Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Sunday, 21 June 2026, 3:40 AM
Communicable Diseases Module: 20. Introduction to HIV/AIDS
Study Session 20 Introduction to HIV/AIDS
Introduction
In Parts 1 and 2 of this Module, you learnt about the basic principles underlying the transmission, diagnosis, management and prevention of communicable diseases, and the application of this knowledge to vaccine-preventable diseases, malaria, tuberculosis and leprosy. In Part 3 of the Module, we focus on HIV and AIDS — a cause of increasing concern for the health of Ethiopians.
The human immunodeficiency virus (HIV) is a virus that infects humans and weakens the immune system. As a result, HIV-infected people are more prone to acquiring other infections and diseases that individuals who haven’t been infected with HIV are able to fight off easily. The collection of diseases that results from HIV infection is called Acquired Immunodeficiency Syndrome (AIDS). In this study session, we will first briefly describe the status of the HIV epidemic in Ethiopia, so you understand the magnitude of the problem and how it may affect your community. We will then describe some important functions of the immune system — the main target of HIV in the human body — so that you have a basic understanding of the biology of HIV infection, and how it eventually leads to AIDS. Finally, we will outline the different modes of HIV transmission between humans. This knowledge will help you in providing effective care and health education for your HIV-infected clients, and in the implementation of HIV prevention measures in your community. Care, health education and prevention in the context of HIV/AIDS will be discussed in greater detail in later study sessions.
Learning Outcomes for Study Session 20
When you have studied this session, you should be able to:
20.1 Define and use correctly all of the key words printed in bold. (SAQs 20.1 and 20.2)
20.2 Summarise the main features of the HIV epidemic in Ethiopia. (SAQ 20.1)
20.3 Describe the basic components and functions of the immune system, and explain what HIV is and how the immune system is affected by it. (SAQs 20.1, 20.2 and 20.3)
20.4 Describe the usual course of an HIV infection and how it progresses to AIDS in the absence of effective treatment. (SAQs 20.1, 20.2 and 20.3)
20.5 Describe the modes of transmission of HIV. (SAQ 20.1)
20.1 The HIV epidemic in Ethiopia
We begin this study session by describing the current extent of the HIV epidemic in Ethiopia. In order to do this, we first need to remind you of several terms that you learnt in earlier study sessions, which you will need to know again here as we describe the epidemiology of HIV/AIDS. Epidemiology is the statistical study of the occurrence, distribution, potential causes and control of diseases, disabilities or other health problems in human populations.
In relation to disease epidemiology, can you recall the difference between prevalence and incidence?
Prevalence and incidence were described in Study Session 2 of this Module. Prevalence refers to the total number of cases of a particular disease or health condition existing in a population at a certain point in time, or during a given period (e.g. a particular month or year). Incidence refers only to the numbers of new cases of a disease or condition that are identified in a given period.
In the context of HIV/AIDS, you will also come across the term people living with HIV (abbreviated to PLHIV) when describing epidemic statistics, and indeed when we talk about other aspects of this disease. PLHIV refers to everyone who is infected with the virus, whether or not they remain in good health or have developed any HIV-associated diseases, including AIDS.
In Ethiopia, there were an estimated 1.2 million PLHIV in 2010. Thus, the prevalence of HIV infection in Ethiopia in 2010 was estimated to be 2.4% of the general population (2.9% of all females and 1.9% of all males). The HIV epidemic in Ethiopia is generally levelling off (stabilising), with signs of decline in major cities, but a rising epidemic in small towns and market centres. Women and children are particularly affected by HIV/AIDS; in 2010, close to 60% of the PLHIV in the country were females (totalling around 700,000 women) and about 80,000 were children.
Another important factor for you to consider in terms of the impact of HIV/AIDS in your community is geographical distribution. There is a marked variation in HIV infection between regions in Ethiopia (Figure 20.1).

Compare the prevalence of HIV infection in Addis Ababa to that of other regions in Figure 20.1. Would you expect HIV infection to be more prevalent in urban or rural areas in Ethiopia?
The prevalence of HIV in Addis Ababa, an entirely urban population, is much higher (9.2%) than in other regions with a mixed urban and rural population. Therefore, HIV infection appears to be more prevalent in urban than in rural areas.
Indeed, the average prevalence of HIV infection across all urban areas in Ethiopia is 7.7%, whereas in rural areas it is 0.9%. Another epidemiological factor that you should consider in order to help target prevention programmes is the fact that the highest HIV prevalence occurs in the 15–24 years age group. Note that reproductive health issues related to this risk group are covered in the Module on Adolescent and Youth Reproductive Health.

In response to the HIV/AIDS epidemic, the government of Ethiopia launched a free HIV/AIDS therapy programme in January 2005. Currently, about 550 health facilities, most of which are health centres, provide HIV/AIDS therapy services in Ethiopia, and you should become aware of the nearest one to your health post. Similarly, you should know the location of the nearest centres providing HIV counselling and testing services (see Figure 20.2; there are more than 2,184 sites providing counselling and testing in Ethiopia), and/or providing services for pregnant mothers (about 1,352 health facilities are mainly focused on prevention of mother-to-child transmission of HIV).
20.2 HIV and the immune response to infection
In this section, you will first learn what HIV is and then about the basic functions of the immune system, which are gradually destroyed by HIV infection. This knowledge will help you to understand how HIV induces disease in infected people.
20.2.1 What is HIV?
HIV is a virus, and like all viruses it is not a true cell, but a microscopic particle much smaller than a bacterium. Viruses are essentially minute ‘boxes’ made of proteins containing the genetic material that carries the information needed to make more viruses of the same type. But viruses cannot reproduce themselves unless they invade a true cell and take control of the normal chemical processes taking place in the cell. The virus turns the cell into a virus ‘factory’, producing millions of new viruses and killing the host cell as it sheds its load of viruses into the body.
There are different types of viruses, and HIV belongs to a group called the retroviruses. This name is important because the drugs that have been developed in recent years to treat PLHIV are called antiretrovirals (or ARVs), and the combination of drugs and other treatments that an individual receives is called antiretroviral therapy (or ART). You will learn all about ARVs and ART in Study Sessions 22 and 23.
There are two species of HIV, known as HIV-1 and HIV-2. HIV-1 is the virus responsible for the majority of HIV infections in most countries, including Ethiopia. HIV-1 is more infectious and has a much greater ability to be transmitted between people than HIV-2. (HIV transmission will be discussed in more detail in Section 20.4.) HIV-2 infection is mainly prevalent in West African countries, and it is thought to induce progression to HIV-associated diseases and AIDS more slowly than HIV-1.
20.2.2 The human immune system
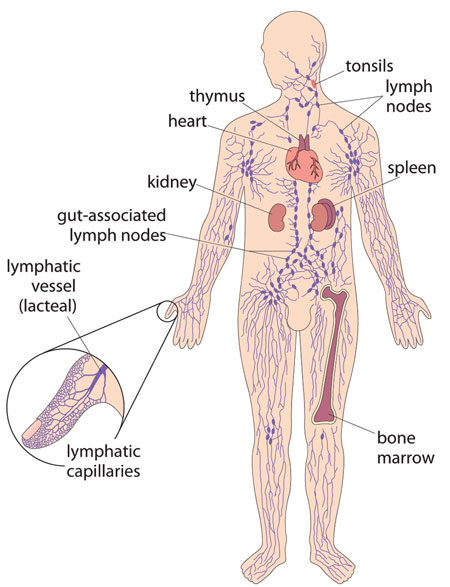
The immune system is a collection of cells, tissues and organs in the human body, with the combined function of protecting us against invasion by infectious agents (see Figure 20.3). In the absence of an effective immune system, our bodies would easily be invaded by pathogenic (disease-causing) viruses, bacteria, protozoa and parasites, which would rapidly cause our death. The exact functioning of the immune system is very complex, and explaining it in detail would go beyond the scope of this Module. Rather, we will focus here on a particular aspect of the immune system, so that you can understand what HIV does to the human body once it gets inside us.
Biologists and doctors use the term ‘leukocytes’ instead of white blood cells; we will use both terms in this study session. You will probably say ‘white blood cells’ when talking to your clients.
The immune system first recognises infectious agents as not being a normal part of the body, or, in other words, ‘foreign’ to the body. Then the cells of the immune system organise a concerted attack against the infectious agents in order to destroy them. These immune cells are most often known as white blood cells — although the name is misleading because they are found throughout the body’s tissues and organs, as well as in the blood, as Figure 20.3 shows. There are several different types of white blood cells, and we will say more about one of them shortly.
The immune response by a person’s white blood cells takes a few days to build up during the first time that a particular type of infectious agent gets into his or her body. During this delay, there is usually time for the infectious agents to multiply and cause symptoms of the illness. However, as the immune attack builds up, it may become strong enough to eliminate the infection, and the person recovers spontaneously from a so-called self-limiting infection. But in some types of infection, the immune response cannot protect the person sufficiently from the infectious agents, they become more and more ill, and without medical intervention they may eventually die. This is what happens in PLHIV unless they receive modern medical treatments.
One important feature of the immune system is that it very quickly recognises the same infectious agents if they have invaded that individual in the past. This is known as immunological memory. It enables the immune system to organise a stronger, faster and more efficient attack if it comes across the same infectious agent again in the future. You will see later that the immune system manages to keep HIV under control for months or years after it first invades the body, but eventually it becomes overwhelmed by the virus.
20.2.3 Lymphocytes and the immune response to infection
We will now describe how the immune system attacks a virus (such as HIV), but note that similar processes occur when bacteria and protozoa invade the human body. The most important group of white blood cells in our defence against infection are the lymphocytes, of which there are several types (Figure 20.4). Lymphocytes called B cells are responsible for producing special proteins called antibodies against the invading infectious agents. Antibodies are proteins that bind to viruses (and other infectious agents), attracting other types of lymphocyte (we have called them cytotoxic T cells in Figure 20.4) to come and destroy the invaders. Viruses can only multiply inside the body’s own cells, so destroying our own body cells if they have been infected by viruses is a price worth paying, because it slows down the production of more viruses.
Cytotoxic means ‘able to kill cells’.
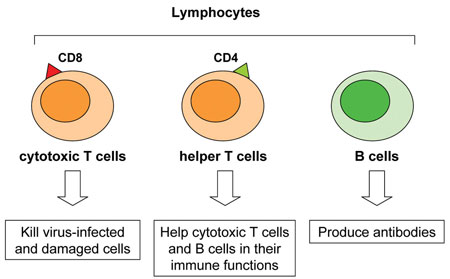
Most importantly, the helper T cells in Figure 20.4 ‘help’ all the other cells of the immune system to make antibodies and attack invading infectious agents. These cells are also known as CD4 lymphocytes (or CD4 cells) because they have a special protein on their surface called CD4. These are the terms we will use in this Module. Without a large number of CD4 lymphocytes circulating around the body acting as ‘helpers’, the functioning of the whole immune system collapses, and the person is defenceless against invasion by infectious agents.
20.2.4 Lymph nodes
If you look back at Figure 20.3, you can see that lymphocytes accumulate in sites located throughout the body, including the lymph nodes (or lymph glands). When an infection occurs, cells of the immune system, particularly lymphocytes, divide and produce more cells that help fight the infection. This process results in the lymph nodes becoming enlarged, as a result of the increased number of lymphocytes they contain. The lymph nodes in the neck can sometimes be seen as small swellings under the skin, or felt by touching with your fingers, if you have a bad cold or a throat infection. Enlarged lymph nodes may also be felt in the armpits and groin during some other infections. They return to their normal size once the infection has been eliminated.
20.3 How does HIV disable the immune system?
In this section, we explain how infection with HIV disables the human immune system. The key to this lies in the CD4 lymphocytes.
20.3.1 HIV infects the CD4 lymphocytes
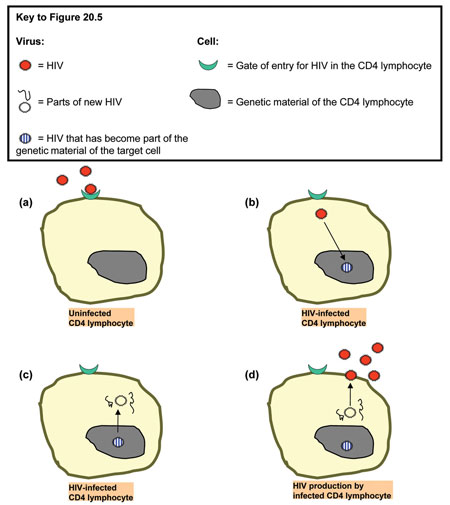
Like all viruses, HIV has to enter (i.e. infect) healthy cells in the body in order to produce more copies of itself. These newly-produced viruses are then released into the blood in order to infect other susceptible cells. You may think of an HIV-infected cell as a sort of HIV factory. However, not all cells in the human body can be infected by HIV. Its main targets are the CD4 lymphocytes. Figure 20.5 shows in more detail the mechanism of infection of a CD4 lymphocyte by HIV.
20.3.2 How does HIV damage our immune system?
In a newly HIV-infected person, the virus enters some of the CD4 lymphocytes, which produce many new copies of the virus and shed them into the body. The CD4 lymphocytes eventually die as they release their load of viruses. The new copies of HIV circulate in the body and attack other CD4 lymphocytes, which in turn produce more HIV and then die. This goes on and on — more and more CD4 lymphocytes are destroyed, as more and more HIV copies are made.
What effect will the destruction of many CD4 lymphocytes have on the immune system’s ability to protect the person from other infections?
The CD4 lymphocytes give essential help to the other types of lymphocytes that make antibodies, or kill virus-infected cells in the body; without this help, the rest of the immune system cannot function properly.
Over time, the number of CD4 lymphocytes declines to the extent that the immune system cannot protect the person from illnesses like chest infections and diarrhoeal diseases that it would normally fight off. We will return to this point shortly.
20.4 The progression from HIV infection to AIDS
Understanding the difference between HIV and AIDS, and the natural course of an HIV infection, is important when you teach community members about HIV transmission and prevention. It also explains why you need to refer PLHIV quickly if they develop new health problems, or their health deteriorates.
20.4.1 The natural course of HIV infection
As you learnt in Study Session 1 of this Module, an infected person may not show symptoms of the disease right away — it generally takes some time to develop a disease after an infection. Likewise, when we say someone is ‘infected with HIV’, we mean that the person has the virus in their blood, and this has been confirmed by doing a laboratory analysis for HIV, or a rapid diagnostic test (RDT) on their blood. Note that an HIV-infected person may not have any symptoms and may look healthy, but they can still transmit the virus to their sexual partner(s).
During the first years of infection, the immune system, although weakened by the loss of some of its CD4 lymphocytes, still functions quite well. The infected person will have no symptoms, or only minor symptoms — perhaps a little loss of weight, or inflammation of the sinuses in the head. Many HIV-infected people do not know that they have acquired the virus at this stage.
You will learn how to do the HIV rapid diagnostic test in Study Session 24 of this Module.
Over several years, the person’s immune system gradually becomes weaker, and they become vulnerable to persistent communicable diseases that they would previously have fought off before symptoms even developed, or would have quickly recovered from. These diseases are called opportunistic infections (OIs) because the infectious agents that cause them only have the ‘opportunity’ to multiply in the body because the PLHIV’s immune system has been so badly affected by HIV.
You will learn about opportunistic infections in detail in Study Session 21.
In adults, it usually takes around 5–10 years after HIV infection before the person becomes very sick, if he/she is not taking ART. The natural course of HIV infection is shorter in children and infants when compared to adults. In Section 31.1 you will learn why HIV-infected children progress faster to AIDS.
You will learn about prevention of mother-to-child transmission of HIV in Study Session 27, and about HIV in children in Study Session 28.
20.4.2 Clinical staging of HIV disease and AIDS
As time passes and the number of CD4 lymphocytes declines even further, to a very low level, the incidence of opportunistic infections and other health problems in PLHIV increase, and the person is said to have reached a particular stage of HIV disease. The final stage of this progressive deterioration is known as AIDS — Acquired Immunodeficiency Syndrome — based on diagnostic criteria developed by the World Health Organization (WHO).
WHO HIV clinical staging is described in Study Session 21.
20.5 Modes of transmission of HIV
Now you know what HIV does once it has infected someone. But how is HIV transmitted from person to person? Getting infected with HIV does not happen as easily as, for instance, infection by the viruses that cause measles or influenza, which are transmitted in airborne droplets, typically during normal social contact with an infected person.
HIV needs ‘transport’ to get into the body of another person. This ‘transport’ can be blood, semen (the male sexual secretion containing sperm), vaginal fluid, or breastmilk.
Suggest some ways in which these transport media could be transferred from one person to another.
HIV can be transmitted through sexual intercourse with an infected person; through transfusion of contaminated blood, or blood products, in medical treatment; through sharing of needles, syringes and cutting or perforating objects contaminated by HIV-infected blood or body fluids; through the blood of an infected mother passing into the baby during pregnancy or delivery; and finally through the breastmilk of an infected mother being fed to the baby.
We will look briefly at each of these routes in turn, but you will discover more details in later study sessions.
20.5.1 Transmission through sexual relations
Unsafe sex (sexual intercourse without a condom) is responsible for the majority of HIV infections worldwide. HIV is primarily considered as a sexually-transmitted infection (STI), an infection that is transmitted through sexual intercourse. Different types of sexual practice have different degrees of risk for transmitting HIV, as described below.
Anal sex
Anal sex refers to the penetration by the male penis into the anus of another person. It represents the biggest risk of infection if one of the partners is HIV-infected, because the anal mucosa does not produce natural lubrication, is fragile, and wounds and bleeds very easily during anal sex. Also, the penis can have microlesions (tiny areas of damaged tissue that are too small to be visible with the eyes), which permit the entrance of the virus into the bloodstream. The soft tissue of the male foreskin in uncircumcised men is especially vulnerable to infection during both anal and vaginal (see below) sex.
Mucosa (also known as mucous membrane) is a very thin layer of moist tissue that lines some organs and body cavities, including the mouth, anus and the reproductive tract.
Vaginal sex

Vaginal sex involves penetration of the female vagina by the male penis, and is the most common type of sexual practice. HIV can be found in large quantities in the semen of infected men, and to a lesser amount in the vaginal secretions of infected women. The risk of infection is still high in vaginal sex, but less than with anal sex, because the vagina produces natural lubrication and is more elastic. However, unprotected vaginal sex represents a serious risk of HIV infection, because the vaginal mucosa (as well as the penis) can have microlesions which permit entry of the virus into the body. Figure 20.6 is a poster which was designed to raise awareness about the dangers of unprotected vaginal sex, and to inform people about ways to reduce the risk of HIV infection
Oral sex
The term oral sex means there is contact between the genitals and the mouth. Compared to anal and vaginal sex, oral sex represents the smallest risk for HIV transmission. However, very small wounds in the mouth can allow entry of the virus into the body.
Other STIs increase HIV transmission risk
Note that in all types of sexual practice, the presence of other STIs causing damage to the genitals (discharge or ulcers) increases the risk of acquiring and transmitting HIV. This is because, in people with an STI, transmission of HIV is easier due to the presence of lesions in the genital mucosa.
You will learn about other STIs in Study Session 31.
20.5.2 Transmission through blood contact
The blood is another way of transmitting HIV. HIV can be transmitted through transfusion of an infected blood or blood products; sharing contaminated needles and syringes to inject illegal drugs; accidental puncturing of the skin by contaminated instruments during healthcare; and sharing contaminated piercing or cutting instruments used in tattooing or harmful traditional practices, like uvulectomy (cutting out the uvula in the roof of the throat) and female genital mutilation (cutting the clitoris and labia).
20.5.3 Transmission from mother to child
HIV can be transmitted from an infected mother to her child through the placenta during pregnancy, or (more often) during labour and delivery. Also, breastfeeding can transmit the virus from mother to child because the breastmilk of an infected mother contains HIV, which can penetrate the mucosa lining the baby’s gastrointestinal tract.

20.5.4 Myths about HIV transmission
Knowing how HIV is not transmitted, and educating community members about the myths that some may believe (see Box 20.1 and Figure 20.7), helps to increase the inclusion of PLHIV in society, and reduce the stigmatisation and discrimination they often experience.
Box 20.1 Myths about HIV transmission
HIV is not transmitted by:
- tears, saliva, sweat or urine
- personal contacts — kisses on the mouth, hugging, handshakes
- social contact — at work, in school, in cafés and restaurants
- air or water — sneezing, coughing or swimming
- contact with common items — pens, toilets, towels, sheets, soap
- insects — mosquito bites or bites by other insects.
In Study Sessions 25–27, we demonstrate how understanding the modes of transmission of HIV is the basis for implementing prevention measures against HIV infection at the community level, and for healthcare providers, including yourself.
Summary of Study Session 20
In Study Session 20, you have learned that:
- At the time of writing, the HIV prevalence in Ethiopia is 2.4%, and an estimated 1.2 million people live with the virus; prevalence is much higher in urban than in rural areas, and more women than men are infected.
- HIV affects the immune system by destroying the CD4 lymphocytes, which ‘help’ all the other white blood cells to defend the body against infection.
- Infected CD4 lymphocytes produce many new copies of HIV and then die. The new viruses infect other CD4 lymphocytes, which make more new viruses and die, until so many CD4 lymphocytes are destroyed that the immune system weakens, and the PLHIV develop opportunistic infections.
- The first few years with an HIV infection are usually healthy, or with only mild symptoms; the person may not know they are infected and can transmit HIV to others.
- It may take 5–10 years following HIV infection to develop more serious opportunistic infections and progress to AIDS (in the absence of ART).
- HIV is transmitted by sexual intercourse, by contact with infected blood and from mother to child.
- The highest risk of sexual transmission is through unprotected anal sex, but the most common route is unprotected vaginal sex.
- There are many myths about HIV transmission; educate your community that it cannot be transmitted by normal personal and social contacts with PLHIV, or contact with air, water, common objects or biting insects.
Self-Assessment Questions (SAQs) for Study Session 20
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering the following questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 20.1 (tests Learning Outcomes 20.1, 20.2, 20.3, 20.4 and 20.5)
Which of the following statements is false? In each case, explain what is incorrect.
A HIV is more prevalent among young sexually active people than among elderly people.
B In Ethiopia, more females than males are infected with HIV.
C In most cases, an HIV infection can lead to AIDS in a few months.
D In the early course of HIV infection, people may not know that they are infected with the virus because they feel healthy (have no symptoms and signs).
E HIV mostly infects the red blood cells of humans.
F HIV can only be transmitted through sexual intercourse with an infected person.
G HIV is not transmitted through oral sex.
H Unprotected anal sex has a lower risk of transmission of HIV than unprotected vaginal sex.
I Eating and shaking hands with PLHIV cannot transmit HIV to uninfected individuals.
Answer
A is true. HIV is more prevalent among young sexually active people than among elderly people.
B is true. In Ethiopia, more females than males are infected with HIV.
C is false. In most cases, an HIV infection leads to AIDS in 5–10 years, and only if the person does not get antiretroviral therapy.
D is true. In the early course of HIV infection, people may not know that they are infected with the virus because they feel healthy (have no symptoms and signs).
E is false. HIV mostly infects CD4 lymphocytes, which are a type of white blood cell in humans.
F is false. HIV can be transmitted through sexual intercourse with an infected person, but also by transfusion of infected blood, or blood products sharing — or accidental puncture with — sharp objects contaminated by infected blood; and from mother to child.
G is false. HIV can be transmitted through oral sex; the virus can get in through microlesions in the mucosa lining in the mouth.
H is false. Unprotected anal sex has a higher risk of transmission of HIV than unprotected vaginal sex.
I is true. Eating and shaking hands with PLHIV cannot transmit HIV to uninfected individuals.
SAQ 20.2 (tests Learning Outcomes 20.1, 20.3 and 20.4)
The main targets of HIV infection are the CD4 lymphocytes.
- a.What is a CD4 lymphocyte and what is its role in the human body?
- b.How does HIV infection of the CD4 lymphocytes determine the natural course of HIV disease progression to AIDS?
- c.Is the progression from HIV infection to AIDS the same for every person living with HIV?
Answer
- a.A CD4 lymphocyte is a special type of white blood cell in the immune system, which circulates in the body and ‘helps’ other lymphocytes to function in the immune response, e.g. by making antibodies, or attracting killer cells to destroy virus-infected cells.
- b.HIV infection of the CD4 lymphocytes determines the natural course of HIV disease progression to AIDS, because the number of CD4 lymphocytes in the body gradually declines over time. They die when they shed millions of new viruses, made in every infected CD4 lymphocyte under instructions from the HIV that originally infected it. As the CD4 lymphocyte numbers fall, they can no longer ‘help’ the immune system to function effectively, and PLHIV begin to develop more and more infections and other health problems. These ultimately progress to the worst stage — AIDS — unless the person gets antiretroviral therapy.
- c.The progress of HIV infection is faster in children and infants when compared to adults.
SAQ 20.3 (tests Learning Outcomes 20.3 and 20.4)
Why are opportunistic infections given this name?
Answer
These diseases are called opportunistic infections because the infectious agents that cause them only have the ‘opportunity’ to multiply in the body because the CD4 lymphocytes are being destroyed by HIV. This leaves the immune system unable to protect the person from infection he or she would otherwise have been able to fight off.