Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Thursday, 9 July 2026, 1:10 AM
Non-Communicable Diseases, Emergency Care and Mental Health Module: 2. Diabetes Mellitus
Study Session 2 Diabetes Mellitus
Introduction
Diabetes is currently becoming a common problem in developing countries like Ethiopia, at a time when the burden of diabetes is rising very quickly in wealthier countries. Chronic diseases such as diabetes, heart disease, cancers and chronic respiratory diseases are by far the leading causes of mortality in the world, representing 60% of all deaths.
Chronic diseases are those that develop slowly, get progressively worse unless they are treated effectively, and cause long-term health problems.
In this study session you will learn about diabetes, the parts of the body involved, and the signs and symptoms that will allow you to recognise if someone in your community is suffering from the disease. You will also learn how to recognise the different types of diabetes and their risk factors, as well as how to educate the community to reduce these risks.
Learning Outcomes for Study Session 2
When you have studied this session, you should be able to:
2.1 Define and use correctly all of the key words printed in bold. (SAQs 2.1, 2.2, 2.3, 2.6 and 2.7)
2.2 Describe how the pancreas, liver and muscles, and the hormones insulin and glucagon, are involved in regulating blood glucose levels. (SAQs 2.2 and 2.5)
2.3 List the signs and symptoms of diabetes and distinguish between Type 1, Type 2 and gestational diabetes. (SAQs 2.1 and 2.3)
2.4 Describe the test that you would do to confirm a diagnosis of diabetes. (SAQ 2.4)
2.5 List the risk factors for diabetes. (SAQs 2.5 and 2.7)
2.6 Explain how to interpret the Body Mass Index (BMI) and its significance for diabetes. (SAQ 2.6)
2.7 Describe the basic features of diabetic self-care and a suitable diet for someone with diabetes. (SAQs 2.1, 2.5 and 2.7)
2.1 What is diabetes mellitus?
Diabetes mellitus is a condition in which the level of glucose (the simplest type of sugar) in the blood is poorly controlled, so that sometimes it rises too high and at other times it falls too low. Both these extremes can have serious consequence, for the diabetic person. Later in this study session we will explain how glucose is normally regulated and how it goes wrong in diabetes. People with diabetes mellitus are usually very thirsty, so they drink a lot of fluids and as a consequence they produce large amounts of urine. There is another type of diabetes, called diabetes insipidus, but it is very rare. Diabetes insipidus shares the name ‘diabetes’ because it also results in the production of large quantities of urine, but this has nothing to do with how the body manages glucose. This study session will focus only on diabetes mellitus, and from this point that is what we mean when we mention ‘diabetes’.
Diabetes mellitus has been known for thousands of years, having been described by the Ancient Egyptians and the Romans. The word ‘mellitus’ comes from the Latin word for ‘honeyed’ – meaning ‘sweet’.
Diabetes mellitus, therefore, describes a condition that produces ‘sweet urine’ (Figure 2.1). This production of sweet urine occurs as a result of a high glucose level in the blood, which results in glucose leaking into the urine when the kidneys filter the blood to remove impurities.

Describe a simple way to test urine or a sign of diabetes.
Anyone can test their own urine by urinating into a clean container like a pot or a cup, and leaving the container outside. If ants climb into the container (Figure 2.1), there is probably sugar in the urine. (Did you remember this from your study of the Antenatal Care Module? It was in Study Session 9, Figure 9.14).
2.2 How the body regulates blood glucose levels
Understanding how the body controls and uses glucose in a normally healthy person will help you to understand what happens when diabetes develops. First we will briefly introduce the main cells, tissues and hormones involved in glucose regulation.
2.2.1 Hormones in glucose regulation
The main role of glucose in the body is like fuel in a car: glucose is a source of energy in human beings. When you are in good health the body controls the level of blood glucose and doesn’t allow this to become very high or very low. The normal range is 75-115 mg (milligrams) of glucose in every 10 ml of blood. Glucose control is due to the action of hormones.
10 ml is called a ‘decilitre’ (dcl); blood glucose levels are usually expressed in mg/dcl of blood.
Hormones are signalling substances produced by collections of cells, called endocrine glands, which release their hormones into the blood. Cells are the tiny building blocks of the body, which can only be seen through a microscope. In the human body there are many different types of cell doing many different tasks. Hormones are carried around the body in the blood and on that journey they interact with whichever ‘target tissue’ is receptive to their signals. There are many different hormones acting throughout the body. Insulin and glucagon are the two most important hormones involved in the control of blood glucose levels. Other examples of hormones that you encountered in the Antenatal Care Module are the male and female reproductive hormones: testosterone, progesterone and oestrogen.
2.2.2 The pancreas
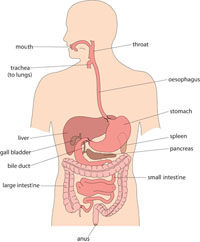
The pancreas is a ‘leaf-shaped’ organ found deep inside the abdomen. The abdomen is the part of the body between the chest and pelvis. The abdomen contains such organs as the stomach, liver, spleen, pancreas, intestines and other structures (see Figure 2.2).
Alpha and beta are the first two letters in the Greek alphabet; they can also be written as the Greek symbols α and β.
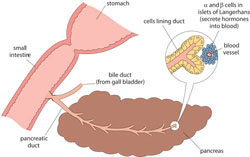
The pancreas has a short connecting tube (the pancreatic duct, see Figure 2.3), which opens into the small intestine so that pancreatic juices can help with the process of digestion (as you learned in the Nutrition Module). Specialised cells in a part of the pancreas called the islets of Langerhans (after its discoverer) produce the hormones insulin and glucagon. The beta cells produce insulin and the alpha cells produce glucagon. When the body is healthy these two hormones help to keep the amount of glucose in the blood at the right level. If the pancreas is severely damaged or removed by operation, the production of insulin and glucagon will stop and diabetes will result.
2.2.3 Insulin and its role in glucose regulation
Insulin has many functions, but its main role is to help glucose enter into the body’s cells, so they can use it as a fuel for all the processes that need energy. The pancreas releases insulin into the blood when we eat a meal.
Can you suggest why this timing is important?
As we digest our food, the level of glucose in the blood rises as it is absorbed from the intestines. It makes sense for insulin levels also to rise in response to the increase in blood glucose.
Insulin enables glucose to be transported into the cells that need it as a source of fuel, and it also prevents the glucose level in the blood from rising too high when we eat a sugary meal. It acts on the liver, muscles and body fat, stimulating them to take up excess glucose and store it, and it stops stored glucose from being released from these tissues when the level in the blood is already too high.
Between meals and overnight the insulin level in the blood falls. If this did not happen, what would be the effect on the blood glucose level, and why?
It would become too low, because insulin would go on stimulating the body’s cells to take up glucose from the blood and to store it in the liver, muscles and body fat.
So, adjustments in the amount of insulin released by the pancreas regulate the blood glucose level to stay within the tight range that the body needs to function normally. In a person with diabetes mellitus, problems in insulin production result in poor regulation of blood glucose, with serious effects, as you will see later in this study session.
2.2.4 Glucagon
The action of the hormone glucagon works in the opposite direction to insulin. Glucagon causes the blood glucose level to rise if it has fallen too low. It does this by stimulating the liver, muscles and body fat to release their stored glucose back into the blood.
You may wonder why the body needs a hormone to increase glucose levels. Besides regulating the blood glucose level so that it does not rise too high, the body also needs to be protected from glucose levels that are too low. The brain does not function properly if glucose levels in the blood drop even a small amount below normal, and if they drop further still the person becomes confused and eventually becomes unconscious. Brain damage and eventually death results if the brain is starved of glucose for a long period.
2.3 Digestion of the main food groups
The glucose in the blood is one of the most important breakdown products from a wide range of the foods we eat in our diet. In this section, we briefly summarise the significant points about digestion and the main food groups, so you understand how to counsel a person with diabetes about selecting a suitable diet for their condition. The main food groups are:
- Proteins such as meat, fish, egg yolk and soya products;
- Fats such as butter and oil, and within foods such as cheese, cream and fatty meat;
- Carbohydrates such as injera, bread, potatoes, rice and cereals, as well as within sugary foods and drinks;
- Vitamins and minerals (such as vitamin A and iron) are found in many foods, especially in fruits and vegetables.
The foods that we eat are broken down as they pass through the digestive tract (look back at Figure 2.1) by chemicals known as enzymes. Enzymes are chemical substances produced by cells in the body, which cause a particular chemical reaction to happen while not being changed themselves. They are particularly important in digestion. The enzymes that are released into the stomach and intestines cause the breakdown of food into the tiny molecules of which it is constructed.
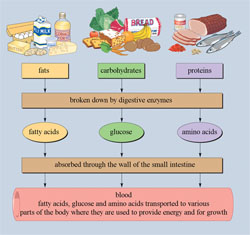
Figure 2.4 summarises the digestion of the main food groups by digestive enzymes. Notice that they break down proteins into amino acids, carbohydrates into glucose, and fats into fatty acids. These smaller components can then be absorbed through the wall of the small intestine and transported in the blood to various parts of the body to provide energy. The level of glucose in the blood is altered by what and how much we eat.
Which food item do you think will result in more glucose in the digestive tract: a carbohydrate-rich meal or a protein-rich meal?
If you eat a meal that is mainly carbohydrate, your digestion will produce more glucose.
Next we will discuss the importance of the liver and muscles in controlling blood glucose levels.
2.3.1 The liver in glucose regulation
The liver is a large and important organ, with many functions, which lies across the top and towards the right of the abdomen (look back at Figure 2.2). As you already know, it is important in helping to control glucose levels, by storing excess glucose and releasing it back into the blood when the level falls too low. Insulin stimulates the liver to take up glucose and change it into glycogen, a substance made of chains of glucose units stuck together. You can think of glycogen as a storage form of glucose.
If there is plenty of glucose in the blood, the body makes glycogen to use later, at times when glucose is scarce. For example, to keep the blood glucose level constant in the body overnight (when one is not eating), the liver slowly releases glucose from its glycogen stores. After a meal when there is plenty of glucose in the blood, the liver stores glucose as glycogen again. Similarly, when you exercise and need additional fuel, the liver can slowly release glucose to provide energy.
2.3.2 The muscles in glucose regulation
There are different sorts of muscles in the body and they have different functions. Skeletal muscles are the ones used for movement, for example in your arms and legs. The involuntary muscles are the ones over which we have no conscious control, for example the muscles in the walls of the stomach and intestines that move food through the digestive tract.
Like the liver, skeletal muscles store glucose as glycogen and are able to use glucose as a fuel. Insulin stimulates muscles to take up glucose. When the muscles are active (for example, while exercising), the absorbed glucose is used to fuel muscular activity.
2.3.3 Fats and diabetes
Fats in the body have an important role in diabetes. Being overweight or obese increases the health risk for people who are already diabetic, and it is a significant risk for developing diabetes in later life. We say more about this later. The breakdown of fats in the body as an alternative source of fuel to glucose is more likely to occur in people with diabetes, because their cells cannot take up glucose easily when insulin levels are low. When fats are broken down to be used as fuel, one of the side-effects is the production of small molecules called ketones. They can build up to dangerously high levels in a person with diabetes, making the blood too acid (the condition is called ketoacidosis), and the person’s breath has a distinctive ‘fruity’ smell.
Ketoacidosis is pronounced ‘kee-toh-assid-oh-siss’.
2.4 Symptoms and signs of diabetes
A person who has untreated diabetes is likely to complain of symptoms like feeling thirsty all the time, drinking a lot of water and passing large amounts of urine, weight loss (some patients describe a feeling of emptiness in the stomach and wanting to eat frequently), and tiredness. The person may report that at times they have felt faint or dizzy and may even have ‘blacked out’ (become unconscious). This can happen if the blood glucose levels fall too low to support normal brain function.
![]() If you detect sugar in a person’s urine you should suspect diabetes and refer them to the nearest higher level health facility.
If you detect sugar in a person’s urine you should suspect diabetes and refer them to the nearest higher level health facility.
If you do a urine dipstick test and find evidence of sugar, this is a strong sign of diabetes because some of the excess glucose in the blood is filtered out by the kidneys and passes into the urine.
Can you suggest another sign of diabetes, which you might be able to detect on the breath of a diabetic person?
When the level of ketones rises in the blood of a person with diabetes, their breath has a distinctive ‘fruity’ smell.
Another sign of uncontrolled diabetes that has gone on for a long time is numbness in the fingers and toes, or gradual loss of vision. This is because persistently high levels of glucose damage the delicate blood vessels (capillaries) serving the extremities and the eyes, so they become starved of oxygen and nutrients and can no longer function normally.
2.5 Classification of diabetes
There are several types of diabetes, including two that are common: Type 1 and Type 2. Worldwide, about 90% of people with diabetes have Type 2 and about 10% have Type 1. Gestational diabetes accounts for very small numbers of cases during pregnancy. We will look at each type in turn.
2.5.1 Type 1 diabetes
Type 1 diabetes was previously called insulin-dependent diabetes. This is because in people with Type 1 diabetes their pancreas fails to produce enough insulin due to the destruction of the cells that make insulin. Without enough insulin, glucose cannot enter the tissues and cells, and so the blood glucose level rises damagingly high. People with Type 1 diabetes are dependent on taking insulin every day – either in tablet form or injecting it.
Although there is plenty of glucose in the blood, it cannot enter the tissues and, because of this, it cannot be used as a fuel source. Instead, the body breaks down fats and protein to use as fuel. As a result, the person often loses weight very rapidly due to loss of fluid, an inability to use glucose as a fuel, loss of muscle as protein is broken down, and loss of glucose in the urine. A person with Type 1 diabetes should never stop taking their insulin, even when they are unwell and not eating. Type 1 diabetes can develop at any age, although it most commonly begins in children and young adults.
2.5.2 Type 2 diabetes
Type 2 diabetes was previously called non-insulin-dependent diabetes, because the pancreas still produces insulin, though the amount reduces over time. The main problem is that the body cells become increasingly resistant to the action of insulin, so it does not stimulate the cells sufficiently to take up glucose from the blood. Symptoms such as thirst and passing large amounts of urine may be absent. Type 2 diabetes may be present for many years before a diagnosis is made, because some people have few symptoms or take no notice of them, e.g. they may not see their thirst or getting up at night to pass urine as a problem. Having Type 2 diabetes for several years before a diagnosis is made can mean that complications of diabetes, which take years to develop, may already be present at the time of diagnosis.
Over-eating and lack of exercise are two particularly important factors thought to be contributing to the rapidly increasing numbers of people worldwide with Type 2 diabetes. Although it is most often a condition that develops in adults, particularly those aged over 40 years, it is beginning to be diagnosed in younger adults and even in teenagers who are obese.
The amount of insulin that is produced in someone with Type 2 diabetes often decreases over a period of years, and eventually insulin treatment is required. Treatment generally starts with changes in the amounts and types of food eaten and an increase in physical activity, before progressing to tablets and then onto insulin injections.
2.5.3 Gestational diabetes
A pregnant woman can develop diabetes in pregnancy, due to chemical changes in her body. This is known as gestational diabetes (also known as pregnancy-induced diabetes). The common symptoms are the same as for Type 1 and Type 2 diabetes (thirst, frequent urination), but she may also complain of itching and an unpleasant smell coming from her vagina due to infection, and wounds that are slow to heal.
Gestational diabetes commonly goes away after the baby is delivered, but you should be aware that a few mothers will have undiagnosed Type 2 diabetes, or have developed coincidental Type 1 diabetes. Also, having had a diagnosis of gestational diabetes, a woman is more likely to develop diabetes in future pregnancies and is also more likely subsequently to develop Type 2 diabetes. During the pregnancy, the woman should be treated for diabetes by changes to her diet and exercise, with or without prescribed insulin.
2.6 Injecting insulin
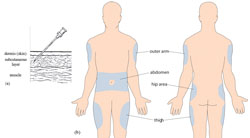
As a community health worker you are expected to teach people with diabetes how to inject themselves with insulin if it is ordered by a doctor. In Study Session 4 of the Immunization Module you learned about giving subcutaneous injections (see Figure 2.5a), i.e. an injection where the tip of the needle penetrates just below the skin into the fatty layer beneath. Insulin is injected subcutaneously using a short fine needle. The usual sites for injection are the thighs, hip area, abdomen or outer arms (Figure 2.5b).
2.7 Risk factors for diabetes
Note that even if all the risk factors are present in the same person it doesn’t mean that they will certainly develop diabetes.
It is important to have a good understanding of the risk factors associated with diabetes, that is, the circumstances that make it more likely that diabetes will develop. Knowing these risk factors can help you make a diagnosis, especially of Type 2 diabetes, and introduce treatment at an early stage. The main risk factors for Type 2 diabetes are listed below:
- A family history of diabetes (genetic factors).
- Being overweight or obese; the distribution of body fat also appears to be important, with fat around the abdomen seen as more of a risk than fat hips.
- Lack of exercise.
There is some indication that a virus infection in early childhood might lead to Type 1 diabetes in some cases; the theory is that the virus in some way causes the person’s own immune system to destroy the insulin-producing cells in their pancreas.
2.7.1 Body Mass Index (BMI)
As mentioned above, being overweight is a risk factor for developing Type 2 diabetes. However, simply weighing someone may not accurately determine if they are overweight.
Explain how it is possible for one person who weighs 80 kg to be obese, and another person who also weighs 80 kg to be a healthy weight.
The key point is their difference in height. One may be taller and assessed as an average weight for their height, whereas the other is assessed as obese because they are much shorter.
The relationship between weight and height is determined by calculating the person’s Body Mass Index (BMI). Your BMI is defined by your weight in kilograms divided by your height in metres and the result is divided again by your height in metres.
BMI is an indicator of how healthy a person’s weight is. Figure 2.6 is a chart that will help you to calculate a person’s BMI and to use this to determine whether they are a healthy weight, underweight, overweight, obese, or extremely obese.
Directions: Find your weight in kilograms (or pounds) along the top of the table and your height in metres (or ft and inches) along the left-hand side. Your BMI is the value at the point in the table where they intersect. NB The chart does not apply to athletes, children, pregnant or lactating women.
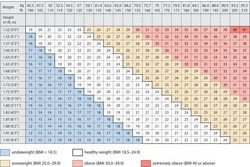
Mr Aseged is 1.70 m tall and weighs 68 kg. Mr Abera is also 1.70 m tall but weighs 93 kg. Use Figure 2.7 to estimate their BMI. What does the BMI of each man indicate about the risk of developing Type 2 diabetes?
Mr Aseged’s BMI is 23, so he is a healthy weight for his height, which does not increase his risk of developing Type 2 diabetes. However, Mr Abera’s BMI is 32, which means he is obese and therefore at increased risk of becoming diabetic.
2.8 Self-care and diet for someone with diabetes
How can you support the people with diagnosed diabetes in your community? If they are already taking insulin or other drugs to treat their condition, you should advise them to take their medication regularly. Everyone with diabetes, regardless of treatment, should:
- attend regular medical checkups
- be aware of possible wound infection if they hurt themselves and seek urgent treatment if this occurs
- always wear shoes that fit correctly; wounds, blisters or sores on the feet can lead to tissue damage that is difficult to heal
- have an eye test once every year to check for early signs of eye damage
- always include exercise as a routine part of their lifestyle
- attend health education classes (if they are available) for people with diabetes to learn about self-care.
2.8.1 Maintaining a healthy diet
Maintaining a healthy diet is one of the most important aspects of treatment for diabetes. Table 2.1 summarises the recommended diet for a person with diabetes, but it is also the healthy balanced diet that everyone would benefit from eating.
You will learn more about all aspects of diets in the Nutrition Module.
| Foods | Can be eaten in moderate amounts | Limited to small occasional amounts |
|---|---|---|
| Carbohydrates | Complex (starchy) carbohydrates should be the main part of any meal, e.g. injera, bread, other cereals, rice, potatoes, etc. Starchy carbohydrates are broken down slowly into sugars, so the glucose levels in the blood rise slowly. | Foods containing sugar are not encouraged, particularly if the person needs to lose weight, because sweet foods are energy-rich and ‘fattening’. Sugary foods and drinks can put up blood glucose levels very quickly and have very little or no nutritional value. |
| Fats | Fats, such as those in olive oil and avocados, are good for maintaining a healthy weight. Grilling, baking and steaming cooking methods produce less fattening foods than frying. | Fats should be limited to help control body weight, especially ‘hard’ fats such as butter and animal lard. |
| Proteins | Protein is found in meat, fish, eggs, nuts, pulses and dairy products, and is recommended in a healthy diet. | Avoid ‘fatty’ sources of protein such as fatty meat, or a lot of egg yolks. |
| Vitamins, minerals and fibre | Fruits and vegetables are an excellent source of dietary fibre, vitamins and minerals; try to eat five portions of fruit and vegetables each day, e.g. ‘gommen’ or kale, cabbage, carrots, spinach, tomatoes, mangoes. | Fruit contains sugar and tends to increase blood glucose levels. People are often surprised at this because fruit is a healthyeating option. |
| Salt | A small amount of salt daily is all that is needed; this can mostly be obtained from fresh natural foods. | Most people eat more salt than is required by the body; food should be tasted before salt is added, if necessary, at the table. Limiting salt intake can help decrease blood pressure. |
Summary of Study Session 2
In Study Session 2, you have learned that:
- Diabetes is a condition in which the level of glucose in the blood is poorly regulated; it is often too high, but may also fall too low.
- Becoming very thirsty, drinking a lot and producing large amounts of urine are symptoms of diabetes; sugar in the urine is a diagnostic sign.
- Insulin and glucagon are hormones produced by cells in the pancreas, with opposite actions, which regulate blood glucose levels within a narrow range.
- Foods are broken down in the digestive system, and nutrients, including glucose, are absorbed into the blood and transported around the body; glucose is used as a fuel for cellular activity.
- Excess glucose is converted into glycogen and stored in the liver, muscles and body fat; it is released back into the blood if glucose levels begin to fall.
- Diabetes is classified as Type 1 (insulin-dependent), Type 2 (non-insulin-dependent) and gestational (pregnancy-induced) diabetes.
- Family history of diabetes, being overweight and lack of exercise are among the main risk factors for Type 2 diabetes.
- Body Mass Index (BMI) is calculated using a chart in which weight and height are used to determine whether a person is a healthy weight for their height. A high BMI is a risk factor for diabetes.
- A person with diabetes should be advised to take their medicine regularly, attend follow-up medical examinations, actively participate in learning about self-care, maintain a healthy diet, and engage in regular physical exercise.
Self-Assessment Questions (SAQs) for Study Session 2
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering the following questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Supporting Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of the Module.
SAQ 2.1 (tests Learning Outcomes 2.1, 2.2, 2.3 and 2.6)
Which of the following statements is false? In each case, explain why it is incorrect:
A Diabetes is a condition in which the blood glucose level is always too high.
B Diabetes is becoming more common in developing countries like Ethiopia.
C Excess glucose is stored in the liver until it is needed.
D Insulin stimulates the liver to release stored glucose when the body needs more fuel.
E Exercise is not recommended for people with diabetes because it depletes the low level of glucose in their blood.
Answer
A is false. Blood glucose can also fall too low in a person with diabetes; the condition is characterised by lack of regulation of blood glucose.
B is true. Diabetes is becoming more common in developing countries like Ethiopia.
C is true. Excess glucose is stored in the liver until it is needed.
D is false. Glucagon (not insulin) stimulates the liver to release stored glucose when the body needs more fuel.
E is false. Exercise is recommended for people with diabetes as part of a healthy lifestyle and maintenance of a normal weight for their height; also, the blood glucose levels of a diabetic person are often too high, as well as sometimes too low.
SAQ 2.2 (tests Learning Outcomes 2.1 and 2.2)
Match each internal organ named in List A in Table 2.2 with the correct description in List B.
| A | B |
|---|---|
| Pancreas | Stores glucose in the form of glycogen and slowly releases glucose from its glycogen stores |
| Liver | Produces many substances including hormones like insulin and glucagon |
| Digestive tract | Used for movement, e.g. in the arms and legs |
| Skeletal muscles | Breaks down foods into smaller nutrients which can be absorbed into the blood |
Answer
The completed version of Table 2.2 appears below.
| A | B |
|---|---|
| Pancreas | Produces many substances including hormones like insulin and glucagon |
| Liver | Stores glucose in the form of glycogen and slowly releases glucose from its glycogen stores |
| Digestive tract | Breaks down foods into smaller nutrients which can be absorbed into the blood |
| Skeletal muscles | Used for movement, e.g. in the arms and legs |
SAQ 2.3 (tests Learning Outcomes 2.1 and 2.3)
Mr Tajebe is a 65-year-old man who developed diabetes two years ago. His condition is controlled by diet alone at the present time. What type of diabetes does he have? Explain the reasons for your answer.
Answer
Mr Tajebe probably has Type 2 diabetes. One reason for reaching this conclusion is that his diabetes only began when he was already 63 years old, and Type 1 diabetes usually starts in children or young adults. Another reason is that his condition is currently being controlled by diet alone; Type 1 diabetes requires daily insulin for its control.
SAQ 2.4 (tests Learning Outcomes 2.3 and 2.4)
List the main symptoms of diabetes that a typical patient could describe to you. How would you test for a diagnostic sign of diabetes?
Answer
The typical symptoms of diabetes are: feeling thirsty all the time and drinking of a lot of fluids, passing large amounts of urine, weight loss, and a feeling of tiredness. The best sign of diabetes is to test the urine for the presence of sugar, using a dipstick for this purpose.
SAQ 2.5 (tests Learning Outcomes 2.2, 2.3, 2.5 and 2.7)
Which of the following statements is false? In each case, explain why it is incorrect.
A Type 1 diabetes might be caused by a virus infection.
B A family history of diabetes increases the risk of developing diabetes.
C People who eat a lot of rice are at high risk of developing diabetes.
D Glucagon is the form in which excess glucose is stored in the body.
Answer
A is true. Type 1 diabetes might be caused by a virus infection.
B is true. A family history of diabetes increases the risk of developing diabetes.
C is false. Eating rice is not a risk factor for diabetes; in fact, eating a slowly broken-down carbohydrate like rice is a good choice for someone with diabetes, because the glucose levels in the body rise only slowly as rice is digested.
D is false. Glycogen (not glucagon) is the form in which excess glucose is stored in the body; glucagon is a hormone produced by the pancreas.
SAQ 2.6 (test Learning Outcomes 2.1, 2.5 and 2.6)
Mrs Aster is 1.6 metres tall and weighs 75 kg. What is her BMI and how would you categorise her weight? Is she at increased risk of developing diabetes?
Answer
Mrs Aster’s BMI is 29. Her weight is at the top end of the ‘overweight’ range – if she gains any more weight she will be categorised as obese. Her weight puts her at increased risk of developing diabetes.
SAQ 2.7 (tests Learning Outcomes 2.1, 2.3, 2.5 and 2.7)
You are asked to produce a poster on reducing the risk of developing Type 2 diabetes. What points do you make on your poster?
Answer
Your poster might say something like:
- Don’t let yourself become overweight!
- Eat a healthy balanced diet with plenty of fruits and vegetables.
- Limit your intake of sugary or fatty foods.
- Exercise every day.