficult to plan their modules, and their pathway through the programme, experiencing things ‘module by module’. Tasks like completing a teaching portfolio would encourage reflection over a longer period, or other forms of patchwork assessment in which smaller assessments are pieced together to form a coherent whole. This will encourage ownership over learning, and autonomy and hopefully shift student mindsets from “I belong to a module” to “I belong to a programme”.