Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Wednesday, 8 July 2026, 8:46 PM
Non-Communicable Diseases, Emergency Care and Mental Health Module: 6. Oral Health
Study Session 6 Oral Health
Introduction
Oral diseases are a significant burden to all countries of the world, including Ethiopia. Oral diseases include tooth decay, leading to painful dental cavities and tooth loss, gum infections that cause teeth to decay and fall out, broken teeth, birth defects such as cleft lip and cleft palate, and cancers in the mouth (oral cancer). The World Health Organization (WHO) estimates that 60–90% of school children worldwide have dental cavities, and severe gum disease is found in 5–20% of middle-aged adults.
With the exception of birth defects (which have a genetic basis), all these oral conditions share common risk factors with the four leading chronic diseases – cardiovascular diseases, diabetes mellitus, cancers, and chronic obstructive pulmonary disease (COPD) – they include unhealthy diet, tobacco use and excessive use of alcohol. Poor oral hygiene is also a risk factor for oral diseases.
In this study session you will learn the basic anatomical structure of the mouth and teeth, and about the common causes of oral diseases and how to promote oral health in your community through improved oral hygiene.
Learning Outcomes for Study Session 6
When you have studied this session, you should be able to:
6.1 Define and use correctly all of the key words printed in bold. (SAQs 6.1, 6.2 and 6.3)
6.2 Explain what oral health means and describe the structures in the oral cavity and their functions. (SAQs 6.1 and 6.4)
6.3 Describe the common oral diseases and their causes. (SAQs 6.2 and 6.3)
6.4 Explain how to decrease the burden of oral diseases in your community by promoting oral hygiene. (SAQs 6.2 and 6.4)
6.1 The oral cavity and oral health
We begin this study session by introducing you to the anatomy and functions of the mouth and its associated structures. This will enable you to understand the oral diseases and disorders described later. According to the WHO, oral health means being free from the following conditions: chronic mouth and facial pain, oral or throat cancer, oral sores, birth defects such as cleft lip and palate, gum disease, tooth decay, and tooth loss.
6.1.1 The oral cavity
Oral hygiene is the practice of keeping the oral cavity (lips, tongue, teeth, throat and surrounding structures, Figure 6.1) clean and healthy to prevent tooth decay and gum disease.

The oral cavity is the entrance to the digestive tract and the respiratory system (look back to Figure 2.2 in Study Session 2 and Figure 4.1 in Study Session 4). A healthy oral cavity has smooth, unbroken lips without any sores. The teeth are not broken or cracked; they are clean and without signs of decay. The tongue and gums are clean and pink, without any greyish coating, bleeding, sores or swelling. The saliva that keeps the mouth moist should be a clear fluid, not thick or coloured white or greenish, which is a sign of infection. The breath emerging from the mouth should be without any smell.
In addition to the teeth, the other structures that aid chewing of food are the lips, cheek muscles, tongue, the roof of the mouth (hard palate), the soft palate (see Figure 6.1) and the uvula. The tonsils are small organs in the throat, containing white blood cells, which help to prevent infection entering the body through the mouth.
6.1.2 Teeth
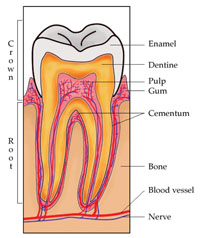
Humans normally produce two complete sets of teeth in our lifetime. The first set are called ‘baby’ teeth or ‘milk’ teeth and there are 20 of them. They usually begin to emerge from the gums at the age of four to six months, but occasionally much earlier. The second set, consisting of 32 permanent teeth, begin to replace the first teeth around the age of six years. If a permanent tooth is damaged or lost, the body cannot replace it. Teeth are the toughest structures in the body – much stronger than our bones. They are covered in tooth enamel, the hard white shiny substance which gives great strength to the tooth (Figure 6.2).
What do you think is the purpose of tooth enamel and what does it enable us to do?
The enamel protects teeth from penetration by bacteria, so it prevents tooth decay. It also strengthens the teeth and stops them from wearing down, so we can bite off chunks of food and chew it to a soft mass throughout our lives.
There are various tooth shapes for different jobs. For example, when chewing, the upper teeth work together with the lower teeth of the same shape to bite, chew and tear food apart. According to their shape and function the adult teeth have got different names (Figure 6.3 and the bullet points below it).

- Incisors: there are eight incisors in the front of the mouth (four on the top and four on the bottom). They have sharp, chisel-shaped crowns that cut food.
- Cuspids: (or canine teeth): there are four cuspids, one next to each incisor. They have a pointed edge to tear food.
- Bicuspids (or premolars): the four pairs of bicuspids are located next to the cuspids. They crush and tear food.
- Molars: there are twelve molars, in sets of three, at the back of the mouth. They have wide surfaces that help to grind food.
6.1.3 Salivary glands
Glands are organs of the body which produce natural substances such as hormones and breast milk, and fluids that keep the body in fluid balance. Salivary glands are organs that produce saliva and release it into the mouth, particularly when we are hungry and when we are chewing food. There are three pairs of salivary glands; their names and locations are shown in Figure 6.4. Their names tell you where they are located: parotid means ‘beside the ear’, sublingual means ‘under the tongue’, and submandibular means ‘under the jaw’.

If the salivary glands don’t function properly due to disease or an injury, the amount of saliva produced decreases and the mouth becomes dry. This is unpleasant for the affected person, it makes chewing and swallowing food more difficult, and it increases the risk of tooth decay and gum disease. There may also be a bad smell from a dry mouth, because saliva naturally keeps the mouth clean by washing away bacteria and small particles of food.
6.1.4 Tongue
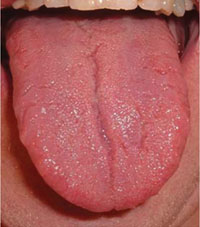
The tongue is a muscular organ which is important in enabling us to taste different types of food, roll chewed food into a ball for easy swallowing, and communicate with others through speech. A healthy tongue is pink and clean, with hundreds of tiny ‘taste buds’ visible on its surface (Figure 6.5).
6.2 Common oral diseases and their causes
Neglecting dental and oral hygiene, eating a high-fat high-sugar diet, chewing khat, smoking or chewing tobacco, and excessive alcohol consumption are the main causes of mouth, tooth and gum diseases. In this section, we describe the most common oral diseases, how you can identify them and what actions you should take.
6.2.1 Bacterial, viral and fungal infections in the mouth
As a health worker, you will know that inspecting the tongue of a person helps you to quickly assess whether he or she is healthy or not. In someone who is unhealthy, the tongue is often coated with a whitish or yellowish deposit that has a fur-like appearance. This may be caused by bacteria, viruses or a fungal infection (‘thrush’) growing on the tongue, which may be due to inadequate oral hygiene. You should also be aware that up to 50% of people who are HIV-positive have fungal, bacterial or viral infections in the mouth, which often occur early in the course of HIV infection. If you are involved in palliative care for someone who is terminally ill (see Study Session 3), you will notice that mouth infections such as thrush are very common as the person approaches closer to death.
Opportunistic infections in people living with HIV/AIDS are described in the Communicable Diseases Module, Part 3, Study Session 21.
Mouth infections may be treated by good oral hygiene (see Section 6.2.2) and by salt water mouth washes. Dissolve a large spoonful of salt in a cup of water which has been boiled and then allowed to cool. The patient should take a mouthful of the salt solution and hold it in his or her mouth for at least two minutes, using their tongue to move the solution around all parts of the mouth. Spit out the solution and repeat one or two more times. This should be carried out two or three times per day until the mouth remains clean.
Can you explain why infections in the mouth are common among people living with HIV/AIDS or in the later stages of a terminal illness?
The reason is because the immune system, which normally defends the mouth from infection, is no longer functioning adequately.
![]() A patient with HIV/AIDS or a terminal illness, whose immune system is not working adequately, may need medical treatment for infections in the mouth and should be referred.
A patient with HIV/AIDS or a terminal illness, whose immune system is not working adequately, may need medical treatment for infections in the mouth and should be referred.
6.2.2 Tooth decay
Bacteria constantly multiply in food particles in the mouth, particularly on the teeth and trapped between the teeth. When bacteria build up, they form a sticky, colourless substance called plaque (pronounced ‘plaak’), which is the main cause of tooth decay and gum disease. Bacteria produce acids that destroy tooth enamel, enabling the bacteria to penetrate into the internal structure of the tooth (look back at Figure 6.2) and cause decay. When plaque is not removed by brushing, it hardens into tartar (or calculus), which is very difficult to remove. The growing layer of tartar pushes the gums away from the tooth and in time it may become loose and fall out.
Certain foods contribute to plaque formation. A diet high in sugar and starch will eventually result in tooth decay. Today, in most parts of Ethiopia, sugar appears to play a key role in the increasing rates of tooth decay. Sugar cane, soft drinks, biscuits, candy, other sweets and refined sugars are readily available in every corner of the country, and the use of sugar as a sweetener in tea and coffee is now universal in both urban and rural Ethiopia. This is having a negative impact on the dental health of the population.
Using tobacco also increases the risk of developing gum disease. Smoking and chewing tobacco and khat contribute to plaque and tartar build up, as well as causing oral cancer (see Section 6.2.4).
6.2.3 Fluorosis
Fluoride is a substance found in nature that strengthens teeth and helps prevent tooth decay. Most water systems naturally contain some fluoride, but the amounts must be ‘just right’ to promote oral health. Not getting enough fluoride in the diet or water supply increases the risk of tooth decay. Many western countries either add it to tap water or advise people to use toothpastes containing fluoride. Communities in the highlands of Ethiopia have water supplies low in fluoride, so they are prone to faster rates of tooth decay than elsewhere.
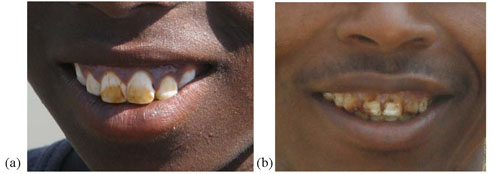
However, very high concentrations of fluoride are even more damaging to the teeth. Water sources in the Ethiopian Rift Valley have very high fluoride levels, causing dental fluorosis (yellowish discoloration of the teeth, (Figure 6.6a) in their populations. A high intake of fluoride during childhood, especially in the first six to seven years of life, leads to severe fluorisis later in life (Figure 6.6b). This is associated with cracking and ‘pitting’ (tiny holes in the surface) of the teeth, which create cavities for bacteria to grow and cause tooth decay. The teeth become very weak and can easily break.
6.2.4 Tooth abscesses, mouth ulcers and cold sores
Tooth pulp is the deepest part of the tooth structure, where nerves and blood vessels are found (look back at Figure 6.2). If it becomes diseased or injured and can't repair itself, the tooth dies and will soon fall out. The most common cause of pulp death is a cracked tooth or a deep cavity. Both of these problems can let bacteria enter the pulp and cause an infection inside the tooth. This infection can create a tooth abscess, which is a collection of pus trapped inside the root of the tooth, or in the tissue surrounding the root. Tooth abscesses are very painful and often produce swelling of the mouth in the affected area. The tooth may have to be removed to release the pus and allow the infected area to recover. The patient may also need antibiotic treatment.
Mouth ulcers are open sores in the mouth, where infection has penetrated the outer layer of tissue. The edge of an ulcer is often ‘rolled’ like a piece of injera. Salt water mouth washes may be enough to kill the infection in a mouth ulcer. Another common oral infection are cold sores – rapidly developing ‘scabs’ on the lips and around the edges of the mouth, caused by Herpes viruses (Figure 6.7).

6.2.5 Eroded or broken teeth
Cracked or broken teeth can be caused by personal habits such as biting pens or chewing hard items like khat, hard grains and nuts. Chewing khat wears down the teeth over many years. Elderly users of khat may have to grind the leaves and mix the green paste with water (Figure 6.8) because their teeth may have worn away completely after many years of chewing the tough leaves. Using your teeth as a heavy duty tool (e.g. for wire cutting or opening bottles) can damage the enamel and crack or break the tooth. This makes tooth decay more likely to occur.

6.2.6 Oral cancer
In Study Session 3 of this Module you studied the different types of cancers, with particular focus on cancers of the breast and female cervix. Oral cancer in the mouth is a less common cause of disability and death, which is often neglected because the signs and symptoms are not recognised, or are thought to be due to infection in the mouth. The signs are white and red patches inside the mouth or lips (Figure 6.9), swelling, blisters and ulcers, difficulty in swallowing, ear pain, loose teeth, and bleeding from the mouth. These signs should alert you to refer the person urgently to a higher health facility for specialist evaluation.

In most countries, the incidence of oral cancers is between one and ten new cases arising every year per 100,000 population. In the Ethiopian population of approximately 80 million people, how many new cases of oral cancer would you expect in a single year?
80 million divided by 100,000 = 8,000. So if there is only one new case per 100,000 population in Ethiopia, you would expect 8,000 new cases of oral cancer to develop in a single year. There would be ten times this number (80,000 cases) if the incidence rate was 10 new cases per 100,000 population.
Two known causes of oral cancer are tobacco and alcohol. Eighty to 90% of oral cancers come from smoking cigarettes, cigars or pipes, chewing tobacco or khat. The longer a person has used tobacco, the higher is their risk of developing cancers, including oral cancer, as well as lung and other cancers. People who use a pipe for smoking tobacco are especially prone to cancer of the lip. When a person stops using tobacco, they greatly reduce the risk of developing oral cancer. Strong alcoholic drinks (‘spirits’ like whisky and brandy) are damaging to the delicate membranes in the mouth, and prolonged use over several years increases the risk of developing oral cancers.
6.2.7 Cleft lip and cleft palate
Finally, we should mention birth defects such as cleft lip and palate (Figure 6.10). These conditions occur in around one per 500 to 700 of all births, but the rate varies substantially between different ethnic groups and in different countries. The clefts can be repaired surgically, but many affected children in poor communities are left without surgery.
A cleft lip may result in the child being stigmatised and rejected as it grows up. A cleft palate can allow infection to get into the brain through the gap in the roof of the mouth; this rapidly leads to death unless urgent medical attention is received.

6.3 How can the burden of oral diseases be reduced?
The burden of oral diseases and several other chronic non-communicable diseases can be reduced simultaneously by addressing common risk factors, such as tobacco use, harmful use of alcohol and an unhealthy diet. Therefore, the health education you should give to people in your community to promote oral health should be to:
- Reduce the intake of sugars and fats and eat a well-balanced diet, which is rich in fruits, vegetables, whole grains, peas and beans; raw vegetables and fruits also help to clean the teeth due to their high fibre content.
- Drink milk. It contains calcium to build strong teeth and bones.
- Eat fluoride-rich foods, such as fish, if they live in a low-fluoride area. Excess fluoride in water can be controlled by the authorities if water is treated to remove some of the fluoride; traditional low-cost methods include storing drinking water in clay pottery, which absorbs some of the fluoride.
- Don’t smoke or chew tobacco and don’t chew khat.
- Reduce alcohol consumption to small occasional amounts (if any).
- Promote oral hygiene.
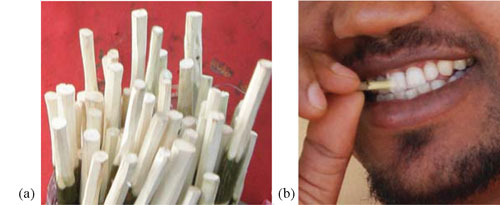
Oral hygiene is the practice of keeping the mouth clean and healthy by brushing the teeth, gums and tongue every day, and cleaning between the teeth using thread-like material (flossing) to prevent tooth decay and gum disease. Advise your community members, especially children, to brush their teeth for a minimum of two minutes at least twice a day and ideally after each meal. If modern toothbrushes are unavailable or are too expensive, use indigenous tooth sticks made from neem, woiyra or other trees (Figure 6.11).
In big towns, modern toothbrushes and toothpaste are available for cleaning the teeth, but they cost much more than traditional tooth sticks. You should advise your clients that if they buy a toothbrush, choose a soft bristled one and use fluoride toothpaste. Hold the toothbrush at a 45-degree angle at the gum line, brushing in a circular motion. This sweeps plaque from between the teeth.
People living with HIV/AIDS, diabetes or cancer should ask a dentist or doctor to check their oral cavity once or twice a year, because these conditions weaken the resistance of the body and infection in the mouth is very likely.
In the next two study sessions (the final sessions in Part 1 of this Module) you will learn about how to give life-supportive care to people with emergency conditions.
Summary of Study Session 6
In Study Session 6, you have learned that:
- Oral health is being free from pain and disease in the oral cavity; oral hygiene is the practice of keeping the mouth clean by brushing and flossing.
- The oral cavity is the entrance to the digestive and respiratory systems; it includes the teeth and other structures that aid chewing and speech, such as the lips, cheeks, tongue, hard and soft palate, and the salivary glands.
- Humans produce two sets of teeth in their lifetimes. The teeth are the strongest structures in the body; their surface is protected by a layer of hard enamel. The shapes of the four different types of teeth enable them to perform different functions during eating.
- Three pairs of salivary glands secrete saliva, which is a clear liquid produced to keep the mouth wet and clean, and to aid chewing and swallowing.
- Sticky bacterial growth around the teeth is called plaque. It destroys the enamel by producing acids which allow decay to penetrate the teeth. If plaque is not removed, it hardens into tartar, which causes the gums to pull away from the teeth. Plaque, tartar and gum disease increase the risk of tooth loss.
- Dental fluorosis is caused by long-term high intake of fluoride in the water supply beginning in childhood; severe fluorosis leads to cracking of the teeth and tooth decay.
- Other common causes of oral diseases are tooth abscesses, mouth ulcers and cold sores, worn and eroded teeth, and oral cancers.
- Babies may be born with a cleft lip or cleft palate, which should be repaired surgically.
- Common causes of oral diseases are a high-sugar high-fat diet, use of tobacco, khat and alcohol, using the teeth as a tool, and poor oral hygiene.
- Oral health can be promoted through eating a healthy diet, drinking milk to build strong teeth and bones, avoiding harmful substances like tobacco, khat and alcohol, good oral hygiene, and protecting the teeth from damage and decay.
- Regular tooth brushing and cleaning between the teeth (flossing) should be taught to children and adults in your community.
Self -Assessment Questions (SAQs) for Study Session 6
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 6.1 (Learning Outcomes 6.1 and 6.2)
Which of the following statement is false? In each case, explain why it is incorrect.
A The structures of the oral cavity enable us to speak, chew and swallow.
B Humans normally produce two sets of 32 teeth.
C The mouth is the entrance to the digestive and respiratory systems.
D The palate is the floor of the oral cavity.
E Saliva helps to keep the mouth clean.
F Teeth are dead structures made from enamel and bone.
Answer
A is true. The structures of the oral cavity enable us to speak, chew and swallow.
B is false. Humans do normally produce two sets, but only the second (permanent) set has 32 teeth. The first set (milk or baby teeth) has only 20 teeth.
C is true. The mouth is the entrance to the digestive and respiratory systems.
D is false. The palate is the roof of the oral cavity (not the floor).
E is true. Saliva helps to keep the mouth clean.
F is false. Teeth are living structures with dentine, pulp and blood vessels inside them; only the upper surface of a tooth is covered with hard dead enamel.
SAQ 6.2 (tests Learning Outcomes 6.1, 6.3 and 6.4)
- a.What is plaque and what conditions promote its formation on our teeth?
- b.What are the consequences of plaque forming on the teeth?
- c.What can be done to prevent it?
Answer
- a.Plaque is a sticky bacterial growth around the teeth. The conditions that promote its formation are high-sugar high-fat diets and poor oral hygiene.
- b.Plaque destroys the tooth enamel by producing acids which allow decay to penetrate the teeth. If plaque is not removed, it hardens into tartar, which causes the gums to pull away from the teeth. Plaque, tartar and gum disease increase the risk of tooth loss through decay.
- c.Reducing the amount of sugars and fats in the diet, and increasing the amount of fruits and vegetables, helps to reduce the development of plaque. Regular brushing and flossing of the teeth also removes plaque and promotes oral health.
SAQ 6.3 (tests Learning Outcomes 6.1 and 6.3)
Habtamu was born and grew up in the Rift Valley in Ethiopia. He is now ten years old and his teeth are yellowish in colour. His friends say he has natural ‘gold’ teeth, but most of them also have yellow or brown patches on their teeth.
- a.Why are Habtamu’s teeth yellow? What is this condition called?
- b.What problems could result from it in the future?
Answer
- a.Habtamu probably has yellow teeth because he has been drinking water containing a high concentration of fluorides all his life. His friends also have yellow teeth. This condition is called fluorosis.
- b.Fluorosis leads to weakening of the teeth, which are likely to develop ‘pits’ (holes) and cracks where decay can get in. Habtamu will probably suffer from a lot of tooth decay, and broken or lost teeth.
SAQ 6.4 (tests Learning Outcomes 6.1, 6.2 and 6.4)
Imagine that you are invited to talk about promoting oral health in a primary school in your village. After the lesson, you ask the students to make a poster with the most important messages about oral health. What messages would you expect to see on the poster made by the children?
Answer
The messages you would expect to see on the school poster should include:
- Brush your teeth for two minutes at least twice a day, especially after meals.
- Use traditional tooth sticks or a soft bristle toothbrush and toothpaste.
- Avoid sugary foods and drinks.
- Eat a healthy diet rich in fruits and vegetables.
- Drink milk. It contains calcium to build strong teeth and bones.
- When you grow up, don’t smoke or chew tobacco, or chew khat, or drink alcohol.