Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Tuesday, 21 July 2026, 9:16 PM
Communicable Diseases Module: 27. Prevention of Mother-to-Child Transmission of HIV
Study Session 27 Prevention of Mother-to-Child Transmission of HIV
Introduction
As you will recall from Study Session 20, one of the routes of transmission of HIV is from mother to child. This occurs when an HIV-infected woman passes the virus to her baby during pregnancy, during labour and delivery, or during breastfeeding. In this study session, you will learn about prevention of mother-to-child transmission (PMTCT) of HIV.
Learning Outcomes for Study Session 27
When you have studied this session, you should be able to:
27.1 Define and use correctly all of the key words printed in bold. (SAQ 27.1)
27.2 Describe the routes and risks of HIV infection in the context of a mother and child. (SAQ 27.1)
27.3 Explain why it is important to offer counselling on HIV testing to all pregnant women, and describe the features of the ‘opt out’ approach to HIV testing. (SAQs 27.2 and 27.3)
27.4 Describe the drugs and regimens used for prevention of HIV transmission from mothers to children. (SAQ 27.4)
27.5 Explain counselling on breastfeeding options for preventing mother-to-child transmission. (SAQs 27.1 and 27.2)
27.1 Transmission of HIV from mother to child
We know that not every baby born to an HIV-positive mother will be infected by the virus. This is because the placental membrane between the fetus and the mother remains intact during pregnancy.
The placental membrane forms a barrier between the blood of the mother and the fetus, limiting the transmission of HIV.
However, if the HIV-infected mother has problems during pregnancy, such as a lack of antenatal care (ANC), infections or poor nutritional support, she may become sick, which will further weaken her immunity. As a consequence, the number of viruses circulating in her blood will rise, and this increases the likelihood of the virus crossing the placenta and infecting the unborn child.
HIV is mostly transmitted from mother to child during delivery, at a time when the cuts and abrasions that often occur during birth increase the risk of the baby coming in contact with his or her mother’s blood. Therefore, it is essential that an HIV-infected pregnant woman is supported by ANC services, and that she delivers her baby safely at a health facility, as illustrated in Figure 27.1. Importantly, if the baby is born in a setting where birth trauma is less likely to occur, the likelihood of transmission of HIV from mother to child is reduced.
It is part of your role as a Health Extension Practitioner to counsel and encourage a pregnant mother to come to you for antenatal care, and to give birth to her baby at a health facility.

After delivery, HIV may be transmitted from mother to child through breastfeeding (although the risk is not as high as that during delivery). During breastfeeding, the virus may pass through the gut wall of the baby, particularly if it is inflamed, due to infection, by bacteria causing diarrhoea.
PMTCT can reduce the chances of HIV from mother to child from 30% to 10%. This is a dramatic improvement, and HIV-positive mothers should be encouraged to seek PMTCT.
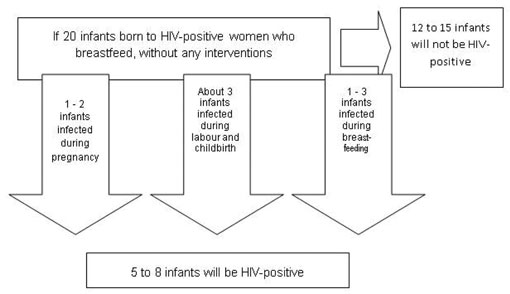
The risk of HIV transmission from mother to child for pregnant women who are not supported by ANC and PMTCT services is summarised in Figure 27.2. It has been estimated that 30 out of 100 babies (30%) born to mothers with HIV will be infected with the virus if the mothers do not attend ANC to receive PMTCT services. The outcome can be dramatically improved if the HIV-infected mother takes prophylactic drugs, which greatly reduce the chances of her baby becoming infected with HIV. The success of chemoprophylaxis depends on the drugs taken, and on good antenatal care follow-up to ensure adherence to treatment. In general, less than 10 out of 100 children will be infected by HIV if drugs for PMTCT are taken by the mother.
27.2 HIV testing and counselling for PMTCT
In this section you will learn about the advantages and challenges of testing and counselling HIV-infected pregnant mothers. For pregnant women, knowing their HIV status may help them to make informed decisions about their pregnancy, in particular if they are identified as being HIV positive. Your role in this process is to inform them about the advantages of receiving ANC, HIV testing and counselling services at the health post. HIV-infected pregnant mothers will then be able to decide whether to receive appropriate and timely interventions to reduce the risk of HIV transmission to their unborn baby. The interventions available to them are described in Box 27.1.
Box 27.1 Interventions for PMTCT available in Ethiopia
Antiretroviral treatment/prophylaxis
If a pregnant mother is HIV positive, the risk of HIV transmission to her baby can be greatly reduced by administering a single ARV drug, or a combination of several drugs (these were introduced in Study Session 22). For the purposes of PMTCT, ART is taken for a short period between the end of pregnancy and at early postpartum time. It is possible that the HIV-infected mother is also eligible to start antiretroviral treatment (this depends on her clinical stage; WHO HIV clinical staging was introduced in Study Session 21).
Breastfeeding
Another route by which HIV can be transmitted to the infant is through breastmilk. One of your duties is to provide counselling on safe infant feeding, and this will be discussed further in Section 27.6.
Family planning
Family planning counselling for mothers who are HIVpositive is another means of preventing the transmission of HIV to their children. This is done through preventing unwanted pregnancies. You will be expected to counsel and inform pregnant mothers about family planning in the context of HIV.
An additional advantage of PMTCT includes the fact that the mother will receive education on the importance of giving birth in a setting where standard precautions for infection prevention and safer obstetric practices are implemented. This ensures safe delivery for the mother and her child, not only in the context of HIV/AIDS, but also in case other complications arise during labour.
PMTCT counselling and HIV testing also contributes to the prevention of HIV transmission between adults, by spreading information about HIV/AIDS amongst the community. Mothers who are HIV positive and continue to receive follow-up and ongoing healthcare for themselves and their HIV-exposed infant usually transmit this information to relatives and/or friends. In order to help with dissemination of information on HIV prevention, you should encourage mothers to disclose their status to partners and family members. In addition, this helps them to get support from their family, and reduces stigma and discrimination from other members of their community.
A supportive partner and family will have a positive effect on how a pregnant mother engages with PMTCT; improving the life outcomes for both the mother and her child.
As a health worker, you may come across pregnant women who are reluctant to undergo HIV testing and counselling for PMTCT. Indeed, when confronted with a life-changing situation (such as knowing your HIV status), women may take into account many personal and community-related factors before making a decision on whether to take a test for HIV and counselling for PMTCT.
When you discuss these intervention measures with them, you should be aware of the most common challenges associated with HIV testing and counselling programmes for women in this situation. They may experience diagnosis-related stigmatisation, or discrimination from their family and community. They will be concerned about the reaction of their partner, and this is often the main obstacle to testing and counselling. HIV testing and counselling for couples encourages mutual support and reduces the stigma and discrimination that might result from being HIV positive. Indeed, the support of the male partner is essential for a pregnant woman who is about to take advantage of PMTCT, if the new situation is to be accepted by the family.
27.3 Approaches to HIV testing in antenatal care settings
Knowing the HIV status of a pregnant woman is the cornerstone of PMTCT. You will recall from Study Session 24 that those about to be tested for HIV need to be offered appropriate pre-test education and counselling and this particularly applies to pregnant women. There are two approaches to HIV testing. Both provide information to the client about HIV, and the risks and benefits of testing in a language that is easily understood. However, the two approaches differ in the process through which consent by the client is obtained. These are known as ‘opt-in’ and ‘opt-out’ approaches.
27.3.1 Opt-in approach to HIV testing
In this approach, you should provide information and individual counselling to the client about HIV/AIDS, about testing for HIV and about the consequences for their lives if they test positive. The pregnant woman is given the choice of either refusing or consenting to a HIV test. This option should be presented in a neutral, supportive manner. Women who ‘opt in’ explicitly request to be tested, and their informed consent is clearly established. The opt-in approach requires an active step by the individual woman to agree to be tested.
Remember, consent can be given either in writing or verbally. Women should not be coerced into giving consent.
27.3.2 Opt-out approach to HIV testing
This approach expects you to provide information on HIV/AIDS and HIV testing in the form of group education. The opt-out approach is offered as a routine part of standard care. In this case, pregnant women are informed and routinely offered HIV testing and counselling. They are then given the opportunity to decline the test should they choose to do so or, in other words, to ‘opt out’ of a HIV test. The opt-out approach emphasises that HIV testing is a routine component of ANC.
However, you should stress to pregnant women that HIV testing is still voluntary under the opt-out approach, and that they have a right to refuse testing. You should identify and resolve issues that prevent a pregnant woman from accepting HIV testing. The Ethiopian FMOH recommends the opt-out approach and therefore you are expected to offer HIV testing and counselling to all pregnant mothers coming to your health post, or that you encounter in your community during house-to-house visits.
A pregnant mother who is HIV positive and two months pregnant comes to you with signs and symptoms of WHO HIV stage 4 disease. What will you do?
As you have learnt previously, WHO HIV stage 4 patients need ART, and you have to refer them to the health centre for thorough care and ART.
27.3.3 Preferred ANC testing approach in Ethiopia
The ‘opt-out’ strategy is the recommended approach by the Ethiopian Federal Ministry of Health for HIV testing and counselling in the ANC setting. This helps normalise HIV testing, and makes the test a routine component of ANC. Importantly, this is also likely to increase the number of women who get tested for HIV.
Recall the ‘3 Cs’ introduced in Study Session 24. ‘consent, confidentiality and counselling’.
PMTCT programmes must adhere to the three guiding principles of testing and counselling. These are informed consent, confidentiality and the provision of post-test counselling and support services. Informed consent deals with asking mothers for their willingness to be tested. So you should obtain verbal or written consent after you counsel the mother about HIV testing. The mother has to make an informed decision. You also have to keep all information about the mother confidential. Information is only used to help the client to get the necessary health services, and the information has to be kept at the health facility. After counselling and testing for HIV, the provision of post-test counselling is essential for both HIV-negative and HIV-positive mothers. For services including PMTCT, you will be expected to refer the mother to the nearest health centre.
A mother comes to the health post a few days before her due date. She has never been tested for HIV. Do you think it is important to provide her with HIV testing and counselling?
Yes, it is essential that you offer her HIV testing and counselling, and refer her to the nearest health centre for further care.
HIV testing, and PMTCT services when appropriate, are offered at several time points during the healthcare provision and management of pregnant women. PMTCT is integrated into antenatal care, labour and delivery, postnatal care, family planning, and other settings where pregnant women and women of childbearing age receive healthcare services and education.
Therefore, you need to provide comprehensive information and counselling services for all pregnant women presenting to ANC and women of childbearing age at your health post. Mothers and potential mothers should receive information on the following issues:
- Pre-test counselling, HIV testing, post-test counselling and follow-up services that should be offered to the mother and her partner for PMTCT of HIV.
- Prevention of HIV in infants and young children, including interventions for PMTCT. Prevention of HIV in infants and young children includes the use of ARVs and safe breastfeeding practices.
- Safer sex practices that would promote the prevention of transmission of HIV infection.
27.4 Steps in the HIV testing process
The steps involved in HIV testing were fully explained in Study Session 24, and will only be touched upon briefly here. You will recall that the key steps are:
- Provide pre-test counselling and education.
- Obtain verbal or written consent.
- Obtain a blood test sample; at health-post level, you take a finger-prick blood sample or venous blood.
- Process the sample using the nationally recommended rapid HIV test procedures.
- Obtain and interpret results.
- Keep results and all information confidential.
- Provide results to the client.
- Provide post-test counselling, support, and referral.
As part of this process, as mentioned earlier, you will also need to provide essential information on PMTCT. You should also discuss safer sexual practices, the importance of disclosure of the test result, and partner testing.
27.5 ARV treatment options for PMTCT
27.5.1 General considerations
Though at this time you may not be allowed to prescribe drugs for PMTCT, it may soon be available for you to provide the service for HIV-positive pregnant mothers in your own community. The type of antiretroviral drug treatment offered will depend on the clinical stage of the mother. You will therefore have to differentiate between HIV-positive pregnant mothers who need ARV drugs for PMTCT, and those who need ARV drugs for treatment of their own condition. The main criteria for PMTCT in HIV-infected pregnant women who still do not need ART for themselves are outlined below. You should be aware though that all options of PMTCT using ARV drugs significantly reduce HIV transmission to the child.
Pregnant mothers should take ART if they fulfil the following criteria:
- If their CD4 count is available:
- WHO clinical stage 4: Regardless of the CD4 count, they have to receive ART for treatment.
- WHO stage 3: They need treatment with ART if their CD4 count is less than 350/mm3.
- WHO clinical stage 1 or 2: They need treatment with ART if their CD4 count is less than 200/mm3.
- If their CD4 count is not available:
- All women who are in WHO clinical stage 3 or 4 need ART.
- Women who are in WHO clinical stage 2 need ART if they do not have a CD4 count, but their total lymphocyte (white blood cells) count is less than 1200/mm3.
Remember that the CD4 count refers to the number of CD4 lymphocytes per cubic millimetre (mm3) of blood.
You should note that the above criteria are used to identify HIV-infected pregnant mothers who need ART treatment. If an HIV-positive pregnant mother is taking ART treatment, she doesn’t need to take any additional ARV drugs for PMTCT. HIV-positive pregnant mothers will be screened at health-centre and hospital level, and if they fulfil one of the above criteria they will be advised to start ART treatment. If they do not fulfil the criteria, they will be counselled for PMTCT using ARV drugs.
Therefore, if you find pregnant mothers who are HIV positive at your health post or in your community, refer them to have their CD4 count checked at the nearest health centre. If they are referred back to you from the health centre, you need to make a proper follow up of them in the community.
27.5.2 Single-dose Nevirapine, and other ARV options for PMTCT
The simplest drug regimen used to prevent HIV transmission is a single dose of Nevirapine given to the mother at the onset of labour, and a single dose given to the baby after delivery. It is estimated that this regimen reduces the rate of HIV transmission by half. As it is given only once to the mother and baby, it is relatively cheap and easy to administer. Consequently, it has been the mainstay of many PMTCT programmes in Ethiopia and other resource limited countries. You may be expected to use this simple intervention at your level for PMTCT.
Because of concerns about drug resistance, and that a single-dose regimen may not be as effective as combination drug therapies, there is now general agreement that single-dose Nevirapine should be used only when no alternative PMTCT drug regimen is available. Whenever possible, women should receive a combination of drugs to prevent HIV resistance problems, and to decrease mother-to-child transmission rates even further.
Nevirapine, however, is still the only single-dose drug available for PMTCT. Other treatments require women to take drugs during and after pregnancy, as well as during labour and delivery. This means they are much more expensive and more difficult to implement, unlike Nevirapine, which can be used with little or no medical supervision at all. For the moment, single-dose Nevirapine remains the only practical choice for PMTCT in areas with minimal medical resources.
In addition to single-dose Nevirapine, two other options are available, but these are beyond the scope of this study session (some of these drugs were introduced in Study Session 24):
- Combining AZT with single-dose Nevirapine and Lamivudine.
- Three full-dose combination of ARVs.
At this point it should be emphasised that short-term ARV prophylaxis for PMTCT does not treat maternal HIV immunosuppression, and therefore does not provide long-term benefits for the health of the mother. For this reason, women should be regularly assessed for ART eligibility. And if a pregnant mother is eligible to start ARV drugs, she should be referred to the nearest health facility to start the treatment.
Explain the difference between using ARV drugs for ART or PMTCT.
When ARVs are used for treatment purposes, usually patients take three or more combined drugs, and they are taken for life. In PMTCT, ARVs are taken as prophylaxis for a short duration, with the aim of preventing the transmission of the HIV from the mother to the child. In addition, in PMTCT a single drug, or a combination of drugs, can be taken.
27.6 Breastfeeding options for PMTCT
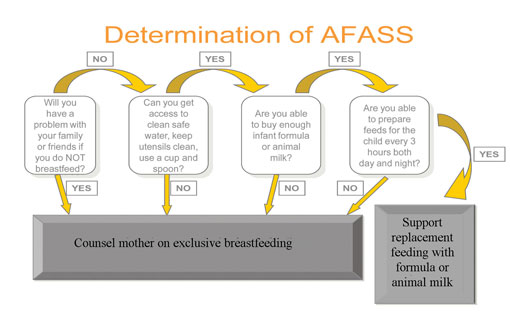
Exclusive breastfeeding is defined as feeding only breastmilk to the infant for the first six months of its life (the mother’s milk is the sole source of nourishment). Exclusive breastfeeding is NOT recommended for HIV-infected women. However, the alternatives, using formula or animal milk, are not always a viable option and in such cases breastfeeding should be used. Exclusive breastfeeding should be avoided if the following criteria, established by the WHO and called the AFASS criteria, can be met:
- Acceptable: replacement feeding for breast milk should be acceptable by the family and others who are close to the family.
- Feasible: the mother has access to clean and safe water for cleaning utensils such as feeding bottles and teats.
- Affordable: the family has to be able to buy formula milk or animal milk.
- Sustainable: the mother is able to prepare feeds for the child as frequently as recommended.
- Safe: the formula milk should be safe for the health of the infant.
Figure 27.3 illustrates the AFASS decision pathway used to determine how an HIV-infected mother should feed her baby.

When replacement feeding fulfils AFASS criteria, avoidance of all breastfeeding by HIV-infected women is recommended (Figure 27.4). At six months, if replacement feeding is still not acceptable, feasible, affordable, sustainable and safe, continuation of breastfeeding with additional complementary foods is recommended, while the mother and baby continue to be regularly assessed. All breastfeeding should stop once a nutritionally adequate and safe diet without breastmilk can be provided.
27.7 Four interventions for PMTCT in the community
In this section you will be introduced briefly to the four intervention strategies associated with PMTCT. In your work as a Health Extension Practitioner you have to keep in mind these interventions aim to increase the number of mothers willing to use PMTCT services.
Component 1: Prevention of new HIV infections in parents-to-be
This intervention targets young women and their partners, and promotes the use of condoms, and voluntary counselling and testing (VCT) before marriage, and during pregnancy. You should ensure that all women know that they have access to family planning and counselling, and you should encourage open discussions on reproductive health issues. This intervention also emphasises the early treatment of sexually transmitted infections (STIs), and encourages a sensible attitude towards sexual activity – strategies that will help prevent HIV transmission.
Component 2: Prevention of unwanted pregnancies in HIV-infected women
Here you should give information and counselling to HIV-infected women on family planning methods. You will also have to explain access to family planning counselling, and services that promote the correct and consistent use of condoms.
Contraceptive methods are fully explained in the Family Planning Module.
Component 3: PMTCT using ARV drugs
This intervention aims to encourage all HIV-positive women who are pregnant or who have recently delivered a baby and their newborns to receive ARV drugs in order to minimise the risk of HIV transmission during pregnancy, labour or during the postnatal period.
Component 4: Care and support of HIV-positive mothers and their families
This intervention seeks to provide clinical care and prophylaxis for opportunistic diseases that HIV-infected mothers (or their HIV-positive family members) may acquire. This strategy includes social, financial and psychological support for both HIV-infected pregnant women and their family members.
Summary of Study Session 27
In Study Session 27, you have learned that:
- PMTCT is one of the key strategies to prevent the transmission of HIV.
- PMTCT significantly reduces the risk if HIV transmission from mothers to their infants and helps establish a link to other HIV-related comprehensive services.
- Community mobilisation to increase attendance of pregnant women for antenatal care and institutional delivery increases the coverage of PMTCT services in Ethiopia.
- HIV testing and counselling services using the ‘opt out’ approach are provided routinely to pregnant mothers as an entry point for HIV care.
- There are three ARV options for PMTCT, but the most widely used at community level is the single-dose Nevirapine regimen.
- When the AFASS criteria for replacement feeding are not met, then exclusive breastfeeding is the nationally recommended strategy for HIV-positive mothers in Ethiopia. Ideally, HIV-positive mothers should not breastfeed their babies if a replacement feeding option is available.
- The interventions implemented by the FMOH for PTMCT target four components: prevention of new HIV infections, prevention of unwanted pregnancies in HIV-infected women, the use of different ARV drug regimens for PMTCT, and care and support services for HIV-positive mothers and their families.
Self-Assessment Questions (SAQs) for Study Session 27
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering the following questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 27.1 (tests Learning Outcomes 27.1, 27.2, 27.3 and 27.5)
Can a pregnant woman transmit HIV to her baby during pregnancy, delivery or breastfeeding? What should you recommend to her?
Answer
An HIV-infected pregnant woman can pass the virus on to her unborn baby, either before or during birth, so she should give birth in a health facility. HIV can also be passed on during breastfeeding. Exclusive breastfeeding is therefore not recommended but will be necessary if the AFASS criteria cannot be met. If a woman knows that she is infected with HIV, there are drugs she can take to greatly reduce the chances of her child becoming infected.
SAQ 27.2 (tests Learning Outcome 27.3)
Can women with HIV have normal healthy babies? What are the most important ways of reducing the risk of mother-to-child transmission of HIV?
Answer
Women who are infected with HIV are able to have normal and healthy pregnancies if they use ANC services and PMTCT to improve the chances of having an HIV-negative baby.
- It is important that HIV-infected pregnant women attend antenatal care to decrease the risk of transmitting the virus to their infants during pregnancy.
- Because of the risk of HIV transmission from mother to baby during labour and delivery, HIV-infected mothers should plan to deliver their baby in a healthcare facility, where there are safer delivery practices.
- It is also critical that the baby and mother continue to receive ongoing care in the post-delivery period to reduce the likelihood of transmission through breastfeeding, and to monitor the infant’s health, growth and development.
SAQ 27.3 (tests Learning Outcome 27.3)
Why should a pregnant mother be tested for HIV? Explain the advantages of HIV testing and counselling for PMTCT.
Answer
There are a number of reasons why a pregnant woman should be tested for HIV:
- Knowing her HIV status can help her make informed decisions about her current and future pregnancies.
- If she is infected, knowing her status can help her to access other HIV care and treatment services.
- If she is infected, she can learn how to prevent HIV transmission to her baby.
- If she is infected, she can learn how to reduce the risk of infecting other people.
- If she is not infected, it will help her to stay uninfected, and keep her family safe from HIV infection.
- Whether she is infected or not, testing can help to plan for the future.
SAQ 27.4 (tests Learning Outcome 27.4)
Which of the following statements is false? In each case, explain what is incorrect.
A Less than 10 out of 100 children will be infected by HIV if drugs for PMTCT are taken by the mother.
B All pregnant women who are HIV-positive and in WHO clinical stage 3 or 4 need antiretroviral therapy (ART).
C A pregnant woman who is taking ARV drugs to treat her own HIV infection also has to take additional ARV drugs for PMTCT.
D PMTCT with single-dose Nevirapine means giving one dose of this drug to the newborn baby.
Answer
A and B are true.
C is false. A pregnant woman who is taking ARV drugs to treat her own HIV infection does not need additional ARV drugs for PMTCT.
D is false. Single-dose Nevirapine for PMTCT is given to the mother at the onset of labour, as well as to the newborn baby.