Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Monday, 29 June 2026, 4:01 AM
Family Planning Module: 9. Permanent Family Planning Methods or Voluntary Surgical Contraception (VSC)
Study Session 9 Permanent Family Planning Methods or Voluntary Surgical Contraception (VSC)
Introduction
Sterilisation is the most effective, and one of the most widely used contraceptive methods available worldwide. It is often the best contraceptive choice when desired family size has been achieved. Both tubal ligation in women, and vasectomy in men, are one-time procedures that are safe, inexpensive and relatively straightforward to do for a trained person. Sterilisation does not require constant use of a contraceptive method, regular visits to health facilities or repeated expenditure on contraceptive supplies. Although sterilisation procedures usually demand a greater investment in skill, training and equipment than temporary methods of contraception, they provide lifelong protection against pregnancy, and are therefore more cost-effective. Since voluntary surgical contraception (VSC) procedures are almost always irreversible, clients require effective counselling before making any decision.
In this study session, you will learn about the definitions, mechanism of action of VSC, techniques of sterilisation, and the advantages and disadvantages of female and male sterilisation.
Learning Outcomes for Study Session 9
When you have studied this session, you should be able to:
9.1 Define and use correctly all of the key words printed in bold. (SAQ 9.7)
9.2 Describe how to counsel on VSC methods. (SAQs 9.1, 9.6 and 9.7)
9.3 Explain the mechanism of action of VSC methods. (SAQs 9.2, 9.3, 9.4 9.5 and 9.7)
9.4 List and discuss the types of VSC methods. (SAQs 9.4 and 9.5)
9.5 Describe the techniques of sterilisation. (SAQ 9.7)
9.6 Explain the advantages and disadvantages of sterilisation for both sexes. (SAQs 9.5 and 9.7)
9.1 Mechanism of action
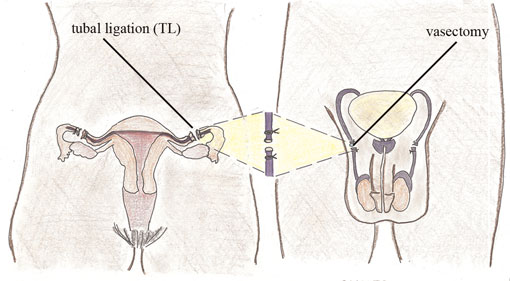
Voluntary surgical contraception (VSC) is a permanent family planning method, which involves female sterilisation or male sterilisation. In women, the process is called fallopian tube ligation or tubal ligation, and involves mechanically blocking the fallopian tubes by cutting them to prevent the sperm from reaching the egg. In men, vasectomy involves blocking the vasa deferentia, or sperm ducts, to prevent the passage of sperm into the semen, so that fertilisation and pregnancy during sexual intercourse cannot occur. You will see diagrams illustrating these procedures later in this study session.
9.2 Counselling for sterilisation
Sterilisation is a permanent method of contraception. Once the surgery has been performed, the individual cannot simply change his or her mind. A number of circumstances, usually hard to predict, may lead users to regret that the sterilisation procedure was performed, for example losing their children, getting divorced or remarried, or wishing for additional children.
Make certain that your client(s) correctly understand the procedure and its consequences. You must tell the client that VSC is irreversible. Once the client has undergone VSC it is extremely difficult for him/her to reverse the procedure and have more children. You can use the ‘BRAIDED’ concept for successful counselling, which you covered in Study Session 3.
The main questions you should ask during a VSC counselling session are covered in Study Session 3, Box 3.1. Be sure to question your client sensitively to find out their concerns about VSC (see Figure 9.1).

9.3 Techniques of sterilisation
There are a number of simple and safe techniques for male and female sterilisation (see Figure 9.2) that can be carried out usually as outpatient procedures in hospitals. Most clients will be able to go home on the same day, as post-operative problems are not common. Pre-operative preparation, which includes counselling, is extremely important to ensure the willingness of the client, and to minimise fears and regret.
9.4 Female sterilisation
Female sterilisation is a surgical intervention that provides permanent contraception for women who do not want any more children. It is a safe and simple surgical procedure. Female sterilisation is also known as Tubal Ligation (TL), or ‘tying the tubes’, as well as VSC. TL is the procedure most commonly done in Ethiopia.
9.4.1 Procedure
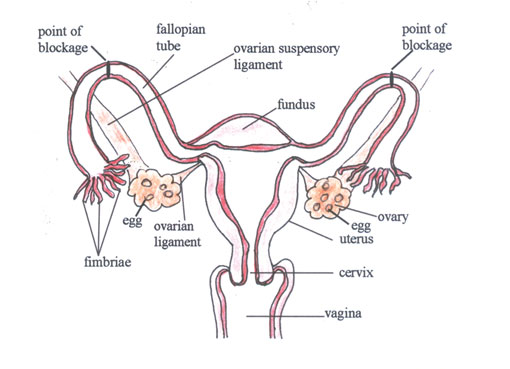
Tubal ligation (TL) is a surgical sterilisation technique for women, where the fallopian tubes are cut, or blocked with rings, bands or clips. This procedure closes the fallopian tubes, and stops the egg from travelling to the fallopian tubes where fertilisation takes place. It also prevents sperm from travelling up the fallopian tube to fertilise an egg (see Figure 9.3 for details). Sterilisation is effective immediately after the procedure. Tubal ligations are 99.5% effective as a birth control method.
When is it most appropriate for women to choose a permanent contraceptive method?
Female sterilisation is ideal for women who are certain that they wish to have no further children, and who need a reliable contraceptive method. It is also an appropriate choice for those for whom subsequent pregnancy may have an undesirable effect on their maternal or child health.
In Ethiopia, tubal ligation is a relatively simple outpatient procedure that has to be done in a hospital. It can be performed under local or general anaesthetic. Minilaparotomy, which involves making small incisions in the lower abdomen, is one of the techniques used in female sterilisation.
After surgery, it is recommended that women take two to three days off and only perform light activities for a week. Sexual activity can start again when a woman feels comfortable, usually after a week. With regard to future fertility, tubal ligation is considered a permanent method of birth control. Surgery to reverse a tubal ligation is not always effective. In addition, reversals are both difficult and expensive.
9.4.2 Sexuality
Women are fully able to enjoy sex after a tubal ligation. Usually, hormone levels and a woman’s menstrual cycle are not affected by sterilisation. The ovaries continue to release eggs, but they remain in the fallopian tubes and are re-absorbed by the body. Some women experience improved sexual pleasure, because they are less worried about becoming pregnant.
9.4.3 Advantages and disadvantages
The advantages and disadvantages of sterilisation for women are summarised in Table 9.1. Being aware of these can help you provide effective counselling to your clients.
| Advantages | Disadvantages |
|---|---|
|
|
9.5 Male sterilisation
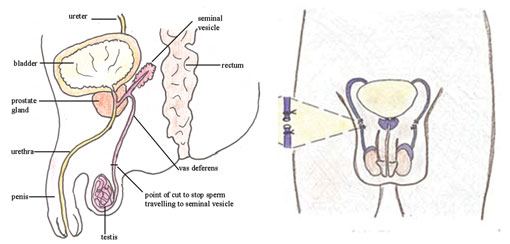
Vasectomy is a permanent method of contraception for men, involving a minor surgical procedure where the vasa deferentia (singular: vas deferens), or sperm ducts, are cut and then tied or sealed (see Figure 9.4). This operation keeps sperm from mixing into the semen when men ejaculate. Without sperm, fertilisation of an egg cannot occur, and so pregnancy is prevented. In Ethiopia, vasectomies are usually done in hospital settings under aseptic (surgically clean) conditions. They are much simpler procedures than female sterilisation, and as a birth control method vasectomies are 99.9% effective.
Is vasectomy the same as castration? How would you explain this to your clients?
No. As you have already learnt, vasectomy is a surgical intervention to the sperm ducts that prevents sperm from reaching and mixing with the seminal fluid ejaculated during sexual intercourse. The procedure does not remove the testicles, and should not be confused with castration. In any discussion with clients, you might want to use appropriate and socially acceptable words in the local language, to best explain what is happening technically.
9.5.1 Procedure
During a vasectomy local anaesthetic is used. The healthcare provider makes a small opening in the skin of the scrotum. This allows the sperm tubes, or vasa deferentia, to be seen and cut. The procedure itself takes about 15 minutes.
Men usually rest at the hospital after the procedure. When they return home, ice packs and painkillers can ease swelling and discomfort. It is recommended that men take two days’ rest, and perform only light activities for a week. For two days, it is helpful to wear scrotal supports and not take a bath. It may take a week for men to feel comfortable and ready for sexual activity.
![]() Vasectomies are not immediately effective. The sperm which was in the tubes before the operation still needs to be ejaculated.
Vasectomies are not immediately effective. The sperm which was in the tubes before the operation still needs to be ejaculated.
Vasectomies are not immediately effective after the operation. The sperm which was in the tubes before the operation still needs to be ejaculated. This may take about a month, or 10–30 ejaculations. Therefore, it is important to use other forms of birth control until the remaining sperm are cleared from the tubes.
Similar to tubal ligation, vasectomy is a permanent sterilisation technique. In developed countries, reversal surgery is available, but not always effective. The reversal procedure rejoins the cut ends of the vas deferens, but it is not always successful.
9.5.2 Sexuality
Men are able to fully enjoy sex after having a vasectomy. Hormonal levels and the feeling of orgasm stay exactly the same. In addition, the amount of fluid men ejaculate does not noticeably change. Some men experience improved sexual pleasure, because they no longer have to worry about making their partner pregnant.
9.5.3 Advantages and disadvantages
The advantages and disadvantages of sterilisation for men are summarised in Table 9.2. Knowing these will help you provide effective counselling to your community.
| Advantages | Disadvantages |
|---|---|
|
|
Summary of Study Session 9
In Study Session 9, you have learned that:
- Both male and female sterilisation can be carried out using local anaesthesia with light sedation under strict aseptic conditions and practices to avoid infection.
- The pre-operative counselling process is very important. You need to tell the client that VSC is almost always irreversible. Therefore, once the client has undergone the procedure, it will be very difficult for them to have children again. Additionally, you need to make sure that the decision for or against sterilisation is made by the client and is not pressured or forced on them by anyone else.
- Tubal ligation is the female sterilisation procedure which involves blocking the fallopian tubes to prevent the egg from travelling down the tubes to where fertilisation takes place. It also prevents sperm from moving up the fallopian tubes to fertilise an egg.
- Women are able to fully enjoy sex after a tubal ligation. Some women experience improved sexual pleasure because they are less worried about becoming pregnant.
- Vasectomy is a permanent method of contraception for men, involving a minor surgical procedure where the vasa deferentia, or sperm ducts, of a man are cut and then tied to prevent the sperm from mixing into the semen when men ejaculate.
- The sperm that were already in the vasa deferentia before the operation need to be ejaculated in order for the vasectomy to be effective. This may take about a month, or 10–30 ejaculations.
- One of the major advantages of VSC is that it is a permanent birth control method, and cost-effective in the long run.
Self-Assessment Questions (SAQs) for Study Session 9
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 9.1 (tests Learning Outcome 9.2)
A 23-year-old, unmarried man has come to your health post to get information on permanent contraceptive methods. At the moment he is not sure whether he would like to have children in the future.
What would you tell him concerning VSC?
Answer
Your answer should include some of these questions:
- Can you tell me why you want to have VSC?
- You are only 23 years old, which is very young to have VSC. Do you realise it is a permanent method of contraception?
- Do you have a partner? If so, does your partner want to have children in the future?
- Do you already have a family? If not, are you sure you won’t want to have children in the future? If yes, are you sure you won’t want to have more children in the future?
- Do you think you might change your mind later? What might change your mind? For example, suppose one of your children died? Suppose you lost your spouse and you married again?
- VSC is irreversible. Have you thought about other contraceptive methods?
Your client may need encouragement to further consider his decision about sterilisation. As a provider, you can advise your client about other methods of contraception, and help him make an informed choice.
Ultimately, the decision about sterilisation belongs to the client alone. A man or woman may consult a partner and others about the decision to have sterilisation, and may consider their views, but the decision cannot be made for them by a partner, another family member, a healthcare provider, a community leader, or anyone else. It is your duty to make sure that the decision for or against sterilisation is made by the client and is not pressured or forced by anyone.
SAQs 9.2 to 9.5
These SAQs are based on Figures 9.3 and 9.4 in this study session. You may also find it helpful to refer to Study Session 3 in the Antenatal Care Module.
SAQ 9.2 (tests Learning Outcome 9.3)
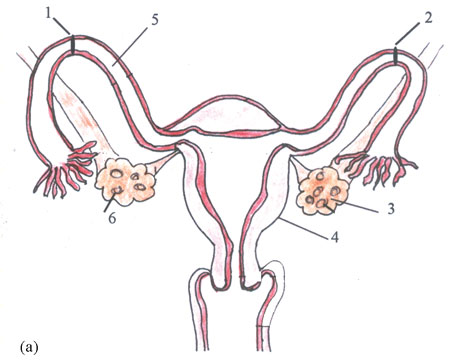
Name structures 4 and 5 in Figure 9.5(a) and describe their function with regard to fertilisation.
Answer
Structure 4 in Figure 9.5(a), is the uterus. Its function is receiving the fertilised ovum and creating a favourable environment for the fetus to develop.
Structure 5 in Figure 9.5(a), is the right fallopian tube. Its main function is hosting fertilisation and transporting the fertilised egg to the inner part of the uterus, where implantation takes place.
SAQ 9.3 (tests Learning Outcome 9.3)
What will happen if structures 1 and 2 in Figure 9.5(a) are blocked?
Answer
If the pathway at structures 1 and 2 in Figure 9.5(a) is blocked it will result in female sterilisation. The blocks prevent the sperm from reaching an egg, and as a result fertilisation and implantation will not take place.
SAQ 9.4 (tests Learning Outcome 9.3)
What will happen to 6 if the pathway is blocked at 1 and 2 in Figure 9.5(a)?
Answer
If the pathway at structures 1 and 2 in Figure 9.5(a) is blocked then the eggs (structure 6.) will remain in the fallopian tube and be reabsorbed by the body. Sterilisation does not usually affect hormone levels and the ovaries will continue to release eggs as part of the normal menstrual cycle.
SAQ 9.5 (tests Learning Outcomes 9.3, 9.5 and 9.6)
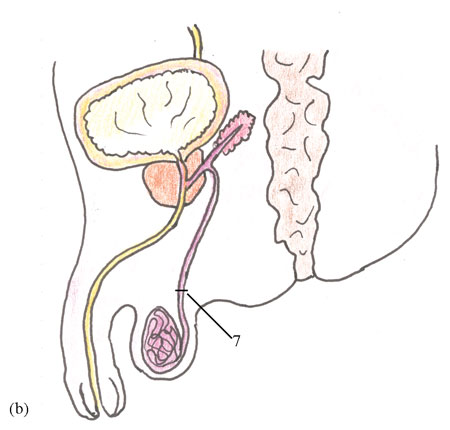
Discuss the advantages and disadvantages of blocking structure 7 in Figure 9.5(b)?
Answer
Blocking structure 7 (left sperm tube or vas deferens) in Figure 9.5(b), is the procedure known as vasectomy, and results in male sterilisation. Its advantages and disadvantages are detailed below.
| Advantages | Disadvantages |
|---|---|
• Permanent birth control. • Requires no daily attention. • Does not affect sexual pleasure. • Less complicated than female sterilisation. | • Not immediately effective. • Requires minor surgery in a hospital. • May not be reversible. • Possible regret. • Possible rejoining of the vas deferens. • Does not protect against STIs, including HIV/AIDS. |
SAQ 9.6 (tests Learning Outcome 9.2)
Why is effective counselling important before carrying out male or female sterilisation?
Answer
Effective counselling is very important before carrying out either a tubal ligation or a vasectomy because these procedures are permanent and almost always irreversible. Clients who do not have sufficient reasons for choosing a permanent contraceptive method at the time of their decision are more likely to regret it later. For women electing VSC following childbirth, thorough counselling during pregnancy, and a decision made before labour and delivery, can help to avoid regrets later.
SAQ 9.7 (tests Learning Outcomes 9.1, 9.2, 9.3, 9.4, 9.5 and 9.6)
Which of the following statements is false? In each case explain why it is incorrect.
A Cutting the fallopian tubes would be enough to sterilise women.
B Cutting and tying both ends of the sperm ducts does not have an immediate effect on male sterilisation. Therefore, an alternative contraceptive method must be used for at least a month after the procedure.
C Many clients assume that cutting the sperm duct is castration.
D Operating on the fallopian tubes in women, and the sperm ducts in men, is very simple and can be done at health-post level.
E Both men and women who have undergone VSC will lose their sexual desire and enjoyment.
Answer
A is false because cutting the fallopian tubes alone would not be enough to sterilise a woman; the tubes have to be tied as well.
B is true. Sperm can remain in the ducts after the operation.
C is true, but this common belief is mistaken.
D is false because operating on the fallopian tubes in women or the sperm tubes in men requires special training and a high degree of skill and is usually done in hospital where aseptic techniques are followed as part of the procedure.
E is false. Clients who have undergone VSC do not lose their sexual desire and enjoyment at all. In women, hormonal levels and the menstrual cycle are not affected, and similarly, men can fully enjoy sex after having a vasectomy. Some couples even experience improved sexual pleasure because they no longer have to worry about the possibility of pregnancy.