Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Tuesday, 21 July 2026, 9:40 PM
Nutrition Module: 11. Nutrition Education and Counselling
Study Session 11 Nutrition Education and Counselling
Introduction
In the previous study sessions you learned about optimal infant and young child feeding, macro and micronutrient deficiencies of public health importance in Ethiopia, and nutritional requirements throughout the life cycle. In this study session you will be introduced in more detail to the different ways you can help people to improve their own nutrition and that of their family.
You will learn about behaviour change communication and essential nutrition actions, as well as useful ways of communicating information about these actions to people in your community. You will also learn about growth monitoring and the triple A cycle, which is a way of making sure that you can pass on your knowledge effectively to the people you are responsible for. You will also learn ways of counselling mothers on child feeding.
Learning Outcomes for Study Session 11
When you have studied this session, you should be able to:
11.1 Define and use correctly all of the key words printed in bold. (SAQs 1.1, 11.2 and 11.7)
11.2 Describe the differences between nutrition education and nutrition behaviour change communication (BCC). (SAQs 11.1, 11.2 and 11.7)
11.3 Identify the steps of behaviour change communication. (SAQs 11.1, 11.2, 11.3 and 11.4)
11.4 Explain the essential nutrition actions used in BCC. (SAQ 11.3)
11.5 List the critical health contact points for nutrition BCC. (SAQ 11.4)
11.6 Identify non-health contact points for nutrition BCC. (SAQs 11.5, 11.6 and 11.8)
11.7 List the GALIDRA steps in delivering nutrition counselling. (SAQ 11.6)
11.8 Explain the critical focus area of nutrition BCC in Ethiopia. (SAQ 11.9)
11.1 Behaviour change communication
In your practice as a Health Extension Practitioner, there are different communication strategies you can use to help the people in your community to be responsible for their health. Systematic behaviour change approaches are a really important way of improving the nutritional status of the women and young children who are under your care. Behaviour change communication (BCC) strategies are aimed at influencing the actions of families and communities. In addition to considering individual health beliefs and practices, BCC can promote nutritional improvements and address local traditions and household dynamics (conditions). Audiences are carefully segmented (grouped), and communications can be made using mass media and through community leaders and elders to achieve defined behavioural objectives.
Segmentation refers to targeting key messages to the relevant audience at the relevant time. This helps prevent information overload for people, by ensuring they are not given unnecessary information. For instance, during pregnancy, it is better to focus on maternal nutrition and breastfeeding rather than talking to the mother and family about complementary feeding, which can be discussed at a later stage.
What is message segmentation and why it is important?
Segmentation refers to targeting key messages to the relevant audience at the right time. It’s a way of ensuring that people get the information that is most relevant to them when they need it.
11.2 Stages of behaviour change
One of your tasks as a Health Extension Practitioner is to identify where change in a person’s behaviour or habits could help to have a positive impact on their health or the health of their baby. For example, helping a person eat a more balanced and healthy diet.
Behaviour change communication is more than just education, it aims to change behaviour and practice.
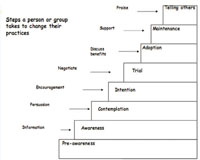
There are eight stages in behaviour change that will help the people you are working with change from being an uninformed person to becoming someone who may even be able to teach or influence others about their behaviour. You are going to learn about this now, using exclusive breastfeeding behaviour as an example to illustrate the key points.
Step 1 Pre-awareness At this stage people are not even aware of the changes that they need to make. In order to help them become a person who has awareness, you need to give them information. Nutrition education would stop at this stage without making sure that the person being educated has changed their action, practice or behaviour. Before this stage the mother does not know about the importance of exclusive breastfeeding during the first six months.
Stage 2 Awareness At this stage, the person has heard about the need to change their behaviour, but needs extra help and persuasion to start to actually bring about the changes. At this stage the mother is aware about the need for exclusive breastfeeding during the first six months, but has not thought of doing it for her baby.
Stage 3 Contemplation This person is contemplating (thinking) about changing their behaviour, but needs more information and continued support and persuasion about the advantages and disadvantages of changing their behaviour. At this stage more information about the benefits of exclusive breastfeeding compared to other forms of feeding is needed, as well as support that shows you understand the mother’s situation.
Stage 4 Intention At this stage the person has understood the advantages and disadvantages of changing their behaviour but is not sure how they can bring about the new behaviour for themselves. The person needs encouragement to overcome obstacles of how to do the new behaviour. For example, the mother may be worried about not being able to maintain exclusive breastfeeding when she is away for work, or for other individual or personal reasons. In this situation you could show her how she can express breastmilk so the baby can be fed when she is away.
Stage 5 Trial The person has tried the behaviour or action required, but has faced difficulties. For instance, the mother tried to exclusively breastfeed her baby, but she faced some difficulties. She now needs support in the form of praise and reinforcement of the benefits. Reinforcing the ways of preventing the problem she faced during exclusive breastfeeding is also important. So she needs counselling to find the best ways of overcoming her problems. At this stage the mother may have inadequate breast milk output and think that her breast milk is not enough for the baby to feed on until six months old. Here, she needs to be assisted on proper positioning and attachment and be reassured about the capacity of the breastmilk to feed the baby for the first six months. Your skills in negotiating the different options the mother can use will be important at this stage.
Nutrition behaviour change communication is different from nutrition education in that BCC needs at least three contacts to change behaviour. Unlike nutrition education, which aims at increasing awareness or knowledge, BCC targets change of behaviour or practice. For example, if at this point the mother has not tried exclusive breastfeeding, there needs to be at least three contacts between you and the mother to change her behaviour and to help her progress from the awareness stage to the trial stage.
Behaviour change communication (BCC) is an ongoing process that requires effective communication to persuade, encourage and support change.
Stage 6 Adoption At this stage, the person is demonstrating the new behaviour. They now need discussion to reinforce their behaviour and sustain the change they have made. For example, the mother has now sustained exclusive breastfeeding. What she needs at this stage is further discussion on the benefits of exclusive feeding to reinforce the behaviour and make sure that she continues exclusive breastfeeding for a few weeks. You can help her with this, by encouraging and praising her and emphasising the importance of exclusive breastfeeding for her baby’s health.
Stage 7 Maintenance The person’s behaviour by this stage has changed and they understand the benefits of the change. Now they just need support if they face any difficulties. For example, the mother has changed her behaviour and is now used to exclusive breastfeeding and has understood its benefits. It has become part of her behaviour and she thinks that she will exclusively breastfeed when she has another baby. What she needs at this stage is support in overcoming any further difficulties.
Stage 8 Telling others The person has done the behaviour for a considerable length of time, it has become routine behaviour and now leads to the person convincing others about the benefits of their health related behaviour. For example, the mother is encouraging other mothers to exclusively breastfeed their babies and describing the benefits to the baby and mother. What the mother needs at this stage is praise.
Why is knowledge not enough to change behaviour, action or practice?
You have learned that knowledge alone only provides information. The BCC model indicates that you can only promote effective and sustained changes in the way a person does something if you have at least three contacts with a person, and spend time persuading, encouraging and supporting a person to change. This reinforces their behaviour and is more likely to lead to lasting change.
Figure 11.1 summarises the eight steps to behaviour change.
You are now going to look at how you can use the BCC steps and apply these to a communication strategy to help improve nutrition in your community.
11.3 Nutrition behaviour change communication
Nutrition behaviour change communication is a strategy that you will be able to use to change nutrition related behaviours in your community. Using the techniques and approaches described in this study session you will be able to bring about practices that promote better health through optimal feeding practices and improved dietary habits. You will be able to use behaviour change communication (BCC) to teach people about essential nutrition actions, most particularly optimal infant and young child feeding practices and the key messages in relation to these, and also to facilitate the adoption of healthy adult dietary styles.
The BCC activity in your community will involve you educating the community about a wide range of activities including horticultural activities, development of backyard fruit and vegetable gardens, and use of irrigation and water harvesting systems. For such activities you will need to gain collaboration from the frontline agricultural workers in your community, as together you will have a greater impact. Table 11.1 summarises some of the actions you will probably need to do to facilitate the progress of behaviour change at each stage.
Of course the methods you are able to use in your work will depend on your own situation. As you read through the table you should think about the ways that you can bring about these stages of change in your own practice as a Health Extension Practitioner.
| Stage of behaviour change | Action needed | Communication strategies |
|---|---|---|
| 1. Pre-aware (never having heard about the behaviour) | Build awareness and provide information | Drama, songs Community groups Radio Individual counselling Young child feeding support groups |
| 2. Aware (having heard about the new behaviour and knowing what it is) | Give more information, discuss benefits and persuade | Group discussions or talks Oral and printed word Counselling cards Feeding support groups |
| 3 and 4. Contemplation and intention (thinking about new behaviour) | Persuasion and encouragement | Group discussions or talks Individual counselling Counselling cards Feeding support groups |
| 5. Trial (trying new behaviour out) | Negotiate the best ways of overcoming obstacles | Home visits Use of visuals aids Groups of activities for family and the community Negotiate with the husband and mother-in-law (or influential family members) to support |
| 6. Adoption (demonstrating the new behaviour) | Further discussion on the benefits to ensure the behaviour continues | Encouraging and praising Emphasising the importance of the behaviour |
| 7. Maintenance (continuing to do new behaviour or maintaining it) | Discuss benefits, provide support at all levels | Congratulate mother and other family members as appropriate Suggest support groups to visit or join to provide encouragement Encourage community members to provide support |
| 8. Telling others | Praise and reinforce the benefits and give support | Reinforce the benefits Praise |
Nutrition BCC can be done with individuals or with groups or communities. To facilitate the progress of a person through each stage of behaviour change you can use the different actions and communication strategies that are summarised in Table 11.1. These are just possible examples however, and are by no means an exhaustive list of all the possible strategies. As a communicator, you will also be able to improvise (or adapt strategies) using locally available resources in your own community’s context. The following activity will help you think how to put these stages into practice in different scenarios.
Activity 11.1 Behaviour change
Read the following case studies and then answer the two questions that follow.
Case 1 A woman has heard the new breastfeeding information, and her husband and mother-in-law are also talking about it. She is thinking about trying exclusive breastfeeding because she thinks it will be best for her child.
Case 2 A woman has brought her eight-month-old child to the baby weighing session. The child has lost weight and the mother asks the health worker for advice.
Case 3 In the past month a health worker talked with a mother about gradually starting to feed her seven-month-old baby three times a day instead of just once a day. The mother started to give a meal and a snack and then added a third feed.
Questions
- a.What stage in the behaviour change model do you think each person has reached?
- b.What could the health worker do to help each of the women?
Answer
Case 1 The mother here is at the contemplation and intention stages. She is thinking about changing her behaviour. So the health worker can give her information and support (Stage 3). The mother has understood the benefits of exclusive breastfeeding but may not be sure how to do this. For example, she may be away for work and needs encouragement to overcome the obstacles to exclusive breastfeeding that this creates (Stage 4).
Case 2 In this case the mother does not know the cause of her child’s weight loss and the health worker will need to explain that there could be a feeding problem. The mother is at Stage 1 (pre-awareness) and the health worker can provide the mother with information about an appropriate diet for her child and persuade (Stage 2) the mother of the advantages of the proposed diet for her child.
Case 3 In the third case the mother has implemented what the health worker told her at earlier visits and she has started feeding her child differently. This indicates that she is in the trial stage and moving towards adoption (Stage 5). The health worker can support the mother by providing additional encouragement and praising her.
11.3.1 The focus of community-based nutrition behaviour change communication
The focus of community-based nutrition (CBN) behaviour change communication in Ethiopia and throughout Africa is to facilitate feeding and dietary behaviours that are compatible with growth, development, long-term health, survival and productivity. Therefore your work will involve:
- Promotion of essential nutrition actions
- Promotion of food-based approaches to enhance the production and consumption of a wide range of nutritious foods.
A balanced and healthy diet is the key outcome.
The essential nutrition actions
Major emphasis is given to essential nutrition actions (ENA) in all national nutrition-related policies, strategies, programmes and guidelines including the National Nutrition Strategy (NNS), the National Nutrition Programme (NNP) and the National guidelines for control and prevention of micronutrient deficiencies. Table 11.2 summarises the seven ENAs and the key messages you will need to communicate to the target audiences in your community such as parents of young children. Take some time now to read the information set out in the table.
Table 11.2 Seven essential nutrition actions (ENA) and key messages. (Source: Linkages project/AED Ethiopia, 2005, Behavioural change communication manual)


11.3.2 Integrating the seven ENAs into the six health contacts
You will have six health contacts with mothers and children in your community. Nutrition behaviour change communication and promoting the seven essential nutrition actions will be an important element within these six health contacts. Table 11.3 overleaf outlines what the six health contacts are, and the key nutrition action messages you need to communicate at each contact.
Table 11.3 Delivery of the key essential nutrition action messages. (Source: Linkages project/AED Ethiopia, 2005, Behavioural change communication manual)

When does breastfeeding appear as a key message within the seven ENAs a key message and why is it so important?
Breast feeding is included in four of the key messages, namely optimal breastfeeding, optimal complementary feeding, sick child feeding and control of vitamin A deficiency. You know from this and earlier study sessions that breastfeeding is critical for promoting healthy growth in infants, helping prevent disease and encourage bonding between the mother and baby.
Nutrition BCC on ENA components can also be given as part of other health programme contacts including child survival interventions (such as community IMNCI and community nutrition programmes), national immunization days and other infectious diseases control programmes.
11.3.3 Integrating the seven ENAs into other sectors
Nutrition improvement for the people you are responsible for cannot be addressed by any one sector alone; it needs to be integrated with frontline workers in other sectors. You will therefore need to communicate with the different frontline workers in sectors such as education and agriculture. Table 11.4 summarises the ENAs that could be integrated to sectors outside health.
| Other non-health contacts | Key essential nutrition action aspects the BCC should focus on |
|---|---|
| School | School lunch programme De-worming Adolescent nutrition Iron and folic acid supplementation Iodised salt consumption by the family Use of insecticide-treated bed nets Tetanus toxoid (TT) vaccination |
| Community nutrition | De-worming Adolescent nutrition Maternal nutrition Community growth monitoring and promotion Maternal nutrition during pregnancy and lactation |
| Emergency | General ration distribution Outpatient therapeutic programme (OTP) Therapeutic feeding programme (TFP) Targeted supplementary feeding and blanket supplementary feeding programmes Caring practices (optimal breastfeeding and optimal complementary feeding, preventive and promotive health seeking) Exemption of pregnant women and lactating mothers with a child under six months old from the public work requirement in the food-for-work programme (unconditional transfer) |
| Agriculture | Food diversification Food security |
| Water and sanitation | Building water points saves maternal workload and energy expenditure and gives more time for caring practices |
| Informal community gatherings (market days, ‘Debo’, ‘Edir’, ‘Equb’, Coffee Ceremony ‘Mahiber’, ‘senbete’) | Using these gatherings to do ENA BCC Consumption of at least one additional meal per day Iron and folic acid supplementation Iodised salt consumption by the family Optimal infant feeding Infant feeding options if the mother is HIV-positive Use of impregnated bed nets De-worming in the third trimester TT vaccination Regular antenatal visits |
How might you be able to work with other sectors in your own community or work situation to improve the nutritional status of people living in your community?
Working with agricultural development workers or school teachers within your community will be an important part of your role. Working collaboratively will help to ensure the essential nutrition actions are shared as widely as possible and help to build understanding of their importance.
11.4 Nutrition behaviour change communication in food-based approaches
It is not possible to address nutritional problems in a sustainable way through supplementation in the form of tablets or capsules. It would be too difficult to organise and the costs would be too high. Therefore, promotion of food-based approaches are important for you to use within your own community. Horticultural activities and dietary diversification are both examples of important approaches, as you saw in Study Session 7, so BCC should focus on the need for consumption of different varieties of foods. The intensification of horticultural activities needs to be supported by nutrition education and one of the things you can do as Health Extension Practitioner is to provide practical demonstrations for people in your community and encourage women to cultivate vegetable gardens as a source of nutritious food for their families (see Figure 11.2).
In addition, BCC should focus on the importance of knowledgeable care for pregnant and lactating women, and for children during the first two years of life. This should give greater emphasis on changing behaviours in relation to:
- Cultural malpractice and beliefs in child feeding and weaning (complementary feeding process, exposure of children to sunlight, addressing issues relating to food faddism and food prejudices)
- Intra household mal-distribution of food (e.g. age bias, sex bias)
- Emotional deprivation and neglect of the child.
As Health Extension Practitioner you can help bring about positive dietary behaviour through effective nutrition BCC in your community.
11.5 Growth monitoring and promotion
Growth monitoring is a critical entry point for you for counselling the mother or the caregiver about the child’s nutrition.
Growth monitoring refers to the regular assessment of the growth of children under two years old to detect deviation from normal growth and the application of appropriate interventions. During community-based nutrition (CBN) programmes you will have the opportunity to weigh children under two years old every month, and plot their weight on the chart. In the following section you will learn how you can counsel mothers and caregivers about the growth and nutritional status of their children.
11.5.1 Objectives of growth monitoring
Growth monitoring and promotion have the following objectives:
- To measure individual health and to instigate effective action in response to growth faltering (slowing down)
- Teach mothers, families and health workers how diet and illness can affect child growth and thereby stimulate individual initiative and improved nutrition and healthcare practices
- To provide regular contact with primary health services.
Poor linear growth (underweight and stunting) usually occurs in the first 24 months of life. If the child is not optimally fed during this time, they could lose 11cm from the potential height that they would have reached as an adult. Once stunting has happened, it is very difficult to catch up. By the time a child is two or three years old, catch-up growth is less likely to occur; such children have probably failed to grow and are potentially stunted for the rest of their lives. You learned how to assess whether a child is stunted in Study Session 4 of this Module.
Table 11.5 outlines the main reasons for malnutrition in children during their first five years.
| Age of malnourished child | Determinant factors |
|---|---|
| Birth | Maternal factors (including nutrition), gestational age |
| Four-six months | Infant feeding practices, maternal ability to care for the child |
| Six months to two years | Complementary feeding practices, exposure to infections, disease and poor household food as the child gets older |
| Two-five years | Inadequate access to household food; infections and social deprivation |
In Ethiopia we use underweight for monitoring growth, as it indicates acute changes in the nutritional status of the child. If you determine that the child is malnourished (underweight), you should be able to analyse the causes, identify resources, suggest alternative solutions and arrive at decisions together with the mother or caregiver as to what should be done about the child. This process of assessment analysis and action is known as the ‘triple A’ cycle which is described below.
11.5.2 The ‘Triple A’ cycle approach
Growth monitoring can be undertaken using a cyclic process called Triple A cycle. As the term indicates, there are three stages to the process.
Assess
This stage involves weighing a child on a regular basis, and comparing the child’s growth with the standard and with their previous weight. The measurements will determine the rate of the growth of the child. This helps to identify any nutritional problems and will help you reflect on and review the child’s situation with the mother or caregiver.
Analyse
This requires exploration of any nutritional problem of the child in order to understand the root causes of any difficulties. You should identify gaps in feeding or care practices and think about different alternative solutions and resources that you can suggest to the mother or caregiver.
Action
This stage involves counselling the mother or caregiver about relevant actions. It involves decision making and resource identification as well as deciding on individual and collective doable actions. After thorough discussion with the mother or caregiver, you should be able to decide on the specific actions they need to do. Ideally these actions are feasible and can realistically be done by the caregiver and the household. Each time the child is weighed again, re-assessment is done, followed by new analysis and new action as necessary.
Figure 11.2 illustrates the triple A cycle.
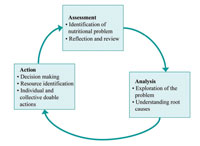
The triple A cycle measures the direction of the child’s growth.
The most important issue in growth monitoring is not the position of the child on the growth curve at one particular time, but the direction of his or her growth. Look at Figure 11.3 overleaf. A single point on the line of growth could be reached from different directions (that is, the child’s weight could go down to the single point or could move up to that point on the chart). Normally the child’s measurements are expected to fall between the lines indicated on the graph by -2 and +2 Z-scores (see the right hand side of the graph). The zero (or ‘0’) score represents the standard average measurement.
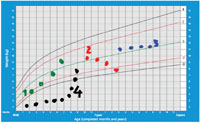
Figure 11.3 plots the direction of growth of four children. It gives you information you need to be able to advise the mother and caregiver what they need to do for their child.
- The child with the green plotted line is growing normally; you should encourage the mother to continue her feeding the way she has been doing it.
- The child with the red plotted line is decreasing weight. There must be something wrong with the feeding. You need to counsel the mother about the optimal feeding practices.
- The child with the blue plotted line is not growing, indicating that there is some problem with its feeding. You need to find out the problem together with the mother or caregiver and counsel them on what to do.
- The child with black plotted line is on catch-up growth (fast growth) after a period of malnutrition. So you should encourage the mother to continue feeding the child in the way she has been doing.
Why are serial (repeated) measurements in growth monitoring needed?
You need to do repeat measurements to check the rate and direction of growth of the child. Knowing the rate and direction of growth will help you when you are counselling the mother or caregiver.
11.6 Counselling mothers and caregivers on child nutrition
In your work, you will have many possibilities for helping parents improve the nutritional status of their children. You should always employ nutrition counselling as a tool to help you achieve this objective. Nutrition counselling is a process of finding the solution to the child’s nutritional problem together with their mother or caregiver. Unlike nutrition education, nutrition counselling is a two-way process during which the mother is actively involved in describing the child’s problems as well as participating in analysing the causes and identifying the available resources and solutions.
Working together in this way with the mother or caregiver will help them reach a decision about the doable actions. Analysing causes and identifying actions are an important part of the overall process. Once you weigh the child and determine their nutritional status you need to share this information with the mother and negotiate with her what actions she can take. Follow-up is also very important and you should always recommend to the mother that she makes an appointment so you can see whether she has carried the agreed actions or whether she has had some problems with these. This action or counselling stage completes the triple A cycle approach.
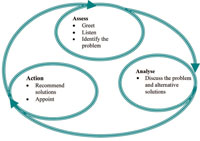
Counselling is an important skill, and as you have seen, a key element of the triple A cycle. The GALIDRA steps outlined in Box 11.1 will help you to counsel mothers and caregivers effectively.
Box 11.1 GALIDRA steps
The diagram below illustrates how the GALIDRA steps fit into the triple A cycle.

Counselling using GALIDRA steps is an individually focused BCC strategy that enables you to bring about positive behavioural change. As you can see in Figure 11.4, the process involves you having repeated contact with a mother or caregiver to make sure that they get to the trial and adoption stages of behaviour change that you looked at in section 11.2 of this study session.
Summary of Study Session 11
In Study Session 11 you have learned that:
- Nutrition education aims at increasing awareness or knowledge. Knowledge is not sufficient because at least three contacts are needed to change behaviour or practice.
- Nutrition behaviour change communication (BCC) is different from nutrition education as it aims to change behaviour or practice.
- The focus of nutrition BCC is on the seven components of essential nutrition actions and their key messages. These messages are communicated at the six health contacts and through other contacts outside the health sector.
- The second focus of nutrition BCC is food-based approaches, which includes the promotion of diversified production and diversified consumption of plant source and animal source foods.
- Growth monitoring and promotion (GMP) is done for children in Ethiopia who are under two years old. The serial measurements in GMP are required for detecting the rate and direction of growth of the child so that appropriate intervention can be planned and delivered.
- GALIDRA steps are used for delivering nutrition counselling and negotiation about child feeding with the mothers or caregivers.
Self-Assessment Questions (SAQs) for Study Session 11
Now that you have completed the study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers on your study diary and discuss them with your Tutor at the next study support meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of the module.
SAQ 11.1 (tests Learning Outcomes 11.1, 11.2 and 11.3)
- a.Write a list explaining the differences between nutrition education and nutrition behaviour change communication (BCC).
- b.Why is BCC important?
Answer
- a.Nutrition behaviour change communication (BCC) is different from nutrition education in that BCC needs at least three contacts to change behaviour. Unlike nutrition education, which aims at increasing awareness or knowledge, BCC targets change of behaviour or practice.
- b.BCC is important because it can influence and lead to lasting change in an individual's behaviour and practice. There are several stages a person is likely to go through, from a stage of pre-awareness, where they are not even aware of the change they need to make (for example, not knowing about the importance of exclusive breastfeeding, through the intention to make the change, but uncertain how to do this and therefore needing encouragement) through to adopting and maintaining the new behaviour (exclusive breastfeeding) and becoming an advocate of the practice to others in the community. BCC is therefore more than just education; it is about promoting sustained changes in the way a person does something.
SAQ 11.2 (tests Learning Outcomes 11.1, 11.2 and 11.3)
Match the correct stage of behaviour change with the actions needed to facilitate the change to the next stage.
Two lists follow, match one item from the first with one item from the second. Each item can only be matched once. There are 6 items in each list.
Build awareness/provide information
Persuade/give more information
Encourage/discuss benefits
Negotiate and help to overcome obstacles
Discuss benefits and provide support at all levels
Praise/reinforce the benefits
Match each of the previous list items with an item from the following list:
a.Aware
b.Telling others
c.Trial
d.Maintenance
e.Pre-aware
f.Contemplation/intention
- 1 = e,
- 2 = a,
- 3 = f,
- 4 = c,
- 5 = d,
- 6 = b
SAQ 11.3 (tests Learning Outcomes 11.3 and 11.4)
Explain the key messages of essential nutrition actions to be used in the BCC for preventing vitamin A deficiency.
Answer
In order to help prevent vitamin A deficiency there are a number of important messages to give your community:
- The importance of breastfeeding
- The need for vitamin A supplementation
- Consumption of vitamin A-rich foods (dark green leafy vegetables, yellow and orange fruits and vegetables) is part of a healthy and balanced diet.
SAQ 11.4 (tests Learning Outcomes 11.3 and 11.5)
Why are the critical health contact points for nutrition BCC important? Think of two or more reasons.
Answer
The critical health contact points are important for nutrition BCC for the following reasons:
- They can be used as an opportunity to educate mothers /care givers about nutrition
- Mothers are likely to implement the suggested actions or when you do a home visit.
SAQ 11.5 (tests Learning Outcome 11.6)
What non-health contact points with the mothers could be used for nutrition BCC?
Answer
Other non-health contacts, including with schools, emergency services, agricultural activities, and water and sanitation programmes can also be used as contacts to pass on nutrition messages. You can play an important role in working with other professionals in your community to promote key messages about nutrition.
SAQ 11.6 (tests Learning Outcomes 11.6 and 11.7)
- a.What are the steps in delivering nutrition counselling?
- b.Why is nutrition counselling important?
Answer
- a.The steps in delivering nutrition counselling are abbreviated as GALIDRA: greeting, asking the mother what her problem is, listening to what she is saying, identifying the causes of her problem and potential resources, discussing the alternative solutions with the mother, recommending the best alternative and appointing the mother
- b.Nutrition counselling is important because it is an individual BCC strategy that gives you an opportunity to involve the mother or any individual in the community in seeking a solution to his or her problem. Because it follows a triple A cycle, it has high potential in bringing about behavioural change.
SAQ 11.7 (tests Learning Outcomes 11.1 and 11.2)
What is the triple A cycle and when might you use it?
Answer
The triple A cycle is a process of assessment of the nutrition situation of vulnerable segments of the population, analysis of the possible causes of the problems and possible solutions, and action based on the evidences obtained from the analyses and reassessment. The triple A cycle is used in many activities related to nutrition, such as growth monitoring and maternal counselling on child feeding and nutritional surveillance.
SAQ 11.8 (tests Learning Outcome 11.6)
What informal community gatherings can be used for ENA BCC?
Answer
Different informal community gatherings can be used as an opportunity for passing the key messages of the essential nutrition actions. For example: market days, ‘Debo’, ‘Edir’, ‘Equb’, Coffee Ceremonies ‘Mahiber’ and ‘senbete’.
SAQ 11.9 (tests Learning Outcome 11.8)
What are the critical focuses of the nutrition BCC in Ethiopia?
Answer
The following are important focus areas for nutrition BCC in Ethiopia:
- Promotion of ENAs.
- Promotion of food-based approaches to enhance the production and consumption of a wide range of nutritious foods.
A balanced and healthy diet is the key outcome.