Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Tuesday, 21 July 2026, 9:28 PM
Postnatal Care Module: 5. Routine Postnatal Care for the Mother
Study Session 5 Routine Postnatal Care for the Mother
Introduction
Postnatal care (PNC) for the mother should respond to her special needs, starting within an hour after the delivery of the placenta and extending through the following six weeks. The care includes the prevention, early detection and treatment of complications, and the provision of counselling on breastfeeding, birth spacing, immunization and maternal nutrition. To standardise the PNC service, you are advised to use the screening, counselling and postnatal care cards. These cards ensure that you have covered all the essential steps in every home visit.
In this study session we are going to focus primarily on the routine checks you need to do to make sure the mother is recovering well after the birth, both physically and emotionally. We will also advise you on how you should counsel her on taking care of her health and recovery, maintaining her personal hygiene to reduce the risk of infection, and what she should eat – especially if she is breastfeeding.
Learning Outcomes for Study Session 5
When you have studied this session, you should be able to:
5.1 Define and use correctly all of the key words printed in bold. (SAQs 5.1 and 5.2)
5.2 Describe the physical checks you should do on the postnatal mother soon after the birth, and at subsequent postnatal visits, to ensure that she is recovering well. (SAQ 5.2)
5.3 Explain how you would counsel the mother on good nutrition in the postnatal period and what micronutrient supplementation you would give her. (SAQ 5.2)
5.4 Describe the types of support for the postnatal mother that you would encourage her partner and other family members to give her, including seeking care promptly if they detect possible danger signs. (SAQ 5.2)
5.1 Routine core postnatal care for the mother
The routine care provided to the mother during the postnatal period is mainly preventive measures targeted towards the early detection of the common causes of maternal morbidity and mortality in rural communities. During every postnatal visit, you should do the following routine activity, even when the mother does not complain of anything.
5.1.1 Check the mother’s vital signs
You learned how to check vital signs in Study Session 9 of the Antenatal Care Module.
Check the mother’s vital signs, i.e. her temperature, pulse rate, and blood pressure, and make sure they are within the normal range. Straight after the birth, check her pulse and blood pressure at least once every hour, and her temperature at least once in the first six hours.
What should the normal vital signs be if the mother is recovering well from the birth?
Her temperature should be close to 37oC; her pulse rate should be between 60 to 80 beats per minute when she is resting quietly; her systolic blood pressure (the top number, which measures the pressure when her heart contracts) should be 90-135 mmHg, while her diastolic blood pressure (the bottom number, which measures the pressure when her heart relaxes) should be 60 to 85 mmHg.
![]() Refer a woman urgently who is showing signs of shock and/or postpartum haemorrhage.
Refer a woman urgently who is showing signs of shock and/or postpartum haemorrhage.
If her blood pressure is too low and falling, and her pulse rate is too fast and rising, she is going into shock. The most likely cause is a life-threatening haemorrhage. If there are no signs of bleeding from the vagina, she may be losing blood internally.
5.1.2 Check if her uterus is contracting normally
Palpate (feel) her abdomen to check contraction of the uterus to make sure it is firm. Immediately after the birth, you should be able to feel it contracting near the mother’s umbilicus (belly button), and it gradually moves lower in her pelvis over the next two weeks. Check her uterus every 15 minutes for the first two hours after birth and every 30 minutes for the third hour. If possible, check every hour for the following three hours. If the uterus is hard, leave it alone between checks. If it feels soft, rub the abdomen at the top of the uterus to help it to contract. Teach the mother to do this for herself (Figure 5.1).

The drugs you gave the mother to help expel the placenta and prevent bleeding (e.g. misoprostol or oxytocin) will also help the uterus to contract. So will breastfeeding her baby. The mother may also need to urinate if her bladder is full, because this can prevent the uterus from contracting properly. Check the contraction of her uterus at every postnatal visit.
5.1.3 Clean the mother’s belly, genitals and legs

Help the mother clean herself after the birth. Change any dirty bedding and wash blood off her body. Always wash your own hands first and put on surgical gloves before you touch the mother’s genitals, just as you did before the birth. This will protect her from any bacteria that may be on your hands. Clean the mother’s genitals very gently, using soap and very clean water and a clean cloth (Figure 5.2). Do not use alcohol or any other disinfectant that might irritate her delicate tissues. Wash downward, away from the vagina. Be careful not to bring anything up from the anus toward the vagina. Even a piece of stool that is too small to see can cause infection.
5.1.4 Check for heavy bleeding (haemorrhage)
After the birth, it is normal for a woman to bleed the same amount as a heavy monthly period. The blood should also look like monthly blood — old and dark, or pinkish. At first, the blood comes out in little spurts or gushes when the uterus contracts, or when the mother coughs, moves, or stands up, but the flow should reduce over the next two to three days and become the more watery reddish discharge known as lochia (Study Session 2).
Very heavy bleeding is dangerous. To check for heavy bleeding in the first six hours after birth check the mother’s pads often — 500 ml (about two cups) of blood loss is too much. If she soaks one pad per hour, it is considered heavy bleeding. If the mother is bleeding heavily, and you cannot stop it, take her to the hospital. Watch for signs of shock. Remember that postpartum haemorrhage is a major cause of maternal mortality and it can happen at any time in the postnatal period – though it is most common in the first seven days.
5.1.5 Check the mother’s genitals for tears and other problems
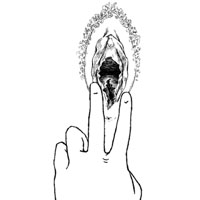
Use a gloved hand to gently examine the mother’s genitals (Figure 5.3) for tears, blood clots, or a haematoma (bleeding under the skin). If the woman has a tear that needs to be sewn, apply pressure on it for 10 minutes with a clean cloth or pad and refer her to the health centre. If the tear is small, it can probably heal without being sewn, as long as it is kept very clean to prevent wound infection.
Ask her to rest as much as possible and tell her she should not climb up or down steps or steep hills. Someone else should do the cooking and cleaning for the family for a few days. To speed healing, she should also eat plenty of healthy food, keep the genital area clean (washing it with water after using the latrine) and cover it with a clean cloth or pad.
Bleeding under the skin (haematoma) or pain in the vagina
Sometimes the uterus gets tight and hard and there does not seem to be much bleeding, yet the mother still feels dizzy and weak. If this happens, she may have bleeding under the skin in her vagina called a haematoma (Figure 5.4). The skin in this area is often swollen, dark in colour, tender and soft.
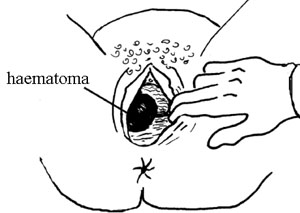
Although a haematoma is painful, it is usually not serious unless it gets very large. If the haematoma is growing, press on the area with sterile gauze for 30 minutes or until it stops growing. If the mother has signs of shock, treat her for shock and take her to the nearest health facility so that the haematoma can be opened and the trapped blood can be let out.
Prolapsed cervix
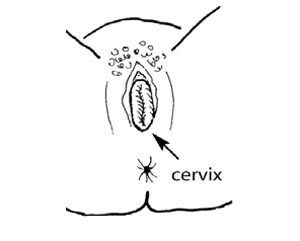
Check to see if the cervix has prolapsed (dropped down to the vaginal opening; Figure 5.5). This problem is not dangerous, and the cervix will usually go back up inside the mother in a few days. Help the mother to raise her hips so that they are higher than her head. Ask her to do squeezing exercises with the muscles of her vagina and pelvic floor at least four times a day.
If the cervix stays at the vaginal opening for more than two weeks, the mother should be referred. A cervix that stays prolapsed can cause problems if the woman has another child.
5.1.6 Help the mother to urinate

A full bladder can cause bleeding and other problems. A mother’s bladder will probably be full after the birth, but she may not feel the need to urinate. Ask her to urinate within the first two to three hours. If she is too tired to get up and walk, she can squat over a bowl on the bed or on the floor (Figure 5.6). She can also urinate into a towel or thick cloth while lying down. If she cannot urinate, it may help to pour clean, warm water over her genitals while she tries.
If the mother cannot urinate after four hours, and her bladder is not full, she may be dehydrated. Help her to drink fluids. If her bladder is full and she still cannot urinate, she needs to have a catheter inserted to drain her bladder. If you have been trained to do this, catheterise her as shown in Study Session 22 of the Antenatal Care Module and your practical skills training. Then refer her to the nearest health centre or hospital.
What is the single most important thing you should always do before examining a woman who has just given birth?
Always wash your hands thoroughly to minimise the chance of transferring any bacteria that may be on them. If you are examining her genital area, then after washing your hands put on surgical gloves.
5.2 Nutrition after childbirth
5.2.1 Eating and drinking in the first few hours
Most mothers are ready to eat soon after the birth, and it is good for them to eat any kind of nutritious food they want. If a new mother is not hungry, she should at least have something to drink. Fruit juice or atmit tea is good because it gives energy (Figure 5.7). Many women want something warm to drink, like tea. Some juices, like orange juice, also have vitamin C, which can help healing. (But she should avoid soda pop like Coke, which is full of sugar and chemicals but has no nutrition.)
If the mother cannot (or will not) eat or drink within two to three hours after the birth:
- She may be ill. Check for bleeding, fever, a hypertensive disorder, or other signs of illness that may be taking away her appetite.
- She may be depressed (sad, angry, or without any feelings). Encourage her to talk about her feelings and needs. (Postpartum ‘blues’ were described in Study Session 3.)
- She may believe that certain foods are bad to eat after a birth. Gently explain to her that she must eat to recover from the birth and to be able to care for her baby.
5.2.2 Counselling on postnatal nutrition
After delivery, women’s routine food intake should be increased to cover the energy cost of breastfeeding and for her to recover her normal energy and health. She should eat about 10% more than before she was pregnant if she is not moving around much or doing her usual work, and about 20% more if she is physically active. In practical terms, she is advised to take at least one or two additional meals every day. Nutritional counselling should include:
Many rural families cannot afford to buy extra food for new mothers. Study Session 14 in the Antenatal Care Module gives advice on eating well with little money.
- Advising the mother to eat a variety of high protein, high energy foods (as much as the family can afford), such as meat, milk, fish, oils, nuts, seeds, cereals, beans and cheese, to keep her healthy and strong. Your nutritional advice should depend on what is available at home and on what they eat as their staple diet. The most important thing is to tell them that she needs to eat more than usual.
- Exploring whether there are important cultural taboos about eating foods which are really nutritionally healthy. For example, in some cultures it is considered bad to eat high-protein foods, spicy foods, or cold foods after a birth. Respectfully advise against these taboos and tell the woman that there is no nutritious food item that needs to be restricted.
- Talk to family members, particularly the partner and/or the mother-in-law, and encourage them to help ensure the woman eats enough of a wide variety of foods and avoids hard physical work.
Advise the mother to take micronutrient supplementation regularly to prevent deficiency disorders and anaemia, as we describe next.
5.2.3 Preventing iodine deficiency

Adding iodine to salt is called iodination and using iodised salt in cooking is recommended in the postnatal period, especially in areas of the country where goitre is common as a result of too little iodine in the diet (Figure 5.8). Iodination of salt has been shown to be a highly effective means of preventing iodine deficiency. Giving iodised oil by mouth or injection can be used as an interim measure in endemic regions where provision of iodised salt may not be feasible. Encourage the mother to use iodised salt every day during the postnatal period, if it is available. Otherwise, a dose of iodised oil can be given to the mother soon after delivery if goitre is common locally.
5.2.4 Preventing vitamin A deficiency
Counsel the mother on prevention of vitamin A deficiency, which not only threatens her sight, but is a major cause of childhood blindness in babies fed by vitamin A-deficient mothers. Vitamin A in the diet increases resistance to infection and is especially important in producing nourishing breast milk.
Can you recall some foods that are rich in vitamin A? (You learned about this in the Modules on Antenatal Care and Nutrition.)

Yellow vegetables like carrots, yellow fruits like mangoes, and dark green leafy vegetables such as cabbage and spinach have a lot of vitamin A. So do liver, fish liver oil, milk, eggs and butter.
Remember that the maximum dose of vitamin A for pregnant women is 500,000 IU; beyond this dose is toxic
Part of routine postnatal care is to check if a vitamin A capsule has been given to the mother. The recommended dose for breastfeeding mothers is one 200,000 IU (International Units) vitamin A capsule once after delivery or within six weeks of delivery. Explain that vitamin A will help her to recover better and that the baby will receive the vitamin through her breast milk. Explain to her if she feels nauseated or has a headache after taking the capsule, it should pass in a couple of days.
5.2.5 Preventing iron and folate deficiency
Pre-existing anaemia can be aggravated by the effects of maternal blood loss and is one of the major contributors to maternal mortality in the postnatal period. Encourage mothers to eat foods rich in iron (e.g. dark green leafy vegetables, beans, peas and lentils, poultry and red meat, organ meats such as liver and kidney, and whole grain products), and foods which enhance iron absorption (fruits and vegetables rich in vitamin C). Tell her to take one tablet containing 60 mg of iron and 400 micrograms of folate (folic acid) every day for three months after the birth, and give her a three months’ supply. (In some places you may have separate iron and folate tablets, but the dosage is the same.) Advise her to store the tablets safely where children cannot easily find them.
Good routine postnatal care for the mother includes counselling her about her nutritional needs. What will you advise her?
That she needs to begin drinking and eating in the first few hours after the birth; that breastfeeding means she will need to eat more (especially high protein foods); if she is in an area where goitre is common, encouraging her to use iodised salt; explaining to her the value of vegetables and other foods which are rich in vitamin A, iron or folate.
5.3 Emotional support for the mother
When you arrive at the house, the first thing you need to ensure is that the mother and baby are not isolated from other family members for cultural reasons. You may have solved this problem during earlier conversations with the family, but during every visit make sure that the mother has all the necessary social support and that family members are visiting her regularly. Together with the community leaders you should try to bring an end to the practice of seclusion, keeping the new mother and baby away from social relations, if it is still practiced in your community. Instead, advise and explain to the woman to always have someone near her for the first 24 hours and family members should be in regular contact every day during the first week to respond quickly to any danger signs in her condition.
5.3.1 Fathers and other family members can help

Encourage the partner to be around the mother at least for the first week of the postnatal period to provide emotional support and to take care of her and the baby (Figure 5.9). In the Ethiopian context, caring for the new mother is usually the responsibility of the grandmother and/or the mother-in-law. As they have already gone through all of these experiences, they are good at providing physical and emotional support to the mother and her baby. They can free her from the routine domestic chores, and this should be encouraged.
5.3.2 When the mother isn’t interested in her baby
Some mothers do not feel good about their new babies (Figure 5.10). There can be many reasons for this. The mother may be very tired, or she may be ill or bleeding. She may not have wanted a baby, or may be worried that she cannot take care of one. As you learned in Study Session 3, she may be very depressed: signs of this are if the woman seems sad, quiet, and has no interest in anything. Also watch for other signs of abnormal behaviour which are different from her usual way of behaving.

What to do if you are concerned about a mother’s lack of interest in her baby:
- Check her carefully for signs of blood loss or infection, or a hypertensive disorder. She may be ill, rather than depressed or anxious.
- You might talk to the mother about her feelings, or you may feel it is better to leave her alone, and to watch and wait.
- If you know that she was seriously depressed after a past birth, talk to the family about giving her extra attention and support in the next few weeks. Usually this depression passes in time, but sometimes it takes a few weeks or even months, and you may need to refer her for additional assessment and treatment. If she demonstrates any of the signs of postpartum psychosis (Box 5.1), refer her urgently.
- Make sure someone in the family takes care of the new baby if the mother cannot or will not.
![]() Postpartum psychosis can be life-threatening, so treat it as an emergency. You will learn more about psychosis in the Module on Non-Communicable Diseases, Emergency Care and Mental Health.
Postpartum psychosis can be life-threatening, so treat it as an emergency. You will learn more about psychosis in the Module on Non-Communicable Diseases, Emergency Care and Mental Health.
Box 5.1 Signs of postpartum psychosis
This condition is rare (affecting about one in 1,000 women), but it is very serious and the mother should be referred urgently for specialist treatment if she is experiencing any of the following symptoms:
- Hearing sounds or voices when no-one is there
- Seeing things that are not real
- Feeling as though her thoughts are not her own
- Feeling afraid that she might harm herself or her baby
- Rapid weight loss and refusal to eat
- Going without sleep for 48 hours or more.
5.4 Encouraging care-seeking behaviour
Encourage the mother, her partner and other family members to seek care immediately if they notice any of the danger symptoms, either in her physical or her emotional state. Delays are a very important cause of maternal and neonatal deaths in the early postnatal period and include:
- Delay in early recognition and decision making to seek help, due to wrong beliefs and cultural taboos. Families may also be afraid of the costs involved if they access the health system.
- Delay in getting transportation to the Health Post or higher level health facility, or getting a health worker to visit the house.
- Delay in receiving appropriate care once in the health facility, due to inadequate staffing or lack of equipment or supplies.
Empowering the mother and the family on early care seeking is fundamental in delivering optimum postnatal care. You should try to develop the capacity of the community to cope with any emergency condition that may occur during the postnatal period. Particularly, attention should be given in every village to designing an emergency evacuation system for mothers and newborns with life-threatening conditions.
Summary of Study Session 5
In Study Session 5 you have learned that:
- The focus for postnatal maternal care is on early identification of the general danger signs through regular checks on the mother’s temperature, pulse and blood pressure, physical examination for contraction of the uterus, bleeding, damage to the genital area, infection or hypertensive disorders, followed by prompt referral.
- The core care that you need to provide to the postnatal mother includes measuring her vital signs at every visit, washing her genital area and checking for tears, blood clots, cervical prolapse and bleeding, helping her to urinate, eat and drink, and giving her micronutrient supplementation (vitamin A, iron and folic acid).
- Counselling the mother, her partner and other family members during the postnatal period focuses on empowering them to recognise the general danger symptoms and seek appropriate care quickly, improve her nutrition to support breastfeeding and recovery, and give her emotional support and help with daily living.
- Seclusion of mothers and babies in the postnatal period is not good for the mother’s mental health and may leave her at risk of neglect, feeling isolated and depressed, and danger signs may be missed if no-one is with her.
Self-Assessment Questions (SAQs) for Study Session 5
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering the questions below. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 5.1 (tests Learning Outcomes 5.1 and 5.2)
You arrived too late to deliver a baby which was born two hours before you got there. What do you do?
Answer
- Check that the mother’s temperature, pulse rate and blood pressure (her vital signs) are normal.
- Palpate her abdomen to check that the uterus is contracting. Do this again 30 minutes later and then every hour for the next three hours.
- Monitor very carefully how much she is bleeding – if she is soaking more than one pad an hour and you can’t stop it, take her to the nearest health facility. Make sure you check for any signs of shock and start pre-referral IV fluid therapy if her blood pressure is low and falling and her pulse rate is fast and rising.
- Gently help her to clean herself – belly, legs and genitals (using soap and very clean water). Check the genitals for any tears, injuries or bleeding under the skin (haematoma), or a prolapsed cervix (the cervix has dropped to the vaginal opening)
- Help her to urinate.
- Make sure she starts drinking to rehydrate her, and if possible encourage her to eat some food.
SAQ 5.2 (tests Learning Outcomes 5.1, 5.3 and 5.4)
Good nutrition and support for the postnatal mother are key aspects of good postnatal care. Complete Table 5.1 to show, for each problem in the first column:
- What you hope the mother or her family would do.
- What you would do to ensure the mother has all she needs.
| Problem or potential for a problem if not addressed | Actions the mother or her family can do to help her | Treatments or other actions that you can provide |
|---|---|---|
Goitre (caused by iodine deficiency) | ||
Not eating or drinking in the first few hours | ||
Lack of energy (maintaining energy when breastfeeding) | ||
Vitamin A deficiency | ||
Anaemia | ||
Seclusion of mother and baby | ||
Lack of interest in the baby | ||
Support for the mother |
Answer
| Problem or potential problem | Actions the mother or her family can do to help her | Treatments or other actions that you can provide |
|---|---|---|
| Goitre (caused by iodine deficiency) | Use iodised salt in cooking. | A dose of iodised oil after delivery, if goitre is common locally. |
| Not eating or drinking in the first few hours | The woman should try and remember that she must drink and eat for her own health and the health of her baby. | Check for bleeding, fever or other signs of illness which may be an underlying problem; encourage the woman to talk about how she is feeling. |
| Lack of energy (maintaining energy when breastfeeding) | Eat one to two more meals a day of high protein foods (meat, milk, oils, nuts, etc) if possible. | Check if there are taboos about foods, talk to family members about ensuring the woman eats enough and avoids hard work. |
| Vitamin A deficiency | Increase intake of high vitamin A, vegetables and fruits, e.g. carrots, mangoes, cabbage and spinach; also eat liver, fish liver oil, milk, eggs and butter. | One 200,000 IU vitamin A capsule taken after delivery or within six weeks of delivery; explain the importance of foods rich in vitamin A. |
| Anaemia | Increase intake of vegetables and fruits rich in iron and folate. | Give her enough tablets (60 mg iron and 400 micrograms folate) to take one every day for three months. |
| Seclusion of mother and baby. | Family members stay with the mother and newborn to offer support, despite the cultural norms. | Explain why the woman needs someone near her, especially in the first seven days, when there is the highest risk; a quick response is needed if something goes wrong. |
| Lack of interest in the baby | Family to give extra attention and support, and have someone care for the new baby if necessary. | Check for illness, blood loss or infection. Talk to her. Check if she is hearing voices, or ‘seeing things’. If the latter, refer her for psychiatric help. |
| Support for the mother | Partner, grandmother and/or mother-in-law to take over some routine domestic jobs. | Make sure partner and family know the danger signs and the importance of avoiding delay in getting the mother to a health facility. |