Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Tuesday, 14 July 2026, 8:51 AM
Health Education, Advocacy and Community Mobilisation Module: 7. Introduction to Health Communication
Study Session 7 Introduction to Health Communication
Introduction

Communication is an essential part of human life; all meaningful social interaction can be labelled ‘communication’. Without communication an individual could never become a fully functioning human being. Reading, writing, listening, speaking, viewing and creating images are all acts of communication. There are also many more subtle communication activities that may be conscious or unconscious. These include expression, gesture and ‘body language’. Through communication people transfer facts, ideas, emotions, knowledge, attitudes and skills to make informed decisions about their health. In this study session you will learn the basic concepts, levels, roles, principles and types of communication used in health education and health promotion.
Learning Outcomes for Study Session 7
When you have studied this session, you should be able to:
7.1 Define and use correctly all of the key words printed in bold. (SAQ 7.1)
7.2 Describe the role of health communication in health education and health promotion. (SAQs 7.2 and 7.3)
7.3 Discuss some of the basic principles of health communication. (SAQ 7.3)
7.4 Discuss common types of communication. (SAQs 7.3 and 7.4)
7.1 Concepts of communication
Different writers define communication in different ways although the central concept remains the same. The word communication is derived from the Latin word ‘communis’ which means to form a common ground of understanding, to share information, ideas or attitudes and to impart or transmit information. The common feature of these definitions is the transmission or exchange of information. Communication implies the sharing of meaning among those who are communicating. To engage in communication is therefore to engage in the process by which two or more people exchange ideas, facts, feelings or impressions, so that each gains a common or mutual understanding of the meaning and use of a message.
7.2 Health communication
Health communication is the art and technique of informing, influencing and motivating individuals or larger audiences about important health issues based on scientific and ethical considerations. It includes the study and use of communication strategies to inform and influence individual and community decisions that enhance health. Health communication is recognised as a necessary part of efforts to improve personal and public health (Figure 7.1). In other words, health communication encompasses the study and use of communication strategies to inform and influence individual and community knowledge, attitudes and practices (KAP) with regard to health and healthcare. The benefits of effective health communication are summarised in Box 7.1.

Box 7.1 Elements of health communication
Health communication:
- initiates action
- makes needs known
- exchanges knowledge, attitudes and practices
- helps people understand issues and may change their health beliefs
- establishes and maintains relationships with health providers.
7.3 Objectives of health communication
In any type of communication, whether you are writing or speaking, trying to persuade, inform or educate, there are several general objectives. These include being understood, being accepted, and influencing an action such as a change of behaviour.
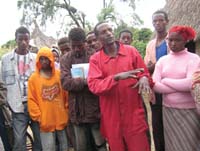
Kidist is a Health Extension Practitioner in the village of Hetosa. She planned to teach her community about environmental sanitation and the benefits of latrine construction. Note down which forms of health communication a Health Extension Practitioner like Kidist might want to use to teach the community about the issue of building and using latrines.
Kidist is likely to inform, influence and motivate community members through health communication. But ultimately, she wants to achieve an action (change of behaviour). There needs to be action so that the latrines are built and used effectively (Figure 7.2). The members of the community asked various questions on the issue of latrine construction. After some discussion the community accepted Kidist’s ideas and agreed to construct the latrine. This is a good example of successful health communication.

Health communication contributes to better health outcomes for individuals and for the whole community. It raises awareness of health risks and solutions, and provides the motivation and skills needed to reduce these risks. It can affect or reinforce good health practices and attitudes, giving people the information they need to make complex choices, such as selecting health plans, care providers and treatments. Health communication also encourages social norms that benefit health and improve quality of life.
Health communication is useful in helping individuals to find support from other people in similar situations. Most importantly health communication can increase appropriate demand for and use of health services. For the community, health communication can be used to influence the public agenda, advocate for policies and programmes, and promote positive change. At the same time it can help improve the delivery of public health and healthcare services (Figure 7.3).

Look at Box 7.2 below and think about two areas where you could use health communication. If you have a chance talk to other health workers, try to find out examples from the list of how and where they have used health communication effectively.
Health communication can be both complex and subtle and different people may focus on different areas. For example one person might generate action through helping people to understand health-related issues, and another by helping them express their needs. Both of these roles will help people to think that bringing about change is a good idea.
Box 7.2 The role of health communication in health education and promotion
- Increases knowledge and awareness of a health issue, problem, or its solution
- Influences perceptions, beliefs, attitudes and social norms about health
- Generates effective action
- Demonstrates or illustrates health related skills
- Shows the benefit of behaviour change
- Increases appropriate use and demand for health services
- Reinforces knowledge, attitudes and behaviour
- Refutes myths and misconceptions
- Advocates for a health issue or a population group.
Read Box 7.3 below, which lists a number of important principles of communication. Some of these are the sorts of things everyone will know and agree with, for example that face-to-face communication is good.
After you have read the box come back to this text and match these examples with the items in Box 7.3.
- a.Combining a leaflet, an audio, a meeting, individual counselling, a demonstration and role playing to get a message across
- b.Talking with someone and asking what they think, rather than talking ‘at’ them
- c.Using simple straightforward language, rather than very big and hard words or being very ‘scientific’ and obscure
- d.Having relevant facts and information gathered together in one place before talking to someone
- e.Having all the information that is going to be needed for an encounter so that nothing is missing and everything is tied up
- f.Talking directly to someone if at all possible when communication is required
- g.Making sure as much as possible that both sides in a communication see things in the same way.
Box 7.3 Principles of communication
- Shared perception: for communication to be effective the perception of the sender should be as close as possible to the perception of the receiver. The extent of understanding depends on the extent to which the two minds come together.
- Sensory involvement: the more senses involved in communication, the more effective it will be. If I hear, I forget. If I see, I remember. If I do, I know.
- Face to face: when communication takes place face-to-face it is more effective.
- Two-way feedback: any communication without a two-way process is less effective because of lack of opportunity for concurrent, timely and appropriate feedback.
- Clarity: ideas, facts and opinions should be clear to the sender before communication happens. Communication should always use direct, simple and easily understandable language.
- Correct information: the sender should have at hand correct, current and scientific information before communicating it.
- Completeness: subject matter must be adequate and full. This enables the receiver to understand the central theme or idea of a message. Incomplete messages may result in misunderstandings.
The examples (a) to (g) illustrate the following principles of communication from Box 7.3.
- a.illustrates sensory involvement
- b.illustrates two-way feedback
- c.illustrates clarity
- d.illustrates correct information
- e.illustrates complete information
- f.illustrates face-to-face communication
- g.illustrates shared perception.
None of this is difficult or indeed anything that people won’t understand. Most people are very good at communication and know what to say when and to whom. However, as a Health Extension Practitioner it is part of your role to be skilled in communication and use it professionally. So be sure to try to analyse what goes on and what works in health education. Although we can all do it, we can all learn to do it better!
7.4 Levels of health communication
The more levels a communication programme can influence, the greater the likelihood of creating and sustaining the desired change. This section outlines the different levels at which health communication can take place.
7.4.1 Individuals
The individual is the most fundamental target for health-related change, since it is individual behaviours that affect health status. Communication can affect an individual’s awareness, knowledge, attitudes, self-efficacy, and skills for behaviour change. For example, counselling on sexual risk reduction as well as HIV testing is an effective way to change behaviour and protect health.
7.4.2 Social networks

An individual’s relationships and the groups (including family), to which they belong can have a significant impact on his or her health. Health communication programmes can work to shape the information a group receives and may attempt to change communication patterns within the group. Opinion leaders within a network are often a point of entry for health programmes such as family-based HIV counselling and testing, or peer education. Targeting health communication at social networks may result in a diffusion of innovations and network-based health strategies. It can also provide opportunities for voluntary counselling and health tests for all network members.
7.4.3 Organisations
Organisations include formal groups with a defined structure such as associations, clubs, worksites or schools. Organisations can disseminate health messages to their members, provide support for individuals and make policy changes that enable individual change. Examples include institution-based health programmes providing services such as voluntary counselling and health testing, or antenatal and child health services (Figure 7.4). These are often available within workplaces, schools and other institutional settings.

7.4.4 Communities

The collective wellbeing of communities can be fostered by creating structures and policies that support healthy lifestyles and reduce or eliminate hazards in social and physical environments.
Community-level initiatives are planned and led by organisations and institutions that can influence health such as schools, worksites, healthcare settings, community groups and government agencies.
7.4.5 Society
Society as a whole has many influences on individual and community behaviour, including norms and values, attitudes and opinions, and laws and policies. Society also creates a physical, economic and cultural environment.
Communicating at the society level can include using the mass media and other types of social mobilisation. For example, HIV or TB educational programmes can be achieved through school, church and workplace education programmes (Figure 7.5).
Suppose you wish to design a communication strategy on the promotion of family planning. The majority of the couples in your community may lack appropriate information about contraceptive methods. Also, the culture is such that children are considered an asset for the community. Many grandparents, in-laws and other key community members believe that contraception is against God’s will. In addition, some healthcare users have reported dissatisfaction with their healthcare providers and tend to discontinue their use of the family planning services. Looking back at the communication levels described in this section, which levels should you design your communication strategy for — and what sorts of things do you think will be important at each level?
Your communication would be aimed at different levels. At the individual level and with couples you can influence factors such as knowledge, beliefs, attitudes and values. At the family or social network level you have to give attention to reinforcing factors such as the attitude of grandparents and husbands towards using contraception. Finally, at the organisational level you should consider any enabling factors such as whether contraceptives are available in your locality or not.
7.5 Types of communication
7.5.1 One-way communication
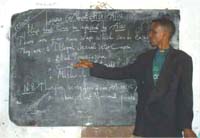
If the flow of information from the sender to the receiver is one-way the communication is dominated by the sender’s knowledge and information is poured out towards the receiver (Figure 7.6). This model does not consider feedback and interaction with the sender (look at the principles in Box 7.3 again). A familiar example of this model is the lecture method used in a classroom, where the teacher stands at the front of the class and lectures on a subject without any interaction or activities (Figure 7.7). Unless mechanisms are put in place to get feedback from the audience, many mass media communication methods are one-way.
One-way communication isn’t in itself wrong and there times when it is very useful — as Table 7.1 illustrates. Think of a situation when one-way communication is used effectively.
This model is commonly used in awareness creation. One-way communication is best used by organisations when the message is simple and needs to be communicated quickly, for example if an organisation wants people to be aware of the date and time of a public meeting.
| Advantages | Disadvantages |
|---|---|
● Faster ● Orderly ● Learning of facts is authoritative | ● Little audience participation ● No feedback ● Does not influence behaviour |
7.5.2 Two-way communication
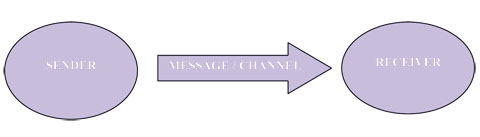
In this model the information flows from the sender to the receiver and back from receiver to the sender again in the other direction (Figure 7.8). Two-way communication is reciprocal, the communicant (receiver) becomes the communicator (sender) and the communicator (sender) in turn becomes a communicant (receiver). Most ordinary conversations are along the lines of this model (Figure 7.9). Two-way communication is usually more appropriate for problem-solving situations.


As a health worker, or just in normal life, you often have cause to have a conversation with people. Think about one recent conversation and look Table 7.2 below to see whether you agree with the advantages and disadvantages of this type of communication.
There are no right or wrong answers to this question, but this has been a chance to begin to assess the qualities of two-way communication that will be useful in your work.
| Advantages | Disadvantages |
|---|---|
● More audience participation ● Learning is more democratic ● Open to feedback ● May influence behaviour change | ● Slower, takes more time |
Box 7.4 summarises some key terms for two-way communication.
Box 7.4 Key terms for two-way communication
Sender: the originator of each message — this could be an individual, group or organisation.
Message: the idea being communicated.
Channel: the means by which a message travels from sender to receiver.
Receiver: the person for whom the communication is intended.
Effect: the change in the receiver’s knowledge, attitude or practice.
Feedback: telling what they have done well or how to improve. Two-way feedback means that members of the community can tell you what you communicated well and what didn’t work so well.
Body Mass Index (BMI) is a measure of a person’s weight, taking their height into account. Very low or very high BMI is a health risk.
Using the example of body mass index (BMI), note down possible examples for each component of two-way communication listed in the key terms above.
Possible examples:
- The sender may be an individual or groups or organisations who are keen to help people to think about their BMI.
- The message might be something like ‘check your body mass index’.
- The channel could be verbal, for example during peer education. Printed materials or audiovisual channels could be used for other messages about BMI to wider audiences.
- The receiver may be an individual, family or the whole community.
- The effect will be the change in the receiver’s attitude, knowledge and practice.
- Feedback should be positive when the desired change in knowledge, attitude and practice (KAP) occurs — but will be negative when the desired change in knowledge, attitude and practice doesn’t occur.
Summary of Study Session 7
In Study Session 7 you have learned that:
- Communication is the process by which two or more people exchange ideas, facts, feelings or impressions so that each person gains a common or mutual understanding of the meaning and the use of the message.
- Health communication is the art and technique of informing, influencing, and motivating individuals, institutions and large public audiences about important health issues.
- All health communication is aimed at achieving four objectives: to be received, understood, accepted and if possible to get action (a change of behaviour).
- Health communication plays a significant role at all levels of disease prevention and health promotion.
- Part of the role of health communication is to increase knowledge and awareness of a health issue and to influence beliefs and attitudes, as well as showing the benefits of behaviour change.
- In order to bring about the desired behavioural changes, health communication should be targeted at several levels.
- Health Extension Practitioners should know the basic principles of communication. If the flow of information from the sender to the receiver is one-way the communication will be dominated by the sender’s knowledge.
- Two-way communication, where information flows from the sender to the receiver and back again, is reciprocal and is therefore more appropriate for problem solving and probably for achieving behavioural change.
Self-Assessment Questions (SAQs) for Study Session 7
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 7.1 (tests Learning Outcomes 7.1, 7.2 and 7.3)
One of the services that Health Extension Practitioners are currently delivering is about HIV/AIDS and TB. Health communication is vital for delivering this service effectively. If you were conducting a health education programme on HIV/AIDS for young people, which of the communication objectives below would you want to achieve? Justify your choice.
- a.To create understanding on HIV/AIDS in the minds of young people
- b.To help young people so that they can accept the message delivered
- c.To get the young people to act on the required behaviour
- d.All of the above
- e.None of the above.
Answer
The answer is d. — all of the communication objectives listed. In any type of communication, whether you are writing or speaking, trying to persuade, inform, explain, convince or educate the general objectives would be first to create an understanding of HIV/AIDS in the minds of young people, second help them to accept the message delivered, and finally to influence the young people to change their behaviour.
SAQ 7.2 (tests Learning Outcome 7.2)
Give some examples of how health communication can help a. individuals, and b. communities.
Answer
You will need to have read the text very carefully to have found the following answers as they are not in a box or list.
- a.For individuals, health communication:
- Contributes to better health outcomes
- Raises awareness of health risks and solutions
- Provides the motivation and skills needed to reduce these risks
- Affects or reinforces good health practices and attitudes, and gives people the information they need to make complex choices, such as selecting health plans, care providers and treatments
- Helps individuals to find support from other people in similar situations.
- b.For the community, health communication:
- Encourages social norms that benefit health and improve quality of life
- Can increase appropriate demand for and appropriate use of health services
- Can be used to influence the public agenda, advocate for policies and programmes and promote positive changes in socio-economic and physical environments
- Can help improve the delivery of public health and healthcare services.
SAQ 7.3 (tests Learning Outcomes 7.2, 7.3 and 7.4)
Which of the following statements is false? In each case explain why it is incorrect.
A For communication to be effective the perception of the sender should not be as close as possible to the perception of the receiver
B One-way communication is dominated by the sender’s knowledge.
C Any communication without a two-way process is less effective because of lack of opportunity for appropriate feedback.
D In health communication, the more sensory organs involved in a communication the less it is effective.
Answer
A is false. For communication to be effective the perception of the sender should be as close as possible to the perception of the receiver. The extent of understanding depends on the extent to which the two minds come together.
B is true. One-way communication is dominated by the sender’s knowledge.
C is true. To meet the communication objectives (raise awareness, promote acceptance and bring about behavioural change) a two-way process is effective because there is opportunity for reciprocal, timely and appropriate feedback.
D is false. The more sensory organs involved in a communication the more effective is will be.
SAQ 7.4 (tests Learning Outcome 7.4)
Discuss some of the differences between one-way communication and two-way communication.
Answer
In one-way communication the flow of information is from the sender to the receiver. The communication is dominated by the sender’s knowledge and learning is authoritative. This model does not consider feedback and interaction with the sender.
During two-way communication information flows from the sender to the receiver and back again. This model is reciprocal and roles are interchanged. Two-way communication is more appropriate in problem-solving situations and there is more participation and feedback, learning is democratic and it can more easily influence behaviour change. However, this type of communication takes more time.