

4 Identifying the key pathogens in global AMR surveillance
4.1 The eight key pathogens
Eight key bacterial pathogens in humans have been identified by the World Health Organization (
| Pathogen | Gram reaction |
|---|---|
| Staphylococcus aureus | Gram positive |
| Streptococcus pneumoniae | |
| Acinetobacter species | Gram negative |
| Escherichia coli | |
| Klebsiella pneumoniae | |
| Neisseria gonorrhoeae | |
| Salmonella species | |
| Shigella species |
E. coli, K. pneumoniae and Acinetobacter species have been selected by WHO for AMR surveillance as all have globally widespread strains which are multi-drug resistant (
-
Why has N. gonorrhoeae been chosen out of all the pathogens causing sexually transmitted infection (
STI ) as a focus for surveillance? -
Infection with N. gonorrhoeae leads to a lot of morbidity including pelvic inflammatory disease and infertility. Resistance is a big problem – especially to oral antibiotics. Some strains are already only sensitive to
IV antibiotics, and untreatable strains are a becoming a possibility. N. gonorrhoeae can be cultured in a clinical laboratory whereas it is not possible to test the organisms that cause Chlamydia, Syphilis etc. for AMR. Resistance is, fortunately, less of an issue so far with these organisms.
Activity 11: Usual isolation site of key pathogens
For each of the images below, can you identify the site you would expect them to be isolated from? Note: for some pathogens, there may be more than one site.
Click 'reveal discussion' to see the answer.

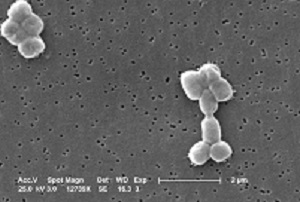
Which site or sites in the body is S. aureus isolated from?
Discussion
Answer: S. aureus is a common cause of infection in the community and of healthcare associated infection (
For
Which site or sites in the body is S. pneumoniae isolated from?
Discussion
S. pneumoniae is a common cause of pneumonia, meningitis and ear infections, as well as infections in HIV patients. It is typically isolated from bloodstream samples in severe infections. It can also be found in upper respiratory and surface swabs, sputum and
GLASS surveillance focuses on bloodstream infection isolates.
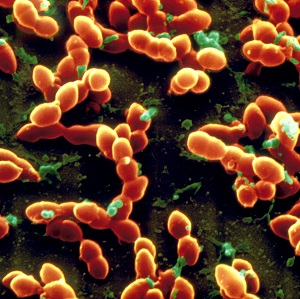
Acinetobacter are gram-negative, coccobacillary-shaped bacteria. A. baumannii accounts for most Acinetobacter infections in humans and is the species of concern. However, identification to species level is technically challenging so many sites report as Acinetobacter species only.
Which site or sites in the body are Acinetobacter species isolated from?
Discussion
Acinetobacter are classic
For GLASS, bloodstream isolates are the focus of interest.
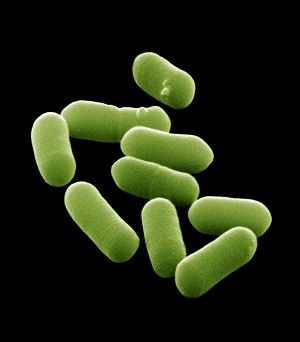
Which site or sites in the body is E. coli isolated from?
Discussion
E. coli is the most common cause of
E. coli is typically isolated from bloodstream and urine. They can also be isolated from stools, but this requires special techniques to distinguish the pathogenic strains from commensal E. coli which is prevalent in the gut.
For GLASS, isolates from bloodstream and urine are the focus of interest.

Which site or sites in the body is K. pneumoniae isolated from?
Discussion
K. pneumoniae is a common cause of HCAI including
K. pneumoniae is typically isolated from bloodstream and urine samples and GLASS focuses on these. It can also be found in swabs and sputum samples, but it is harder to be sure it is acting as a pathogen rather than colonising these sites.
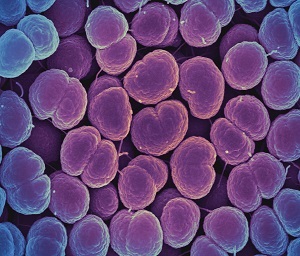
Which site or sites in the body is N. gonorrhoeae isolated from?
Discussion
N. gonorrhoeae causes the
For GLASS, N. gonorrhoeae isolated from genital samples are the focus.
Which site or sites in the body are Salmonella species isolated from?
Discussion
Enteric fever is caused by S. typhi/paratyphi with the other non-typhoidal strains causing diarrhoeal disease. Enteric fever strains only affect humans, but the other strains can also be transmitted via animals and animal products. This is important in the
For GLASS, Salmonella isolated from both stool and blood samples are the focus.
Which site or sites in the body are Shigella species isolated from?
Discussion
Shigella species cause diarrhoeal disease and cause significant morbidity in young children.
For GLASS, Shigella isolated from stool samples are the focus.
Your laboratory is almost certainly identifying other organisms than the ones listed in Activity 11. However, the focus of this module is on some of the issues around identifying the eight key GLASS pathogens under global AMR surveillance. Your laboratory should have comprehensive
3.3 Advanced testing
