Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Thursday, 23 July 2026, 3:37 PM
Module 3: Module 3 - Children’s rights and health practice
Introduction to Module 3
This is the third module in a course of five modules designed to provide health workers with a comprehensive introduction to children’s rights. While the modules can be studied separately, they are designed to build on each other in order.
Module 1: Childhood and children’s rights
Module 2: Children’s rights and the law
Module 3: Children’s rights and health practice
Module 4: Children's rights in the wider environment: the role of the health worker
Module 5: Children’s rights: planning, monitoring and evaluation
Module 3 provides four crucially important study sessions for health care practitioners in relation to ensuring children’s rights in health care settings. Each of these sessions is designed to take approximately two hours to complete. The sessions provide you with an introduction to these topics and are supported by a range of different activities to help you develop your understanding and knowledge. The activities are usually followed by a discussion of the topic, but in some cases there will be answers at the end of the study session for you to compare your own answer to before continuing. We have provided you with space to write your notes after an activity, however if you wish, you can use a notebook.
- Study Session 1 stresses the importance of children being actively involved in their own health care. In the session you will explore the implications of listening to children and taking their views seriously. You will also learn about the importance of recognising children’s evolving capacities. By the end of the session you will have a better understanding of why the participation of children is so important and what are the main difficulties and challenges.
- Study Session 2 will introduce you to two important principles: the right of children not to be discriminated against and the need for adults to think about the best interests of children when they are making decisions on their behalf. It will help you explore the different forms of discrimination and the importance of treating children equally in a health care setting. The session will question how can we act to ensure the best interests of children and prevent discrimination? And how are the best interests of children to be determined and balanced against any other considerations?
- Study Session 3 is devoted to the topic of violence against children. It looks at how you can support the right of children to be free from violence and abuse. In this study session you will question your own views and attitudes towards violence, recognise the signs of abuse and understand the impact it has on children. By the end of the session you will have explored the important role of health practitioners in identifying and reporting violence against children.
- Study Session 4 focuses on an issue important to any health worker, which is how to make their practice environment ‘child-friendly’. You will consider what is meant by being child-friendly and the role that standards and charters can have in promoting a positive environment. By the end of the session you will have had the opportunity to reflect on your own health facility and plan how it can be improved to support the rights of children.
1 The child as an active participant
Focus question
Why should children be involved in making decisions concerning their health?
Key words: competence; confidentiality, decision-making, participation
1.1 Introduction
In this session you will learn about one of the fundamental rights contained in the United Nations (UN) Convention on the Rights of the Child. Article 12 of the UN Convention gives children the right to express their views and have them taken seriously. This means that children are entitled to be involved in decisions that affect them. It is commonly described as the right to participation. It challenges assumptions in East Africa that children are not expected to question or challenge adults or to contribute to decisions adults make on their behalf. Article 12 does not encourage children to be disrespectful or disobedient. It seeks to promote respect for children to be more actively involved in their own lives and to be able to influence the things that happen to them. Children are not just passive recipients of adult care and protection – they can also contribute to the exercise of their rights and participate in decisions that affect them.
This session will help you to explore your own views about child participation, to appreciate the capacity of children to influence decisions about their health. You will also think about why this is important for health workers to understand.
1.2 Learning outcomes
When you have studied this session, you will be able to:
- explain correctly the meaning of the above key words
- understand the right that children have to participate in their own health care
- discuss the benefits of involving children in decisions that concern their health
- identify situations in your practice where children should be involved in decision making.
1.3 Your own childhood experience
Activity 1:1 Thinking about your own childhood experience
Think back to when you were a child and try to remember a situation when you visited a doctor, a health facility or a hospital.
What was your experience like? Did the doctors or nurses you met ask you questions? Did they listen to your response? Did they explain what was happening to you? Did you have an opportunity to ask questions? Did they involve or encourage you in any other way?
How did your experience make you feel?
Discussion
It is a very common experience of children that adults make decisions about them without explaining why that decision has been made, asking what he or she feels about it or enabling them to influence that decision.
For some children, not being listened to can have a harmful effect on their health, as this quote highlights:
At school I got a sudden headache. I went to the nearby school but they ignored me thinking I was playing truant. When I went home to inform my mother, she was out. As my condition was getting worse I had to go to my sister. When I told her she took me to the hospital run by nuns who admitted me with serious malaria. My sister then called my mum to tell her I had been admitted. What would have happened if I did not have a sister? Since mum is at work, I could have died. Just because they ignore children.
(From the consultation undertaken in Tanzania for the development of this module)
When you recalled a memory of childhood, perhaps you remembered how vulnerable you felt when you had no control over what was happening to you. Maybe you felt upset because the nurse did not take account of your understanding of the situation. This might have meant she/he gave you the wrong treatment, or was unable to make an effective diagnosis. It might also have made you feel humiliated and frustrated. If a doctor or nurse imposed a treatment, for example, an injection, without discussing it with you or addressing your fears, you might have experienced more distress or pain than was necessary.
If the doctor or nurse explained what was happening to you, then you may have felt reassured and less fearful. They may have been particularly kind and spoken to you in a gentle way, encouraging you to be brave or telling you that the treatment would not hurt and that it would not be long before you could go back home. As a result, you may have felt valued, and even have positive memories of a time visiting a clinic or hospital.
All of us want to be respected and recognised when decisions are being made that have important implications for our health and well-being. This applies as much to children as to adults. It is important to remember these feelings when you are working with children: you can then respond to them as you might have liked to be treated when you were a child.
As health workers you need to put yourselves in the shoes of the children you care for in order to understand their feelings, anxieties and expectations. You can explain why you are making decisions and involve them in that process. They are then in a better position to understand the reasons for the treatment, are more likely to be open about their condition and symptoms, and are more likely to cooperate in any treatment.
1.4 What is child participation?
Participation is a process of being involved in decisions and actions that affect you. Children traditionally are denied this opportunity. However, this right to be heard and taken seriously is one of the fundamental values of the United Nations Convention on the Rights of the Child and the African Charter on the Rights and Welfare of the Child. Of course, children have always participated in many ways within societies – for example, at the community level, through play and art, and in their economic contribution to their families. In the context of children’s rights, however, the term participation is now very widely used as a short-hand to describe the process of children expressing their views and having them taken seriously.
Participation can be defined as an ongoing process of children’s expression and active involvement in decision-making at different levels in matters that concern them. It requires information-sharing and discussion between children and adults based on mutual respect, and requires that full consideration of their views is given, taking into account the child’s age and maturity.
(Lansdown, 2011, p. 3)
It is important to understand that this does not mean that children should always have their own way, or that adults can no longer make decisions on behalf of children. What it does mean is that children can and should be involved in those decisions and have their views taken seriously, even if they cannot always be complied with.
Children can form and express views from the earliest age, but the way they participate, and the range of decisions in which they are involved, will necessarily increase as they grow older and more able. Young children’s participation will be largely limited to issues relating to their immediate environment within the family, care facilities and their local community. However, as they grow older and their capacities evolve, they are entitled to be involved in issues that affect them in the immediate family, in their community, their country, and even at the international level.
Study note
For ease in reading the text, from hereon we will be referring to the UN Convention and the African Charter.
Activity 1.2: Role play demonstrating a lack of child participation
If you are studying in a group you could conduct this activity as a role play. There are four characters, so you will need to have at least four people for a role-play activity. Otherwise you can read it and then consider the two questions that follow.
Background
A parent decides to take his or her daughter, aged 8, to the health clinic because they are worried that the child might have malaria. A health worker is available straight away.
Parent: Greets the health worker and explains that the child has a fever and headache.
Health worker: Examines the child silently and straight away prescribes medication without any discussion with the child. She also decides the child needs an injection and prepares to give the treatment.
Child: Sees the large needle and runs out crying to the reception area.
Receptionist: Asks what is the matter.
Child: Cries and says the doctor is going to give her an injection and she does not understand why. She is frightened.
Questions:
- What do you think about this situation?
- What would you do differently to permit the child’s participation? Act it out again, this time taking account of the child’s right to be heard.
Once you have acted it out again, note the points at the end of the session for Activity 1.2.
1.5 Four rights that promote children’s participation
Some of the key rights that need to be understood in relation to the child as an active participant in their own health care are contained in Articles 5, 12, 16 and 17 of the UN Convention. Figure 1.1 below shows the relationship between the four articles and children’s involvement in their own health care. We will now move on to explain these four Articles in a little more detail.
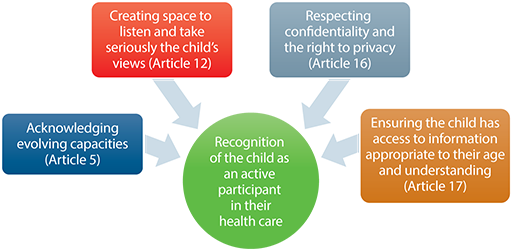
Article 5: Acknowledging children’s evolving capacities
Article 5 recognises that parents have rights and responsibilities to provide guidance and direction to children. However, it also introduces boundaries on how those responsibilities are exercised. For example:
- Parents’ rights exist in order to protect children’s rights. For example, a child has a right to a name, so parents have the authority to give a child a name because a small baby cannot exercise that right for him or herself. Parents can give consent to medical treatment while the child is too young to do that for him or herself.
- Any guidance or discipline must respect children’s rights. For example, parents cannot impose punishments on a child that causes them physical, emotional or psychological harm. This means they should not punish a child by denying them food because this would abuse the child’s right to be as healthy as possible. Beating a child is also an abuse of their right to protection from violence.
- Parents should recognise that as children are able to exercise their own rights, then they should be increasingly allowed to do so. They should respect their child's evolving capacities (you studied evolving capacities in Module 1). In other words, parental rights exist until a child can exercise those rights for him or herself. After that, children should be allowed to take decisions for themselves. Children are not the property of the parents. The level of guidance and direction provided by parents should reduce as children acquire greater competence.
Children learn through experience and observation of what is going on around them. They develop their capacities to think and make decisions through guidance by the adults and other children around them. Constant mentoring and guidance as they grow through childhood enables them to develop their capacities.
Article 12: Listening to children and taking their views seriously
Article 12 of the UN Convention states that children have the right to be involved in all matters that affect them and to have their views taken seriously in accordance with their age and maturity. This applies to individual decisions such as their own health care. It also means that children as a group should be involved in matters that affect them, for example, how and what health care services are provided in their local community. The Committee on the Rights of the Child has identified Article 12 as a general principle that must be considered in the way all other rights are implemented. For example, in order to ensure that children’s right to health is fully realised, it is necessary that children are listened to and involved in their own health care. In order to ensure children’s right to protection from violence, they need to be listened to and taken seriously.
Children are entitled to make choices about whether or not they want to participate and to what extent. In relation to health care, for example, some children will want their parents to retain full responsibility for taking decisions. Some will want to share it with their parents. Others may feel that as it is their life and future at stake, it should be their responsibility to make choices for themselves.
My mum took me to the dispensary. I was afraid of the injection and wanted to run away. The nurse called some men who held me down by force. They hurt my chin but she didn’t care.
(From the consultation undertaken in Tanzania for the development of this module)
Article 16: Respecting confidentiality and the right to privacy
Article 16 of the UN Convention states that children have a right to privacy. This means that children are entitled to respect for privacy and confidentiality, for example, in getting advice and counselling on health matters, depending, of course, on their age and understanding. Governments are expected to introduce laws and regulations to ensure that older children are able to seek medical help in confidence. As a health worker, you need to know what the law says about keeping the medical information of older children confidential, and to protect that confidentiality as far as possible.
Confidentiality
Respecting confidentiality means that information is kept a secret. It means that information about the child, or things that the child has talked about should not be disclosed to anyone else unless the child agrees.
Respect for confidentiality is important as young people are likely to avoid seeking medical help if they fear either that they will not be seen without their parents or, that if seen alone, their parents will be notified. Clear and well-publicised policies that confidentiality will be respected will encourage children to approach a nurse or doctor. They should then feel free to discuss their situation more frankly and explicitly than might otherwise be the case. The outcome will certainly be better access to health care and earlier interventions to promote good health. There are many circumstances where the principle of respecting confidentiality is of crucial importance to children’s safety, well-being and dignity.
They maintain confidentiality for common diseases. But for STIs, no confidentiality. You can go to the dispensary to be treated and then you find that after a few days, people know what was your problem and even the meds you were given.
If I go to the dispensary on my own, my parents should not be told without my permission. Some sicknesses are my private affair.
(From the consultation undertaken in Tanzania for the development of this module)
Article 17: Ensuring that the child has access to age appropriate information
Children can only make meaningful decisions if they have access to relevant information. As a health worker, you can play a key role by ensuring that children have appropriate information to help them make healthy choices in their lives. For example, information on how to keep healthy, how to avoid risks, information about sexual and reproductive health and HIV/AIDS, illegal drugs and alcohol, diet and nutrition. You could be involved, in collaboration with young people, in developing preventive and promotional materials on health to disseminate within your local community. If children are ill, you need to provide them with information about the nature of the condition, the symptoms, the treatments needed, the implications of those treatments, and how to avoid further problems. Such information enables them to appreciate the importance of the decisions they make and empowers them to make safe choices in the future.
We are told what the meds are for what but never ever been told about side effects.
Doctors don’t want to be being asked questions. They say: ‘Who is the doctor, you or me?’
We are never given the chance to ask.
(From the consultation undertaken in Tanzania for the development of this module)
Activity 1.3: Participation in the African context
Read the article below (adapted from Lansdown, 2011, p. 17) and then answer the two questions that follow.
If you are working in a group discuss your opinions afterwards..
Understanding participation in the African context
Participation of children as stated in the Articles of the UN Convention is sometimes seen as foreign, superficial and alien to the African culture. In any discussions on participation of children, it brings out political, cultural, social and emotional concerns and divides. It can be viewed as a threat to parental authority, and an intrusion on the authority of the family head in particular.
In the past, many African traditions encouraged child participation without realising that they were doing so – making it possible for children to access useful information and contribute to decisions. Sitting round the fire, sharing folklore, stories and songs, elderly people gave children the opportunity to participate actively. This included questions and answers, the sharing of opinions and personal interpretation of the messages in a story. Dances within the community also prompted discussions around cultural practices and morals. While some of these forums had negative aspects such as encouraging stereotyping, early marriage and the subordination of women, they nevertheless did solicit the views of children.
While child participation has been practiced in the African context for decades, this form of participation in traditional African society is beginning to disappear because modern-day living has led to the loss of these practices.
These days, while many adults believe that children have rights to life, health and education, many are not convinced that children have the right to participate in decisions affecting them, their family or their community. Child participation is often restricted because African family relationships can be divided into categories with role expectations clearly defined. In some communities children are not allowed to speak among adults without permission as doing so may bring disgrace on the parents.
Children’s rights are enshrined in the UN Convention, which was developed outside East Africa. However the Convention has been interpreted and incorporated into the African Charter on the Rights and Welfare of the Child, which has been accepted by African governments as good principles for all African countries (Ministry of Gender, Labour and Social Development, 2008).
Questions
- What can you learn from this article?
- How could you use positive traditional practices to enhance children’s participation in your country or community?
Discussion
- This article suggests that children’s participation is often viewed as an imposition from outside African culture. It is seen as an alien concept that challenges traditional ways of relating to children. However, you will also have learned that, in fact, many traditional practices in Africa did involve listening to children. Story-telling, sharing traditions, sitting together around the fire, all provided opportunities for children to talk with elders and share experiences. What is missing is a way of linking these traditional practices with the modern language of the UN Convention. The article highlights the fact that there is no real conflict between the values of the Convention and African culture. The similarities between the UN Convention and the African Charter provide evidence of the compatibility of the values.
- You could begin to think about traditional practices within your own community that might have involved children, and then explore how they might be used to help strengthen understanding of their value and how they might be applied in the current context of children’s lives. For example, in some communities, children and young people have expressed concern that traditional rites of passage such as male circumcision place boys’ health at risk, particularly in areas where there is a high rate of HIV/AIDS. Instead of ignoring those concerns, it may be possible to bring different members of the community together in a ‘circle’ to discuss the issues. Some elders may feel it is threatening to their culture and authority to change these traditions whereas young people may feel it is more important to stay healthy than to preserve traditions. By bringing generations together to listen to each other, it may be possible to find a way of maintaining the important rite of passage but doing so in a way that is safer and does not place boys at risk.
1.6 Why is child participation important?
Participation is not only a right of every child, but it also brings with it many positive benefits for children themselves, including to their health and well-being. It can also make the work of the health worker easier:
- Involving children in their own health care makes children feel more respected. And when children feel that they are respected, listened to and that their views are valued and taken seriously, this helps reduce the vulnerability associated with being ill, in pain and dependent on others.
- If you listen to children, it will help you understand the child’s condition better, and this will help you treat them more effectively.
- Being listened to helps relieve anxiety and enables children to cope better with treatment.
- If children have information about their condition, they are better able to understand and address what is happening to their bodies and why things are happening the way they are.
- It gives them confidence. If children are involved in the process of treatment, they will not have fears that actions will be taken without their knowledge or understanding.
- It encourages co-operation. If children lack information, they are likely to be more frightened and therefore less willing or able to co-operate in treatment which, in turn, makes interventions more painful and distressing.
- It avoids unnecessary distress. When information is withheld, children may worry unnecessarily about what is going to happen to them.
- Often the imagined risks are far worse than reality. If they have information, children can prepare appropriately for what is happening and receive necessary counselling, comfort and support.
- Children develop a better understanding of their own health care needs.
- It encourages them to take more responsibility for their own health because they develop a better sense of the causes and consequences of their actions or inactions.
1.7 What are the challenges to participation and how can we address them?
There are a number of challenges to making sure children are listened to by health professionals. As we discussed earlier, in many countries and cultures, including in Africa, there is a considerable resistance to the idea that children and young adults have to be consulted and listened to. It runs counter to the assumption that adults know best and that children lack the experience and competence to take responsibility for decision-making. Many parents and professionals are also concerned that providing children with information about their medical condition might be painful for them to accept. They argue it is better to protect children from such information and choices. The following discussion looks at five particular challenges and provides some ideas on how to address these.
1.8 Capacity to participate
Are infants capable of expressing their views? If so, how?
What about a child who cannot communicate verbally? How can you acknowledge and respect the views of these children?
Even very small children can tell you what they like or dislike about being in hospital and can produce ideas for making their stay less frightening and distressing. Provided they are given support, adequate information and allowed to express themselves in ways that are meaningful to them, all children can participate in issues that are important to them. This can be through pictures, poems, drama, photographs, as well as more conventional discussions, interviews and group work.
In the case of babies, their lack of speech should not be an obstacle to considering and respecting their point of view and feelings. For example, they can express their feelings of distress, fear, distrust, or comfort through facial expressions, body language, crying and smiling. A health worker can use this information to identify needs such as the need for a nap or a feeding, responding to whether or not they are in pain. It is important for health professionals to establish a positive relationship with a baby and his or her parents and involve them during the consultation or treatment.
Some children with disabilities, such as children who are hearing or visually impaired, or those that have autism, may experience difficulties in communicating verbally. It is equally important to explore approaches that allow them to express their views. Parents and caregivers will often be able to advise on how to communicate effectively with disabled children.
All children have the capability of expressing their views. Therefore it is necessary for health professionals to explore the many ways that enable the child to articulate these views, concerns and opinions.
1.9 Assessing competency
Should the views of a six-year-old be given the same weight as the views of a 16-year-old?
At what age are children competent to take responsibility for their own health care?
What defines competence?
Obviously children at different stages of development will have differing capacities to take responsibility for their own health care, although these capacities are not necessarily defined just by age. Children’s capacities are highly dependent on the experiences they have had. For example, young children who have experienced major surgery or frequent medical interventions may have a profound understanding of life or death and how decisions will affect them. There are two distinct issues to consider here.
- All children can be involved in decisions about their health care, even though the actual decisions will be taken by adults. For example, while five-year-old children may lack the competence to decide that they need to go to hospital for an operation, they can indicate if and why they feel comfortable at the hospital, and provide suggestions to improve their stay.
- Some children will have the capacity to give formal consent to their treatment or to refuse treatment, although the legal rights to do so will be determined by the legislation in any given country. You need to know what the law says in your country. Considerations to take into account in assessing children’s capacities to give or refuse consent can include:
- Is the child able to understand and communicate relevant information? The child needs to be able to understand the alternatives available, express a preference, express concerns and ask relevant questions.
- Is the child able to think and choose with some degree of independence? The child needs to be able to exercise a choice without coercion or manipulation and to think through the issues for themselves.
- Is the child able to assess the potential for benefit, risk and harm? The child must be able to understand the consequences of different courses of action, the risks involved and the immediate and long-term implications.
In general, health professionals need to listen to children, provide appropriate information and give them time to articulate their concerns, so that children can develop the confidence and ability to contribute effectively to their own health care.
1.10 Child participation: obligation or burden?
Do children have an obligation to express their views?
Does giving children rights to be heard burden them unnecessarily?
Neither the UN Convention nor the African Charter imposes obligations on children to express their views. Rather, they provide a right for the child to do so. Children should be given the opportunity to participate and express their views if they so choose, and be helped to do so.
The assumption that children will be burdened unnecessarily is rooted in a view of childhood that imagines children and adolescents do not take decisions or responsibilities at very early ages. However, even small children can act responsibly, for example, in caring for younger siblings, coping with parents in conflict, deciding on what games to play, and negotiating rules. Listening to the views of children, and supporting their participation in a way that respects their evolving capacities teaches children to listen and respect the opinions of others, clarify their own opinions and make decisions about their lives.
1.11 The right to protection versus the right to privacy
Should a child’s right to protection from violence, abuse or neglect override their right to privacy and confidentiality? If so, when?
All rights are inter-dependent. However, at times there can be a tension between different rights. For example, it may be the case that in order to protect a child from serious risk of abuse, it is necessary to override their right to privacy. Depending on the laws and regulations in your country, health care professionals may have an obligation to report cases of abuse and neglect, even where the child is adamant that he or she does not want the information to be taken further. In such circumstances, it is important to be clear with the child about the boundaries of confidentiality, what the law says, and to involve the child as far as possible in deciding how and when the information will be reported. It is important to remember that violence and abuse of children disempowers them. The strategies adopted to protect them should not further disempower them. Any action must take account of the child’s individual circumstances and contexts. A ‘one size fits all’ approach should never be adopted.
1.12 Lack of respect for parents
Does participation lead to disrespect?
Will it undermine parental authority?
Listening to children is about respecting them and helping them learn to value the importance of respecting others. It is not about teaching them to ignore their parents. Indeed, the UN Convention states that education should teach children respect for their parents. Listening is a way of resolving conflict, finding solutions and promoting understanding – these can only be beneficial for family life. It can be difficult for some parents to respect children’s rights to participate when they feel that they, themselves, have never been respected as subjects of rights. This does not imply the need to retreat from encouraging children to participate but, rather, the need to be sensitive in doing so. Children should not be led to believe they alone have a right to have a voice; wherever possible, their families should be involved too.
Activity 1.4: Involving children in health care decisions
Think about a situation where you have had a difficult decision to make in your practice. You may have had to override the wishes of a child or his or her parents by insisting on a treatment, or you may have had to breach confidentiality or report an incident. What did you decide to do and why?
If you are unable to identify a case from your own practice, you could think about what you would do for one of the following examples:
- a.A 13-year-old wanting contraception but does not want her parents to be informed. Should her privacy be respected?
- b.An 8-year-old child has HIV, which was transmitted from the mother. Should the child be told even though the mother does not want this?
- c.In a school vaccination programme should individual children be consulted and asked to give their permission?
Now, for your own situation or one of the examples above, consider these questions:
- Would you create time to explain what was happening to the child or would you simply provide information to the parents?
- How would you determine whether the child is competent to make a decision about his or her health care?
- When would you breach a child’s privacy?
If you are working in a group - discuss and debate your experiences and responses.
Discussion
There are no right and wrong answers to these questions. However, there are some issues that it would be useful for you to consider when faced with such cases.
- Some of the negative implications of providing information to the child are that it would take time, it might cause the child distress, and the parents might object. Some of the benefits are that the child might be less anxious, feel more in control, and be better prepared for what is happening. In addition, the child might be more able to co-operate and better able to talk about problems if she or he knows what is happening. Parents would also be better equipped to help the child where there is openness and honesty.
- You could check their level of understanding about the kind of treatment being proposed and its implications. You could make time to talk with the child about their feelings and views and why they are concerned about the treatment proposed or the request for confidentiality. You could assess the child’s ability and competency as an individual and try to avoid assumptions based on their gender or age.
- On the one hand, you may feel it is necessary in order to ensure that a child gets the treatment he or she needs, or in order to ensure their protection. On the other hand, there is a danger that if children feel the health worker will not respect confidentiality, they will not seek help when they need it. This may cause even more harm to the child. As a general guide, you should always respect a child’s privacy unless it is in the child’s best interests not to do so, or where the law requires you to breach privacy.
1.13 Summary
The aim of this study session was to introduce you to the right of children to be active participants in decisions and actions that affect their lives. The key points it addresses are as follows:
- Participation is a process of being involved in decisions and actions that affect you. Despite historical traditional practices that encourage children’s participation, children are often denied this opportunity. However, this right to be heard and taken seriously is one of the fundamental principles in the UN Convention and the African Charter.
- In the field of health care, the right to participate is addressed in four key articles in the Convention: the right to respect for evolving capacities, the right to information, the right to express views and have them taken seriously, and the right to privacy and confidentiality.
- Participation is not only a right but also carries significant benefits for children. It leads to better decisions, it builds their confidence, it reduces fears and anxieties, and it helps children to take on the responsibilities they will have in later years. The health worker benefits too, as children will be more likely to communicate more effectively with the health worker and to cooperate in treatment.
- Many adults have concerns about letting children participate. For example, they worry that children lack capacity or that it will erode parental authority. On the contrary, participation serves to enhance children’s lives and can strengthen relationships between adults and children. Of course, children should never be forced to participate against their will. It is a right not an obligation.
1.14 Self-assessment questions
Question 1.1
List three benefits of children’s participation to children themselves and three benefits to the health worker.
Question 1.2
What do you understand the term ‘evolving capacities’ to mean, and how is this relevant to children’s participation in health care decisions?
Question 1.3
Name three objections you might hear about children’s participation and state how you might challenge these objections.
Question 1.4
Having completed this study session, identify two things that you will do differently in your practice to involve children in decisions that affect their health?
1.15 Answers to activities
Activity 1.2: Role play demonstrating a lack of child participation
- The problem for the child in this scenario is that she has no idea what is happening and why. No-one has bothered to explain to her what is the matter with her and what treatment is necessary to help her to get well.
- If you were the health worker, you could explain to the child that she is ill, what is the matter with her and how having the injection will help her recover. You could give her reassurance about having the injection, for example, you could ask her if it would help if she sits on her parent’s lap and holds their hand. You could explain where you will give the injection and how she will feel afterwards. This way, she may be less frightened. Having an injection may be less painful and distressing if the child has a little more control over how it is delivered and is comforted and supported. You might also involve the parents, explaining to them why it is important to reassure the child and listen to their concerns.
2 Best interests of the child and non-discrimination
Focus question
How should we act to ensure the best interests of children and prevent discrimination?
Key words: best interests, competing interests, direct discrimination, inclusive services, indirect discrimination
2.1 Introduction
In the first study session of this module, we discussed the principle of children as active participants. Children have a right to be involved in the decisions made by adults on their behalf. In this session, we explore the right of children to have their best interests given consideration when adults are making decisions about them, as well as the right not to be discriminated against.
Both the UN Convention and the African Charter emphasise the importance of best interests and non-discrimination. These are two of the guiding principles you studied in Module 2. This session will explain what these two rights mean, their implications for you as a health worker, and will provide guidance on how to apply them in your day-to-day practice
2.2 Learning outcomes
At the end of this study session, you will be able to:
- define and use correctly the key words above
- explain the principle of best interests of the child as it applies to the provision of health services to children
- explain the principle of non-discrimination as it applies to the provision of health services to children
- understand how to make decisions that are in children’s best interests in your practice.
2.3 What is meant by ‘best interests of the child’?
The concept of the ‘best interests of the child’ is a central building block and a guiding principle of both the UN Convention and the African Charter. It means that when any decision or action is being taken that will affect a child, you need to think about whether it is in the best interests of that child.
In all actions concerning children, whether undertaken by public or private social welfare institutions, courts of law, administrative authorities or legislative bodies, the best interests of the child shall be a primary consideration.
(From Article 3, United Nations Convention on the Rights of the Child)
In all actions concerning the child undertaken by any person or authority the best interests of the child shall be the primary consideration.
(From Article 4, African Charter on the Rights and Welfare of the Child)
The Committee on the Rights of the Child has interpreted Article 3 as applying both to children as individuals and as a group. For example it applies to a child’s specific health condition and care, and it applies to decisions affecting groups of children, for example, policies on health or welfare. To give an example, if you are deciding to give a child a particular treatment, you must be sure it is in their best interests to do so. Equally, the way in which your clinic or hospital ward is organised should take account of the best interests of children rather than the convenience of the administrators or doctors.
It is important to understand the weight that should be given to the best interest principle. Article 3 of the UN Convention and Article 4 of the African Charter require that the best interests of the child is a primary consideration. This recognises that other interests can be considered, but that the child’s interests are the most important interests. The scope of the article is extremely wide, covering all actions concerning the child or children.
2.4 How to determine the best interests of a child
There are four aspects you can consider in determining the best interests of a child. These are shown in Figure 2.1 below.
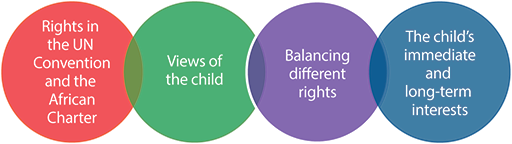
These aspects are interlinked and can be used in any situation where you want to determine the best interest of a child or children.
Rights in the UN Convention and the African Charter
The overall goal of the UN Convention and the African Charter is to promote children’s best interests. The starting point in defining the best interests of the child, therefore, must be to make sure that all their rights are fully realised. Both treaties also make clear what is not in children’s best interests, for example, exposure to all forms of violence, sexual and economic exploitation, harmful traditional practices, and discriminatory laws, policies and practices. Together they provide an important guide to help you assess whether a decision or action may be harmful to a child’s best interests.
Views of the child
The views of the child must be taken into account in determining what is in their best interests. A child’s age, maturity and capabilities are important factors in the weight given to the child’s views, but children of all ages and abilities should have an opportunity to have their views considered. Too often, adults decide what is best for a child without any reference to the child’s experiences or concerns.
Balancing different rights
Determining the best interests of the child also requires you to think about the different rights children have and how they are taken into account with each other. For example, a child requires a stable family environment, but if the child is experiencing harm or neglect in the family home, it may not be in their best interests to stay with their own family. The disruption to the child's life may be necessary in order to protect them. Situations can arise where rights appear to conflict. For example, a competent teenager may exercise his right to refuse treatment, whereas medical opinion considers that the treatment is vital for his long-term health and well-being.
The child’s immediate and long-term interests
Consideration must always be given to both short- and long-term best interests of the child. A child that is at risk of harm or neglect may need to experience temporary disruption to their lives while they are moved to a safe location. However, in the long term this may prevent them from further harm and improve their opportunities in life.
There are no easy answers to such complex dilemmas, but a commitment to the best interests of the child provides a mechanism to help determine how to reconcile tensions, and ensure the realisation of children’s rights.
Activity 2.1: Acting in the best interests case study
Read the case study below, keeping in mind the four interlinked aspects introduced above in section 2.4.
If you are working with another person or in a group, discuss the questions below. Otherwise, try to answer the questions yourself before reading further.
Asha, aged 11 years, has had a history of continued ailment and, because of limited facilities, it took four years to diagnose her illness as leukemia. She has undergone numerous procedures that have controlled the spread of the cancer but these treatments have resulted in secondary complications including a hole in her heart. Her medical advisers say that to reach adulthood she will need a heart transplant but they cannot predict that this will be successful. Asha has said that she has had enough of medical procedures and does not want the transplant. She is supported by her parents. The doctors insist that they should proceed.
- What rights does Asha have in this situation?
- What are Asha’s views?
- What other needs does Asha have?
- What are Asha’s short- and long-term interests?
- In your view, are the doctors right to insist on this treatment?
Discussion
- You may have identified a number of rights that Asha has. She has a right to survival, a right to appropriate health services, and a right for her views to be taken into consideration. These rights are contained in both the UN Convention and the African Charter.
- Asha does not want to be operated on. She has undergone numerous procedures already and may be distressed by the thought of further medical intervention. Her experience to date may have given her a negative perception of medical facilities.
- Agreeing to Asha’s preference may be detrimental to her well-being. In this situation it may lead to further serious illness or even death. In such cases, the health worker, parents, or others, might have to help the child understand the effect of their decision and the advantage of taking the operation.
- Asha’s most immediate interests are to prevent distress and upset, but her right to survive is of greater importance. Consideration has to be given to her evolving capacities to take responsibility for decisions that will affect her future. You would need to decide if she genuinely understands the implications of the choices that need to be made.
- From the limited information available to you, it may not be possible for you to say with certainty whether the doctors made the right decision. They can consider Asha’s views and respond sensitively, ensuring that Asha understands the importance of the operation. They want to give Asha the best medical care to ensure her survival and they are willing to override her views and that of her parents if necessary to achieve this best interest. However, if the operation would be likely to cause significant distress and physical pain both during and afterwards, and was expected to prolong life for only a very short time, would the doctors still be right to insist? While the right to life is vitally important, the quality of life is an important factor to consider when making decisions in health care.
In determining the best interests of the child, there is often no easy right or wrong answer. Rather, consideration of the best interests can be a way of resolving difficult dilemmas and making judgments in complex situations. It provides a guiding principle to help you in those circumstances.
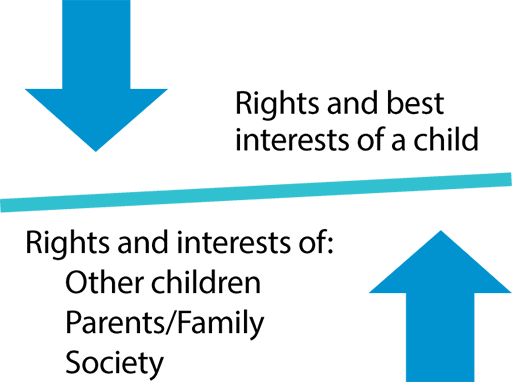
2.5 Competing rights and interests
So far, we have considered how children’s rights law, children’s views, children’s holistic needs and children’s short- and long-term interests help to determine what is in a child’s best interests. Sometimes, the rights and interests of other children, of parents and families, and of wider society, also need to be balanced with the rights and best interests of a child (see Figure 2.2).
Balancing the interests of a child with other children
Situations will arise when ensuring the best interests of one child or a group of children may not be in the interests of other children, and vice versa. For example, health workers might need to respond to a particular epidemic, which might affect other children and adults. They cannot decide to use a particular child for experiments so they can get a remedy to treat the disease and save many other children. Instead they have to identify other strategies that do not compromise the best interest of the child. By contrast, even though an individual child has a right to education, if she or he is continuously disruptive and behaving badly, they may need to be excluded from school for a while so that other children can learn.
Balancing the interests of a child with parents and family
Most parents will have their children’s best interests at heart. However, it cannot be assumed that this will always be the case. There are times when the interests of children and parents can be in conflict. For example, a parent may wish to arrange for a teenage girl to be given a contraceptive injection to prevent her getting pregnant. However, the girl may strongly object to having the injection, perhaps because she is frightened of injections or because she feels it is a sign of her parents not trusting her.
Although the UN Convention and the African Charter fully recognise the importance of parents in children’s lives, and respect their rights and responsibilities towards their children, it also stresses that children have rights and that it cannot simply be assumed that parents will always act in the best interests of children. Where children’s rights are placed at risk by their parents, the best interests of the child must always come first. Where parents abuse or neglect their children, for example, or discriminate against girls. Health professionals need to ensure that this principle underpins all services, procedures or policies, which they are responsible for implementing.
Activity 2.2: Balancing best interests of a child with the interests of the parents
Think about the example described above – a parent forcing a girl to have a contraceptive injection.
If you are working with others on this curriculum, break into two groups with one group taking the side of the parent and the other taking the side of the girl. Then construct a role play arguing out the scenario. What arguments might you bring to support each position?
After the role play, discuss in plenary whether you think it is in girls’ best interests when parents force them to have contraceptive injections to prevent pregnancy while they are still at school?
Compare your answers to those at the end of the study session.
Balancing the interests of a child with wider society
It is sometimes proposed that the interests of the community or the society must take precedence over those of an individual child. For example, where the maintenance of traditional cultures is sometimes seen to be more important than the rights of an individual child who may be harmed within that culture. However, these arguments cannot be used to override the rights of a child. Nor can it be argued that children’s best interests are served by cultural practices, which deny rights that are now guaranteed in law. For example, it is not acceptable to claim that because a particular culture has always beaten children to instil discipline, their best interests are served by its continuation. Similarly, female genital mutilation cannot be defended as a traditional practice serving girls’ best interests by enhancing their marriage prospects, or maintaining the values of the wider community. It clearly represents a rights violation, and is contrary to the child’s interests in terms of health, survival, emotional well-being, dignity, and protection from violence and harm.
A commitment to the best interests of the child demands that health services adopt explicit policies to protect and promote the rights of children above those of their communities when those rights are in conflict. Of course, the way in which this is done needs to be sensitive to the concerns of that community and, wherever possible, explore approaches, which can be accepted by the majority of its members.
Can you recall a situation where you have had to deal with competing needs, interests or claims? How did you deal with the situation?
Now that you have learned more about the best interests of the child and managing competing rights and interests, would you deal with it any differently if something similar happened again?
No easy answers can be provided when there are legitimate competing claims. When assessing the best interests of the child and children generally, it is a case of sensitively assessing and comparing different views and different degrees of actual or potential benefit and harm.
2.6 Assessing best interests and competing interests in practice
Activity 2.3: Assessing best interests and competing interests in practice
Read the case study below.
Achen is a 14-year-old girl who goes to see her doctor saying she is getting headaches. During the course of the consultation, she breaks down and says that her father is sexually abusing her. However, she does not want you to do anything or tell anyone. She feels that it will cause more problems. She does not think her mother will believe her, and then she will be even more isolated and unhappy than she is now. And if action is taken against her father, it will destroy the family and her mother will blame her.
- What factors do you need to consider in weighing up Achen’s best interests? Use the table below to write in the factors you need to think about, which include factors relating to Achen’s best interests and the interests of others. Some suggestions have been filled in to get you started. You do not have to complete every box in the table, but try to fill in at least five more suggestions.
| Rights and best interests of a child | Interests of other children | Interests of parents/family | Interests of wider society | |
|---|---|---|---|---|
| Rights in the UN Convention and African Charter | Children have a right to be protected from all forms of violence | Governments should ensure children are protected from violence and abuse | ||
| Views of the child | Achen is worried about the impact on her family | |||
| The child’s other needs | Achen may provide support in the home which includes looking after younger children | |||
| The child’s immediate and long-term interests | Taking visible action in one case may deter others from committing offences |
- Once you have added at least five more suggestions of factors you need to consider, look at all the information in the table, comparing different degrees of potential benefit or harm. In this situation, what action will be in Achen’s best interests?
Compare you answers with the table at the end of the study session.
2.7 What is meant by ‘non-discrimination’?
Human rights apply equally to every child. No child must be discriminated against on any grounds. For example, it is not acceptable to say that the right to education for children with disabilities is less important than for other children. It is also not acceptable to allow different levels of funding for services for one ethnic group over another. Children who are stateless or refugees or asylum seekers have exactly the same rights as any other child – the right to food, shelter, education, and protection, for example.
Discrimination can be defined as any distinction, exclusion, restriction or preference which is based on a particular ground such as race, colour, sex, language, religion, political or other opinion, national or social origin, property, disability, birth or other status, and which has the purpose or effect of removing or harming the recognition, enjoyment or exercise by all persons, on an equal footing, of all human rights and freedoms.
(United Nations, 2009)
The articles in the UN Convention and the African Charter place a clear obligation on governments to respect and ensure the realisation of all rights to all children without discrimination on any grounds.
State Parties shall respect and ensure the rights set forth in the present Convention to each child within their jurisdiction without discrimination of any kind, irrespective of the child’s or his or her parent’s or legal guardian’s race, colour, sex, language, religion, political or other opinion, national, ethnic or social origin, disability, birth or other status.
(From Article 2, United Nations Convention on the Rights of the Child)
Every child shall be entitled to the enjoyment of the rights and freedoms recognized and guaranteed by this Charter irrespective of the child’s or his/her parents’ or legal guardians’ race, ethnic group, colour, sex, language, religion, political or other opinion, national or social origin, fortune, birth or other status.
(From Article 3, African Charter on the Rights and Welfare of the Child)
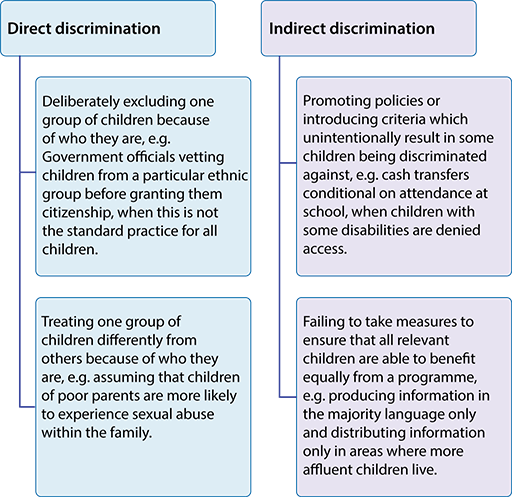
2.8 Different types of discrimination
Discrimination can occur at any level in a society. It can be practiced by governments, by adults against children, by one community against another, or one group of children against another. It can arise from active, direct and deliberate actions, or it can take place unconsciously through insensitivity, ignorance or indifference. These two types of discrimination that arise from either deliberate action or indifference are called direct and indirect discrimination (Figure 2.3). It is important that you understand the difference because they need to be tackled in different ways.
Direct discrimination
This occurs when an action, activity, law or policy deliberately seeks to exclude a particular group of children. In some countries, for example, children with disabilities are classified as either ‘educable’ or ‘non-educable’, the latter being denied the right to education. In many countries, the marriage age, and that of sexual consent, is lower for girls than boys, and children born outside marriage are denied equal rights. Legislation can also discriminate against all children as a group – for example, laws that permit children to be subjected to assault through physical punishment, when the same assault against an adult would constitute a criminal offence. In a recent consultation carried out in Tanzania for this module, young people repeatedly commented that nurses would treat children nicely when they were private patients, but would be rude and disrespectful to others, a clear example of discrimination against poorer children.
Indirect discrimination
This occurs when an action, law or policy has the consequence of excluding or harming particular groups of children, even if that was not its intention. For example, holding clinics in areas where there is no public transport may result in discriminating against poorer children. A health facility would discriminate indirectly against some children with disabilities if it was based in a building that they find difficult to get into. Young people in Tanzania described examples of children with disabilities being removed from health care lists, and a total lack of any attempt to provide accessible facilities, such as ramps or adapted toilets. Without these adaptations, children with disabilities are indirectly discriminated against in their right to health care.
Multiple discrimination
Discrimination can occur on more than one ground, for example, relating to both age and gender, or to both language and cultural background. To give an example, a girl may experience discrimination because of:
- her gender, including low status within her family
- a reluctance to send her to secondary school
- an expectation that she will do domestic chores
- vulnerability to physical and sexual violence.
If she also has a disability, she may suffer further discrimination. A very common form of multiple discrimination arises when children of poor parents also belong to an ethnic or religious group that is already excluded or treated differently. Poverty and other types of discrimination can work together to reinforce exclusion.
2.9 Treating children according to their needs
The principle that children should not be treated differently does not mean that all children must be treated the same. This may seem like a contradiction, but it simply means it is acceptable and appropriate to provide different responses to different children if they have different circumstances and needs. For example, a child with a disability may require a particular service or may require extra time to assess their condition during a medical examination, particularly if they are unable to communicate their needs as well as other children. It would not be appropriate to give all children this extra time because they do not need it. This difference in treatment is very similar to the principle we discussed earlier – the best interests of the child. Different treatment is appropriate when it is in the child’s best interests.
Compared to other children, what specific services might an eight-year-old girl who is a wheelchair user need when attending a clinic?
Are there particular physical, communication or attitudinal barriers that might be encountered?
2.10 Who is protected from discrimination?
If you look back at the box that contains the Articles from the UN Convention and the African Charter, you will see that in the Articles on discrimination there is a list of categories of children who are entitled to protection from discrimination. Children are often discriminated against because of their own or their parents’ or guardians’ race, colour, sex, language, religion, political or other opinion, national, ethnic or social origin, disability, fortune or birth status. That is why these categories are specifically listed in the UN Convention and the African Charter.
However, it is important to note that both the UN Convention and the African Charter include ‘or other status’ at the end of the list of categories. Human nature is such that people will continue to find ways of including or excluding groups of people based on distinctions in how we look or sound, our history and how we behave. The Convention and Charter are clear that no category of distinction permits the denial of any child’s human rights.
Activity 2.4: Children that are particularly at risk of discrimination
Think about the work that you do in your health facility or other place of work.
Are there particular categories of children you see that might experience discrimination and are therefore be in need of protection against discrimination? Try to identify at least three categories of children that are particular to your country or locality.
For each category you have identified, how might discrimination occur? Can you say whether this discrimination is direct or indirect?
Discussion
Your list might include children with disabilities, street children, children from some ethnic backgrounds, children from families of particular religious groups, or girls and young women.
If you thought about street children, a specific issue is that they could be refused access to a health centre because they are unwashed. The policy to stop unwashed children from entering the health centre will result in indirect discrimination against street children, preventing them from accessing health services that are important to their needs and the fulfilment of their right to health.
In some East African countries, a category of children that are particularly at risk is albino children, who have a genetic condition that causes a deficiency of melanin pigment in the skin, hair and eyes, resulting in a pale complexion and little protection from the sun’s ultraviolet rays. Many albino children in East Africa continue to be feared and even murdered for their body parts which are used in medicine believed to cure a wide variety of ailments. Albino children in Tanzania are often forced into exile. This form of extreme treatment is direct discrimination, denying children their right to security, to a family life and the right to participate in the community.
2.11 Applying the principle of non-discrimination in health care
It is important to go beyond an approach that relies on an absence of direct discrimination towards any particular group of children. Ensuring that a service is not discriminatory requires a pro-active analysis of what the service does, how it does it, and who it does and does not include. Consideration can also be given to targeting services towards the most marginalised or vulnerable children. This means designing programmes that explicitly tackle under-representation or exclusion.
The approach shown in Figure 2.4 may help you to review your existing practice or practices in your place of work. It goes beyond preventing discrimination and encourages a pro-active approach to creating an inclusive service that meets different needs, ensuring that all children can realise their rights.
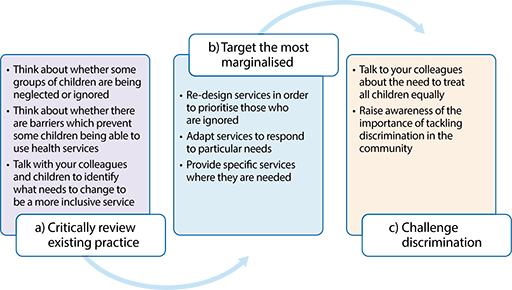
By taking action to prevent unfavourable treatment, to challenge discrimination and to meet different needs, you will be creating an inclusive health service.
Discrimination against children on the grounds of, for example, disability, gender and colour exist in all societies to varying degrees. Some types of discrimination have been identified as particularly serious issues in East Africa. Girls are discriminated against in many ways; for example, if a girl gets pregnant, is the attitude to her the same as it is to the boy who is the prospective father? Also, do girls get the same access to reproductive health care advice as boys?
As you reflected on your work place, you could no doubt identify many examples of discrimination that you have seen. In your health care practice, you may have seen children with disabilities getting a much poorer response from parents or fellow practitioners because they do not feel that their life is of equal value to other children. Perhaps a child with a disability has been refused services on the grounds that their quality of life does not justify intervention. The physical structure of the building or the toilets may prevent some children with disabilities from using the health facility in the first place.
As a health worker, now that you are becoming familiar with the UN Convention and the African Charter, part of your role needs to be in countering this discrimination in the workplace. You can work to ensure that children with disabilities get the same treatment as other children. You could also challenge attitudes and behaviour that are directed towards girls and make sure your own practice is informed by a commitment to children’s rights and non-discrimination.
2.12 Summary
- In all actions concerning a child or children, the best interests of the child is a primary consideration, meaning that it has added weight when weighing the interests of the child against other interests.
- Four different aspects can be actively considered to help you to assess what is in a child’s best interests:
- implementing all children’s rights
- taking account of the views of the child
- balancing different rights
- looking at the short- and long-term interests of the child.
- Children have a right to experience their lives free from discrimination on any grounds.
- There are two main types of discrimination. Direct discrimination arises from active, direct or deliberate action, and indirect discrimination arises from indifference to the needs of particular groups in society.
- In applying the principle of non-discrimination, it is essential to go beyond an approach that simply aims to avoid direct discrimination. Consideration can be given to ensuring the most vulnerable children in the community have access to services and that specific services are set up to meet the needs of particular groups of children.
2.13 Self-assessment questions
Question 2.1
Define what is meant by:
- The principle of the best interests of the child.
- The right to non-discrimination.
Question 2.2
Give three examples of issues to consider in determining the best interests of the child in any particular situation.
Question 2.3
Describe the difference between direct and indirect discrimination.
Question 2.4
List three groups of children who might be discriminated against in your place of work and provide some examples of action that could be taken to address the discrimination
2.14 Answers to activities
Activity 2.2: Balancing best interests of a child with the interests of the parents
- The parents might argue that many girls of her age are getting pregnant, and that it is very easy to get involved in sexual relationships even if you did not really intend to. They want to protect their daughter from getting pregnant and losing out on schooling. They also worry about the stigma of a teenage pregnancy. They might argue that even if the girl does not choose to have a sexual relationship, many girls get sexually assaulted, so can get pregnant against their will. Their view may be that overall, it is better to be safe than sorry. The risks are too high so it is better to be prepared.
- The girl may argue that her parents are showing a total lack of trust in her and undermining her right to make her own choices. She may argue that she has no intention of getting into a sexual relationship, that her education is far too important to her to take such a risk, and that her parents should have a higher opinion of her. She may also feel that the argument that she might be assaulted is a terrible reason for having the injection. If they think she is at risk of being attacked, they should act to protect her not simply act to prevent a pregnancy if it happens.
- Obviously, any decision needs to take account of the specific circumstances of the family in question. However, it is very important to recognise the negative implications of forcing a medical intervention on a girl in her teens that she does not want and that is not needed for clinical purposes. It may well damage her relationship with her parents, undermine her sense of self-esteem and self-worth if her parents fail to trust her or support her to make safe choices. In this situation, it may be in the best interests of the girl to spend time exploring her choices, the risks she might be facing, the implications of all those choices, and then encouraging her to think about what action she feels would be best for her.
Activity 2.3: Assessing best interests and competing interests in practice
- We have completed more of the table below.
| Rights and best interests of a child | Interests of other children | Interests of parents/family | Interests of wider society | |
|---|---|---|---|---|
| Rights in the UN Convention and the African Charter | Children have a right to be protected from all forms of violence Children have a right to live with their parents, unless it is bad for them | Families have a responsibility to direct and guide their children | Governments should ensure children are protected from violence and abuse | |
| Views of the child | Achen does not want to tell her mother as she is worried about the consequences in the short term | Achen has not considered the interests of other children | Achen is worried about the impact on her family | Achen may be worried about the way others in the community will treat her and her parents |
| The child’s other needs | Achen is suffering from headaches; there may be physical and emotional harm which affect her; her education may be affected | Achen may provide support in the home which includes looking after younger children | Achen’s family may rely on her to carry out work | Achen may perform other roles in the community which are affecte d |
| The child’s immediate and long term interests | Removing Achen from her family will prevent further sexual abuse; if this happens, Achen may also be restricted in how often she can see her mother in future | If action is not taken to prevent further sexual abuse in this case, it may mean that action is not taken for other children in the future | Achen’s mother will need to experience distress in the short-term if she is told; in the long-term she can take action to protect her daughter and other children | Taking visible action in one case may deter others from committing offences |
- Achen has a right to be protected from violence and abuse. It is not clear from the information given as to how long the abuse has been continuing for, but it may be over a long period of time. Abuse is likely to continue unless some action is taken. Achen is very worried about the consequences, including the potential for embarrassment to her family and damaging the relationship between herself and her mother. Her fears may or may not be realised, but even if they are, the need to act to prevent further abuse is an overriding concern. It is in Achen’s immediate and long-term interests that action is taken to investigate and prevent further harm to her, and potentially to other children in the future. Action may include: questioning Achen to obtain further facts, reassuring her that she is not to blame and that she has done the right thing by telling you, reporting the information to a more senior member of staff, recording the information for monitoring purposes, and depending on your position and level of seniority, reporting the information to an external authority, who can investigate the claim.
3 Addressing violence against children
Focus question
How can you support children’s right to protection from violence?
Key words: emotional abuse, neglect, physical abuse, sexual abuse, violence
3.1 Introduction
Many children face violence in their homes, at schools and in their communities. The impact of neglect, physical, sexual and emotional violence and abuse on children is significant. It can damage their health, well-being, growth and ultimately their development into adults able to create strong family and community units. It is important for health practitioners to have an understanding about the factors that are likely to place children at risk of violence, and to recognise key signs and indicators of abuse. In this session you will explore the various forms of violence that may be inflicted on children and consider the impact of such behaviour. You will also learn about the strategies that may be used to prevent and respond to violence in the communities where children live.
3.2 Learning outcomes
At the end of this study session, you will be able to:
- define and use correctly the key words and terms above
- explain the right for children to be safe from all forms of violence
- identify the risk factors for violence against children
- describe the effects of violence on children
- recognise the key symptoms of a child who is a victim of violence
- understand how to conduct an appropriate professional response.
3.3 The right to protection from violence
The legal right to protection
Violence against children happens regardless of where they live, and regardless of their race, class, religion or culture. It is never justifiable. You will know from your study of Module 2 that both national and international law and conventions recognise children’s right to protection from all forms of violence.
The box below contains a quote from the UNICEF Fact Sheet A summary of the rights under the United Nations Convention on the Rights of the Child, and specifically refers to Article 19: The right to protection from all forms of violence.
Children have the right to be protected from being hurt and mistreated, physically or mentally. Governments should ensure that children are properly cared for and protect them from violence, abuse and neglect by their parents, or anyone else who looks after them. In terms of discipline, the Convention does not specify what forms of punishment parents should use. However any form of discipline involving violence is unacceptable. There are ways to discipline children that are effective in helping children learn about family and social expectations for their behaviour – ones that are non-violent, are appropriate to the child's level of development and take the best interests of the child into consideration.
The significance of the right to protection from violence is also reflected in Article 16 of the African Charter, as below:
States Parties to the present Charter shall take specific legislative, administrative, social and educational measures to protect the child from all forms of torture, inhuman or degrading treatment and especially physical or mental injury or abuse, neglect or maltreatment including sexual abuse, while in the care of the child.
Protective measures under this Article shall include effective procedures for the establishment of special monitoring units to provide necessary support for the child and for those who have the care of the child, as well as other forms of prevention and for identification, reporting referral investigation, treatment, and follow-up of instances of child abuse and neglect.
It is clearly agreed that children have rights to be protected from all forms of violence. Therefore there is an important role for those responsible for health care provision in recognising and challenging the abuse of these rights. In the next section Activity 3.1 will help you to think about your own experiences of witnessing violence against children, and to help you understand more about what is meant by violence, and how and where it happens.
3.4 Defining violence
For many children some form of violence is a part of everyday life, and wide cultural acceptance of certain violent practices means that this is often unchallenged. While, for example, rape is universally recognised as a violent and abusive act, opinions on corporal punishment or child labour might vary significantly according to region and/or culture. As a health worker it is vital that your definitions of violence recognise all forms of child abuse.
Activity 3.1: What do you know about violence against children
- What kind of violence against children have you seen or heard about in the area where you live or work? Try to list at least five different examples of violence, and make them as different as you can.
- Who is violent against children?
If you are working in a group compare your answers with a colleague. Do your lists agree?
Discussion
- Violence can happen in many forms, some more obvious than others. The types of examples you could have given might include:
- A father beating his child for urinating in his sleep.
- A mother telling her daughter that she is ugly, worthless and will never marry because she is disabled by polio.
- A girl who has been diagnosed with a food allergy, whose parents continue to feed her the same meals that she is allergic to because that is what they want to eat and they know that she likes the food.
- A teacher regularly degrading a boy in front of his classmates by calling him stupid and using derogatory names.
- A girl giving birth in a hospital being hit by the midwife to stop her from crying out.
- ‘Circumcising’ – performing genital mutilation on – a 10-year-old girl as a rite of passage into womanhood.
- A man having sex with the 13-year-old school-friend of his daughter, with the girl’s apparent consent.
- A teenage boy threatening a younger child to force him into stealing cigarettes.
- A woman, who is paid to care for a toddler while his mother works, leaving him in a pen all day while she attends to her own child’s needs.
- A teacher molesting a young boy who stayed behind for help after class.
- An 8-year-old boy who works full-time looking after his family’s herd of goats.
- It is always possible that violence can come from strangers, and this is a fear held by many parents. However, it is more common for violence to come from individuals in positions of trust, often with a duty of care, who are known to, and maybe even respected or loved by, the children they abuse. They may be parents, family members, family friends, community elders, religious leaders, care workers, criminal justice workers, employers, teachers, health workers or any other adults or young adults in similar roles. One study of sexual abuse found that the offenders are almost always known to the victim; approximately 30% are relatives of the child, most often fathers, uncles or cousins; around 60% are other acquaintances such as friends of the family, babysitters, or neighbours.
The discussion section for the activity above gave a number of examples of violence. Did any of them challenge your own definitions? Do you agree that they all show evidence of abuse? If not, why not? These are important questions because your own views on violence and abuse will effect on how you respond to incidents of violence and abuse to children. Activity 3.2 will get you to look at this in more detail.
Activity 3.2: Your own attitudes on violence towards children
Take some time now to think about your own attitudes on violence towards children. Make a few notes under each question. If you are working with others compare your notes with your colleagues.
- Are there circumstances in which you believe some forms of abuse are acceptable, for example for cultural reasons or corporal punishment in the home or classroom?
- How has your understanding of abuse changed according to your personal development, change of circumstances (e.g. becoming a parent or looking after an aging relative) and your professional practice?
- Do you have any difficulties working with the definitions of abuse that are described by the UN Convention on the Rights of the Child and the African Charter?
Discussion
Your views have been shaped by your own upbringing and cultural beliefs and are likely to change over time with new life experiences. But we can all question our own views. For example just because something like corporal punishment is the common way of disciplining children does not make it acceptable. If you believe children need to be beaten regularly you will not be able to help them achieve their right to be protected from violence. Taking children’s rights seriously challenges all societies to think about how they treat children and question what is positive and what is harmful. By adopting the international treaties and passing laws to protect children from violence your country is trying to adapt views, behaviour and practices to reflect what we know about the harmful effects of violence against children. If you have studied Module 2 you could look back at how the law in your country clearly supports work against violence and abuse. Front-line workers like health practitioners are crucial in achieving this change – but questioning some of your own views might need to come first if you are to help children achieve their rights.
In the box below are the examples that were described in Activity 3.1: What do you know about violence against children, may be easier to recognise as abuse if we think about them under the four key headings that are generally used to categorise violence:
| Category of violence | Example | General definition |
|---|---|---|
| Physical abuse |
| Physical abuse covers all physical contact directed at a child with the intent to intimidate, injure or otherwise cause physical suffering or harm. |
| Sexual abuse |
| Sexual abuse of a child covers any behaviour by any adult or older adolescent towards a child that stimulates either the adult or child sexually. This often involves direct physical contact, but also takes place as indecent exposure, conversation on a sexual theme, sharing of pornography or using a child to make or produce pornography. Apparent consent should be treated with caution as children may be in situations where they do not feel they can say no. |
| Emotional abuse |
| Emotional abuse is any kind of behaviour that is designed to control and subjugate a child through the use of fear, humiliation, and verbal assault. It can include anything from verbal abuse and constant criticism to more subtle tactics such as name-calling, belittling, intimidation, manipulation, and refusal to ever be pleased. |
| Neglect |
| Child neglect is the persistent failure to provide a child with necessary care and protection including adequate shelter, food, clothing, sanitation, medical care and education, as well as the failure to protect a child from physical and emotional harm or danger. Lack of appropriate supervision, especially for young children, for extended periods of time is also classed as neglect. Neglect may also occur during pregnancy, for example as a result of maternal substance abuse. |
Key points to remember:
- Not all abuse involves physical violence.
- Not all abuse involves the victim exhibiting obvious or immediate distress.
- Most abuse is inflicted by someone the child knows.
3.5 Risk factors for violence
Since ancient times there have been records showing that children have suffered abandonment, cruel and humiliating punishment, sexual abuse, neglect, and even murder and other violence from adults. This has occurred in every country in the world in a whole range of forms and settings. All children, everywhere, are vulnerable to abuse of any kind but research finds that certain conditions increase the risk factors.
Figure 3.1 below shows a model that demonstrates the layered nature of the risk factors for violence. This is known as an ‘ecological model’ which shows how an individual person is influenced by lots of other factors in their family, the community and the wider society.

We can perhaps understand this diagram in relation to risk better by grouping some of the most commonly recognised risk factors within each of the layers of the model (Figure 3.2). You might want to adapt the model to take account of your particular community and context. Obviously the specific risks will vary in different situations.
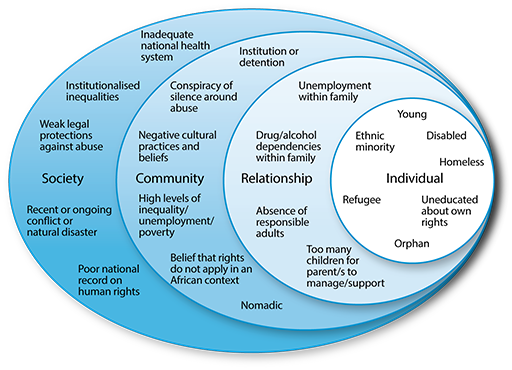
By looking at this model, you can begin to see the factors that expose children to risk of violence can take place at many levels. For example, a child may be more vulnerable because he or she has a disability (individual level). However, the risks will be much greater if the family is very poor (relationship level), the community has negative views towards disability (community level) and the government has failed to provide any protective laws and services to ensure that families with a disabled child are properly supported (society level).
The most powerful factors in the protection of children are:
- the development of strong bonds of attachment between parents and children
- the building of positive relationships within loving, safe and stable family units
These need to be supported by:
- communities that recognise and nurture the rights of their children within positive cultural norms
- societies that have a strong legal framework to reject all forms of abuse.
Together these conditions provide the wider layers of protection that help minimise the risks for violence.
Activity 3.3 will help you see the connections between the layers in deciding how much a child is at risk.
Activity 3.3: Prioritising risk factors
Rearrange the following list in order of risk, so that the child at greatest risk of abuse is at the top, and lowest risk is at the bottom. Consider each case as it applies to the same 10-year-old boy.
If you are working with colleagues – discuss each one in turn and see if you can agree.
Make notes explaining why you think each situation is risky or less risky.
- A boy living with his parents in a refugee camp.
- A boy living with his parents in the same village as his grandparents and other extended family.
- An orphan boy living and working on the street.
- A physically disabled boy living with his parents in a refugee camp.
- An orphan boy living in a children’s home.
| Which situation? | Why is this situation risky or less risky? |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
Compare your answers to those at the end of the study session.
3.6 Effects of violence
Children and adolescents feel the effects of violence and neglect in ways that range from mild symptoms to debilitating and life-threatening conditions. In the same way that the risk of violence comes from a combination of influences, so the child's circumstances (both negative and positive) will affect their vulnerability or resilience to the effects of violence. Factors that influence the effects of abuse include:
- the age and developmental status of the child when the violence occurs
- the severity of the abuse
- the frequency and duration of the abuse
- the relationship between the child and the perpetrator
- the type(s) of violence and neglect.
You might remember these definitions from Module 1 Session 1:
Vulnerability: being more easily physically, emotionally, or mentally hurt, influenced, or attacked.
Resilience: the process of adapting well in the face of adversity, trauma, tragedy, threats or significant sources of stress.
In the first section of this session we identified four groupings for violence against children. Let us return to those grouping to consider the effects that children may suffer from each sort of violence.
| Category of violence | Effect of violence |
|---|---|
| Physical abuse | The initial impact of physical abuse is painful and emotionally traumatic for the child. The longer the violence continues, the more serious the physical and psychological consequences are likely to be. Short-term effects are likely to include pain, medical problems, emotional troubles (such as anger, fear, anxiety, lowered self-esteem) and behavioural problems (such as aggression and truancy). Longer-term effects can include physical disabilities and serious emotional disturbance such as depression. |
| Sexual abuse | Much of the harm caused to child victims of sexual abuse only becomes apparent years after the abuse happens, when the victim has become an adult and is struggling to deal with long-term psychological damage. Sexual abuse by a family member can result in more serious trauma, especially in the case of parental incest. The effects of child sexual abuse include guilt and self-blame, flashbacks, nightmares, insomnia, fear of things associated with the abuse (including objects, smells, places, etc.), low self-esteem, sexual dysfunction, depression, anxiety, and physical injury to the child. Victims of child sexual abuse are far more likely to attempt suicide (CDC, 2006) |
| Emotional abuse | Some level of emotional abuse is involved in all types of maltreatment of a child, though it also frequently occurs alone. It can be hard to recognise but the effects on children who are shamed, humiliated, terrorised or rejected are significant. Emotional abuse has been likened to brainwashing in the way that it wears away at the victim’s self-confidence and sense of worth. Other effects of emotional abuse include poor development of basic skills, alcohol or drug abuse, suicide and difficulty forming relationships including friendships with other children. Longer-term psychological and/or behavioural problems include depression, aggression, hostility, lack of attachment or emotional bond to a parent or guardian. It can affect educational achievement and social skills. |
| Neglect | Given that neglect is often found with other forms of abuse, isolating the impacts of neglect alone is difficult. However neglected children, relative to children affected by physical, sexual or emotional abuse, are generally found to experience more severe cognitive and academic problems and social withdrawal. Children who have been the subject of chronic neglect exhibit problems with attachment, cognitive development, social self-confidence, social competence, perseverance in problem-solving. They may experience language delay and health problems due to lack of ensuring medical attention. As with all abuse, the younger the child and more prevalent the neglect, the greater the harm. |
You will see there is some overlap between the effects of different forms of violence and abuse. This is because they are all forms of trauma to the child. The extent of the impact of violence may also be affected by the length of time for which it has been experienced by the child.
3.7 Responding to violence
Recognising violence
Cultural norms around abuse vary significantly between countries and regions, but as with all issues relating to child rights it is the right of the child (in this case to protection from violence) that should be considered first and foremost. For example the line between physical abuse and corporal punishment or discipline is often considered hard to define, however, the UN Committee on the Rights of the Child has stated that the right to protection from violence covers the issue of corporal punishment for children and therefore all corporal punishment is unacceptable.
Professionals who support the cultural norms that sanction physical punishment, or indeed any other form of culturally sanctioned abuse such as harmful child labour or early marriage, are effectively approving or condoning child abuse. Protecting children from violence is not only an issue of rights, but research shows that it has the potential to reduce all forms of violence in society. This makes sense when we reflect on the previous section and what it tells us about the long-term effects of all forms of abuse including the impact on the behaviour of adult survivors of childhood violence.
Health workers and teachers are the two professional groups of adults that most children are likely to encounter regularly. This makes you the front line of defence beyond the adults within the child’s family. A parent or carer may have experienced violence or abuse in their own childhood and may not know about their own rights or the rights of their children. They may know that violence or abuse is happening to their child, but assume that this is a normal part of growing up. Even if they believe that the violence or abuse is wrong, they may not know how to protect their child. Sometimes they will be the actual perpetrators of abuse. Children themselves may not have the information they need to know how to protect themselves or how to report or challenge abuse. So it is vital that you as a health worker recognise your responsibility and duty to act in order that the appropriate agencies can investigate and take any necessary action to protect a child.
As part of this process it is helpful if you are alert to the possible signs of abuse. Sometimes it may be obvious, but often children will be reluctant to say anything and it is up to practitioners like health workers to notice the signs. Every case of abuse is individual and unique and there is no definitive list of signs or indicators. However, there are many generally recognised indicators that should alert you to the possibility of violence and abuse. There is a list of these as a resource for you to consult at the end of the session.
Look back at the examples of violence that you studied in Activity 3.1. You can look at each of these and use the resource list combined with your own experience to think about the likely signs of each type of abuse. In the table below there are three of these examples: one of physical abuse, one of sexual abuse and one of emotional abuse with some of the potential signs of violence alongside.
| Violence / Abuse | Examples of possible indicators |
|---|---|
| A father beating his son as punishment for having urinated in his sleep |
|
| A man having sex with the 13-year-old school-friend of his daughter, with the girl’s apparent consent |
|
| A teacher regularly degrading a boy in front of his classmates by calling him stupid and using derogatory names |
|
Responding to violence
Some professionals such as doctors and nurses may be legally obliged to report suspected child abuse. It is essential that you find out what your own responsibilities are within your specific role as a health worker. If you have studied Module 2 you will already have found out this information. If not you need to know:
- Is there a procedure for reporting?
- Is there a child protection committee?
- Which other colleagues can you consult with?
- Are there other appropriate services or people in the community who should be consulted?
If you believe there are signs of violence and abuse to a child then any response you make should prioritise the child’s safety and well-being. In a situation where a child is in immediate physical danger then your response should be equally immediate in acting to separate the child from the situation.
You should respond sympathetically and listen to what the child is saying. Do this sensitively and with respect for the child’s or young person’s need for privacy and confidentiality. They may have important information that may help decide what happens next. It may be appropriate to talk to the parent or parents, but only if you believe it will not jeopardise the safety of the child or young person. In most cases it is logical to gather information and facts according to what you know and have observed.
Ultimately the action that you take will be dependent on the many variables and the practical options that are available to you, but it should always be driven by the child’s right to be protected from being hurt and mistreated, physically or mentally.
A proactive approach to violence
Finally in this section it is important to think briefly about what you can do to prevent violence against children. Much of this approach is about education – for example the fact that you are working through this study session indicates that you are taking a proactive stance in the prevention of violence against children. You can now share that education by working with your patients and their communities as an advocate to raise awareness and promote non-violent values in their everyday lives. There are many opportunities to share your learning, for example in the way that you talk one-to-one with a parent about how they discipline their child, or you may run a campaign or other wider awareness-raising activity. You could work with your organisation and with other professionals (for example in law and/or education) to create accessible and child-friendly reporting systems and services. You should consider a child protection charter for your own health facility. (This is discussed in Study Session 4 of this module.) You could include children in the consultation for any education and measures of prevention so they are educated in their own rights, and not solely dependent on adults to advocate on their behalf. Try to develop and promote health services and systems that are accessible, child-sensitive and accountable. Where possible implement or support research efforts and the collection of systematic data that can contribute to a bigger picture of education about violence against children. (More information on how to do this can be found in Module 5.)
Activity 3.4: Flo and her mother
Read the case study below and answer the following questions.
- Can you identify any of the risk factors or protective factors in this case using the ecological model you looked at in Section 3.3 of this study session?
- What positive interventions did Damtew make in this case?
Flo is 13 and lives with her mother, Hanna, and five younger siblings. Flo used to go to school, but last year her father died of HIV and so she had to stay home and support her mother in caring for her brothers and sisters.
Damtew is the community health worker who has responsibility for Flo’s village. He met Flo one day when she walked 3 miles carrying her little brother to the clinic outpost for medical treatment. She had no money and was desperately worried about the little boy. Damtew found her waiting at the end of clinic hours and took them both in for a consultation. Fortunately the treatment for the little boy was very simple, but Damtew was more worried about Flo. She was clearly tired and malnourished and showed signs of abuse in the bruises he noticed on her upper arms. He asked some careful questions and learned about the family circumstances, and that Flo was very proud to be helping her mother to care for her siblings. Damtew sent her home, but made a note to discuss her situation with his colleagues.
A week later, Damtew had the opportunity to discuss Flo and his concerns with another health worker. He talked about the risk factors for abuse, and the physical signs he had observed. Damtew’s colleague suggested that he talk to one of the community elders who live in Flo’s village.
The next day Damtew had cause to go to the village, and was able to meet with the community elder, Yared. They discussed Damtew’s concerns, and Yared was able to provide some more background information. He had observed that Flo’s mother worked very long hours to support her family financially, and sometimes she beat Flo out of tiredness and frustration. Damtew and Yared agreed a plan and went to visit the family that evening. They asked to speak to Flo’s mother alone, and Yared began by talking about how Flo’s father was missed within the community, and how difficult it must be for Hanna to manage the family without him. Hanna began to cry, and they talked for a long time about all her daily challenges and how much she loves her children and wants the best for them. She knew that Flo was giving most of her food to the younger children, and was missing her education, and this contributed to Hanna’s frustration that led her to hit Flo when they argued.
Yared suggested that Flo and the older children be allowed to go to school, leaving just one child to be cared for during the day. Hanna’s mother would be able to cope with the little one, and a social programme at the school means that the children would all be fed a hot meal for free at lunchtime. Hanna agreed to the plan, and Damtew exacted a promise from her that she would stop beating Flo.
Mostly the plan has worked very well. Flo and the other children are at school and Hanna’s mother, who would not have been able to cope with all of them, is very happy looking after the baby. Hanna is still very tired and often frustrated, but Damtew made sure one of the teachers at school is looking out for Flo and Hanna has so far not beaten her again. Sometimes Flo stays home if one of the other children is sick, because someone has to care for them while Hanna works, but if they are absent for more than 3 days the teacher will come to visit and lets Damtew know if treatment is needed.
Thanks to Damtew’s careful intervention, Flo is no longer suffering neglect or physical and emotional abuse, and remains living happily with her family.
Compare your answers to those at the end of the study session.
3.8 Summary
- Violence and abuse towards children is widespread but it is a fundamental right for children to be protected from violence and abuse.
- For health workers to be effective in contributing to the protection of children you need to be aware of the risk factors, the signs and the effects of violence and abuse.
- It is important that children are listened to and their views are taken into consideration in finding a solution.
- It is vital to know how to report concerns you have about children and know the system for reporting.
3.9 Self-assessment questions
Question 3.1
Identify one article in the UN Convention and one the African Charter that establishes the right of children to be free from violence and abuse.
Question 3.2
What are the four ways in which violence has been defined in the study session?
Question 3.3
Working in a health setting, how should you respond if you see a child with injuries that you believe have been caused by violence at home?
3.10 Answers to activities
Activity 3.3: Prioritising risk factors
We put these children in the following order for risk:
| Which situation? | Why is the situation risky or less risky? |
|---|---|
An orphan boy living and working on the street | The orphan boy who lives and works on the street is likely to be at greatest risk because he has to look after himself and is in an environment where he is unlikely to have any community support. He is already suffering abuse as he is engaged in child labour. |
A physically disabled boy living with his parents in a refugee camp | Although this boy is with his parents, he is living in a context that is often aggressive, competitive and full of transient adults. His disability also makes him particularly vulnerable because he may be seen as less valuable than other children, and he may be unable to defend himself and/or escape from his abuser. |
An orphan boy living in a children’s home | This child is living with responsible adults, so his immediate relationship needs should be cared for and the home may be part of an established community. However many children’s homes and orphanages are not well run and can develop cultures of harsh treatment and abuse. |
A boy living with his parents in a refugee camp | This boy is vulnerable to the same challenging community issues as in (2) above, but is at slightly less risk as a non-disabled child. |
A boy living with his parents in the same village as his grandparents and other extended family | The child at lowest risk has the support of his immediate and extended family, and it is likely that he will also be known to the wider community as his family are all established in this location. |
Did you identify the same order? This is one of those activities where there is no single correct answer, and more information could make significant changes. For example what if we now said that the village that is home to the extended family subscribes to abusive traditional practices, such as early marriage and widow inheritance? The circumstances around every child are unique. As a health worker you have a responsibility to consider an individual risk assessment for every child in your care, and recognise the key factors that can make them vulnerable to abuse.
Activity 3.4: Flo and her mother
- You probably easily identified some of the pressures on this family that might add to the level of risk to Flo. The death of the father has had a major impact at the relationships level as it reduces the income level in the family and also leaves the mother with many children to care for on her own. There is a clinic in the community although it is not that easy to get to in order to get help. There would seem to be no formal reporting procedure in place to a child protection committee but fortunately the community does respond positively to the concerns through the elder and the school. This is an important protective factor at the community level.
- Damtew recognises the signs of abuse and violence straight away and decide to take some action. He talks to the child and listens carefully to her explanation. Damtew then speaks to the right people in the community to negotiate a solution and a plan is set up to protect Flo in the future.
4 Child-friendly health facilities and standards
Focus question
How can you create a child-friendly health facility?
Key words: children’s charter, child-friendly, child protection, standards
4.1 Introduction
Creating a child-friendly environment is a very important part of promoting children’s right to have the best possible health and well-being. Health facilities can be designed to promote children’s rights to express their views, support their best interests and be non-discriminatory. As a health worker you can address barriers that obstruct children’s access to effective health services in the environment in which you work.
In this session you will learn about the value of a child-friendly environment in health service delivery. Such an environment can be created by training staff to be child-friendly, providing facilities, such as play rooms where feasible, and promoting child-friendly attitudes. This session will explore how establishing protocols and standards can also help to create the right environment.
Not all measures to establish a child-friendly service require resources – sometimes all it takes is a change of attitude and personal commitment.
4.2 Learning outcomes
By the end of this session you will be able to:
- explain the meanings of the above key words
- describe a child-friendly environment in relation to health service delivery
- list ways in which you could make your facility child-friendly
- understand the importance of standards in delivering a child-friendly health service
4.3 What does the term ‘child-friendly health services’ mean?
A child-friendly health service provides an environment for children where they feel safe and respected rather than threatened or unnecessarily worried. Health care providers, organisations and individual health care workers, share a responsibility to reduce the anxiety and suffering of children and their families. The services should be accessible, free or easily affordable, and should be guided by procedures that specifically address the needs and rights of children. They should allow children to participate in diagnosis, treatment and prevention of situations that might put them at risk. Child-friendly health services should provide appropriate information for children to be able to know how to access the service and give feedback on their experiences.

What do children say?
Research undertaken in Tanzania with children and young people for this module clearly revealed that many children experience unfriendly and unhelpful responses when they visit health facilities. The older boys in the research said they go on their own to get medical attention but the doctors disregard them. They can stay for a long time without being seen by anyone and are called truants if they turn up in school uniform. The following quotes are real examples of their experiences.
At school I got a sudden headache. I went to the nearby clinic but they ignored me thinking I was playing truant. When I went home to inform my mother, she was out. As my condition was getting worse I had to go to my sister. When I told her she took me to the hospital run by nuns who admitted me with serious malaria. My sister then called my mum to tell her I had been admitted. What would have happened if I did not have a sister? Since mum is at work, I could have died… just because they ignore children.
(From the consultation undertaken in Tanzania for the development of this module)
I had forgotten that my meds were finished and my grandmother did not remind me. When I got to school, I remembered and went to the dispensary where I usually take the meds. I left at 9 in the morning but no one was concerned until I was the only person left. Then they turned to me and asked, ‘You, child, what do you want? Why aren’t you speaking?’ When I told them I had come for my meds because I didn’t take them, they told me ‘Come with your grandmother’. It was 1 o’clock and I was so hungry but I had to go back to my grandmother and come back with her.
(From the consultation undertaken in Tanzania for the development of this module)
It is clear that some children and young people suffer very poor experiences at health facilities (which in turn can actually endanger their health). It may be that you think the two young people would not have this experience where you work. If they would then now that you understand children’s rights and their importance, you can adapt your own practice and challenge the practice of others where necessary.
Many health facilities are very busy and under-resourced but being child-friendly is not just about resources. Research that was done in many countries around the world concluded that:
Even in the most disadvantaged health facilities there were many examples of excellent care, but everywhere there was care that can only be described as very child-unfriendly.
…it is usually more dependent on the health workers responsible than on the resources available.
(Nicholson and Clarke, 2007, p. 14)
A well-resourced city hospital may be very frightening for children because of the environment and attitudes of the staff. A poorly resourced rural facility could be a model of supporting the rights of children if staff have made efforts to make children feel safe and at ease.
Activity 4.1: Case study – An unaccompanied child
A young boy is brought into a clinic by a man. The man says to the nurse on duty that he found the child crying on the road near the clinic. The child looks sick and possibly neglected and he thinks that he should bring him to the health facility. He wants the staff to help the child and take him back home. The child is about 7 years old and is able to talk. The staff at the health facility insist they cannot help the child without the parents or guardians being present.
Questions:
- As a health practitioner how would you go about helping this child given the fact that he was unaccompanied?
- Who else would you involve in managing this case?
Discussion
- In health facilities, health workers should be easily accessible to children whether accompanied or not. Health workers should always take the best interest of the child as paramount, checking on their circumstances and establishing their health status and other related issues that affect the child’s well-being. It is important to involve a young child’s family where appropriate but this should not prevent help being given at the time. The health workers should develop an attitude of making children who come to their facilities comfortable, and help children to express themselves.
You will know from your study in the last session that children sometimes come to health facilities when they have been abused and neglected by their parents, guardians and those with whom they stay. According to the laws in your country, health workers are very important in identifying abuse and neglect and reporting this to the relevant authorities.
- As a health worker you can also involve others beyond the immediate care of the child, both other practitioners and social workers or psychologists if they are available. If there is a problem that requires work with the community, you can approach the community leaders and work with them to trace the parents or resettle children like the one in the case study. The community can be supported in ensuring that cases of neglect by parents/guardians can be prevented and that the well-being of children in such communities can be promoted.
4.4 What is your own health facility like?
This session is an opportunity for you to review your own service and consider how it might be improved to give children a better and more valuable experience of health care. This means that you need to see your workplace in a different way – from the point of view of a child. Also you can draw on the work you have done in the previous sessions in this module about a child’s right to express their view, not to be discriminated against and to be safe. Putting all of these issues together can make a big difference to the quality of health care for children.
Activity 4.2: From the point of view of a child – how child-friendly is your health facility?
Try to put yourself in the place of a child. How child-friendly do you think your own facility is in terms of the following:
- The physical environment
- Attitudes of the staff towards children.
The type of questions to consider are:
- Is it accessible to disabled children?
- Do disabled children get the same level of service as non-disabled children?
- Is there anywhere for children to play or anything to play with?
- Is there information available for young people to read in a format and written at a level that they can understand easily?
If you are working in a group spend time comparing views and experiences. You can also discuss these questions with colleagues in your own health setting.
Discussion
The answer to some of these questions will vary depending on where and what kind of health facility you work in. However as we discussed earlier there is no direct connection between the type of facility and it being child-friendly. Hopefully you identified some positive aspects of your workplace and it is important that examples of good practice are shared. However, if this is not an issue you have considered before there may be lots of things that could be improved. For example the children in the Tanzania study said that their hospital had stairs and pit latrines that were a big problem for disabled children.
I have not seen any dispensary or hospital with special toilets or ramp for people with disability.
(From the consultation undertaken in Tanzania for the development of this module)
In the same study, attitudes, which require no extra resources, were also a problem:
They look down on children with a disability, as if they do not have the same rights.
(From the consultation undertaken in Tanzania for the development of this module)
Now that you have spent time thinking about this issue it is important that you translate your views into action. Activity 4.3 asks you to identify some specific changes you could make where you work.
Activity 4.3: Identify three changes
Now you have looked again at your workplace, identify at least three changes or improvements you could make. These might be about your personal practice or the setting in general. If you are working in a group, discuss and share your ideas and suggestions:
Discussion
Simple suggestions can sometimes make a big difference. The health facility should always take the best interest of the child as paramount – treating them as a priority and ensuring that children have been given an opportunity to express themselves.
You will do an activity later in the study session that looks at areas of practice in your health centre in more detail.
4.5 What are child-friendly health standards?
A good way to ensure the development of child-friendly heath care is to develop child-friendly health standards. This should be done with the participation of everyone at the health facility and ideally also with members of the community, including children. This will help to ensure that the standards are accepted by everyone.
Creating standards and protocols in your facilities that promote respect for children, is a way to support improving the well-being of children. Health workers can ensure that guidelines and standards for promoting respect for children in the health facilities are established and followed. There are both international and national standards in health care systems that can be used to develop your facility-based standards for children. In the next section we will explore different standards and guidelines that can be established to improve the experience of children in health facilities.
Child-friendly standards are the minimum requirements necessary for enabling a child to access services in a health facility without discrimination and in a safe and friendly environment. They help to ensure that through awareness, good practice and robust systems and procedures, staff and other representatives are able to keep children safe and can access health services without any inhibitions. Child-friendly standards can work hand-in-hand with a child protection policy and, as you will see later, with a children’s charter.
Why should you implement child-friendly health standards?
- To ensure that children can access health services in safety.
- To protect and advocate for children’s rights.
- To ensure that staff and other representatives are competent and committed to protecting the best interest of the child while accessing health services.
- To maintain the reputation and credibility of your individual facility.
The Child-Friendly Healthcare Initiative developed a set of standards for health care facilities. They can be used as standards against which health facilities can identify positives, gaps and improvements. The standards below are all supported by articles in the UN Convention and the African Charter.
‘Child-Friendly Healthcare’ is the best possible integrated health care provided by health workers to minimise the fear, anxiety and suffering of children and their families by supporting and practicing the following 12 standards:
- Keeping children out of hospital (and other health facilities or institutions) unless this is best for the child.
- Supporting and giving the best possible health care.
- Giving health care safely in a secure, clean, child-friendly environment.
- Giving child-centred health care.
- Sharing information and keeping parents and children consistently and fully informed and involved in all decisions.
- Providing equity of care and treating the child as an individual with rights.
- Recognising and relieving pain and discomfort.
- Giving appropriate resuscitation, emergency and continuing care for very ill children.
- Enabling play and learning.
- Recognising, protecting and supporting vulnerable or abused children.
- Monitoring and promoting health.
- Supporting best possible nutrition.
Activity 4.4: Using standards
You could consider reviewing all 12 of these standards and apply them to your workplace but for this activity, take just three: standards 4, 5 and 9.
What examples or evidence do you have of how your environment currently meets these standards?
What might need to be done to improve?
Record your answers in the table.
Take the ideas into your workplace to discuss with colleagues.
| Standard | What happens now? | What needs to be done to improve? |
|---|---|---|
| Giving child-centred health care |
|
|
| Sharing information and keeping parents and children consistently and fully informed and involved in all decisions |
|
|
| Enabling play and learning |
|
|
Discussion
Using these standards is another way of promoting change in health care practice. You may think you are already good at some of these areas but some of the others could be improved. There are no right or wrong answers to how you can improve but some suggestions include:
Giving child-centred health care:
- a welcoming attitude to children
- allowing parents to stay with children in hospital
- named nurses – in other words, when a child goes into hospital, they are given the name of a nurse who will have special responsibility for them.

Sharing information and keeping parents and children consistently and fully informed and involved in all decisions:
- involving children and parents in explanations about their health problems and treatment
- helping children and families understand what to expect. This should help reduce fear and anxiety
- explain how the child or the parents can provide feedback on how they felt about their care, or make a complaint if there were problems.
Enabling play and learning:
This recognises children’s right to play (Article 31) but can also contribute to a reduction in fear and play an important role in helping children recover.
- Where there is space, have a separate clean area for children to play.
- If children are in hospital and missing school, provide the opportunity to read or have access to educational materials.

4.6 Protecting children
Another important standard from the list above is number 10: protecting and supporting vulnerable or abused children. In the session on violence and child protection you covered your role in identifying violence and abuse in the community and in reporting. Here you are continuing the theme by considering protection for children within health facilities.
Children are not always safe in health facilities as this quote from a child participating in the Tanzania study indicates:
Fondling girls is very common (by health workers) and we don’t like it.
(From the consultation undertaken in Tanzania for the development of this module)
While the majority of health workers will act appropriately towards children, clear and agreed standards will help protect children and young people from exploitation or harm. There may also be many other people who are not health workers who are able to come in and have contact children and young people. Many workplaces have a child protection policy which lays out the procedure staff should follow in some detail.
What is the purpose of child protection standards?
- To raise awareness of the problem of child abuse and the risks children may be exposed to.
- To provide a framework for everyone working with children to effectively protect them from abuse.
- To outline clear actions to be taken when abuse is suspected.
What are the advantages of implementing child protection standards?
- Children are protected, which minimises risks of abuse and exploitation.
- Agency representatives are protected – clarity on expected behavior with children and what to do if there are concerns about the safety of a child.
- The organisation is protected – commitment to keep children safe deters potential abusers from joining it.
An example of a list of standards is provided below. You could use it to help you develop or improve the child protection standards of your own facility.
Example of child protection standards
The following standards are adapted from: Keeping Children Safe: A Toolkit for Child Protection, Keeping Children Safe, 2011.
In our health facility we will ensure that we:
Standard 1 Have a written policy on keeping children safe.
Standard 2 Have clear procedures for putting the policy into practice.
Standard 3 Do everything we can to prevent harm to children.
Standard 4 Follow the written guidelines on how we behave towards children.
Standard 5 Meet the standards in allocations where we work.
Standard 6 Protect children equally, regardless of any differences they have.
Standard 7 Actively communicate ‘Keep Children Safe’ message.
Standard 8 Educate and train our staff on child protection.
Standard 9 Provide children with access to advice and support.
Standard 10 Monitor the implementation of these standards.
Standard 11 Promote these standards with the partners we work with.
4.7 A children’s charter
Standards are important to measure how a hospital or health centre is achieving appropriate rights-based child-friendly care. Sometimes standards are not written in very simple language and it may be helpful to convert the key principles behind a list of standards into a more specific and easily understood ‘charter’ suitable for your location. This can make the standards easily understood by children themselves and make a clear link to children’s rights. For such a charter to be successful it is important to create one that is agreed on by practitioners and members of the community, including children.
Activity 4.5: Developing a charter
1. Think about developing a charter for children for your health facility. Add at least three points to the list below.
2. How would you go about involving children in drawing up a charter? Share your ideas if you are working in a group.
Children’s Charter
If I am seeking, needing or receiving health care I have the right to the following:
- I have the right to the best possible treatment and care.
- I have the right to be listened to and taken seriously.
Discussion
From your work in the previous sessions on ensuring that children are enabled to participate you will know that given the opportunity children are perfectly capable of expressing their opinions. So, if the purpose is made clear and you use appropriate engagement methods, then children will be able to contribute.
If you have access to the internet there are lots of materials that have been developed to involve and consult children.
www.child-to-child.org/resources/index.html
Also, Save the Children: So you want to consult with children? A toolkit of Good Practice
www.savethechildren.org.uk/resources/online-library/so-you-want-consult-children-toolkit-good-practice
You will see in this example that the language is fairly simple to try and make sure the charter is easily understood by children. It would obviously need to be in an appropriate language. You could get a small group of children to work with you on writing a charter or children who visit could be encouraged to contribute things they would like to see included. Perhaps children could survey other children and draw up a list. A proposed charter could be tested out with the children in the community. You will probably have had lots of other ideas which you can share with your colleagues. The understanding of older children might be helped by seeing a simple version of the UN Charter (see Unicef, n.d.). In this way you can help children learn about their rights.
This kind of charter should be prepared with the involvement of other staff and preferably with people in the community so that everyone accepts and works with it. It is also likely that you would need to get the agreement of the managers to have the charter displayed on a wall and used actively in other ways at your practice.
For some suggestions to add to the charter see the list below:
An Outline for a Charter of Children’s Rights
If I am seeking, needing or receiving health care, I have a right to the following:
- I have the right to the best possible treatment and care.
- I have the right to be listened to and have my views taken seriously.
- I have the right to be given information that will help me understand my treatment.
- I have the right to ask for advice, information and support.
- I have the right to be asked before anyone touches me.
- I have the right to respect for my privacy.
- I have the right not to suffer unnecessary pain.
- I have the right not to be hit or abused.
At a children’s hospital in South Africa, a project was introduced to create a space to hear from children directly about their experiences in hospital. Children were provided with an opportunity to share their fears, concerns and hopes through a variety of methods including drawing and painting, making and talking through puppets, as well as group discussions. By listening to the children, it was possible for staff to gain a far better understanding and insight into how the children were feeling. Children highlighted, for example, their fears at night when sleeping alone in a bed in a large ward, their sadness when family members failed to visit, their desire for someone to talk to, the need to be able to play. The children identified simple strategies to improve the quality of their hospital life – having a favourite toy from home, photos of family members to look at when they were unable to visit, a commitment to celebrating birthdays, nurses available at night to provide comfort, and someone to talk to when they were feeling lonely or unhappy. These small changes can be achieved at little cost but with enormous impact on the overall well-being of the children.
If you have access to the internet you might be interested to look at the video link to this South African project. It might help you do something similar in your own hospital to begin to find out what children might want to include in a charter of their rights.
Activity 4.6: Plan a charter for your workplace
Either on your own or in a group, decide on a plan to introduce a child friendly charter in your workplace. Include how you will involve children, families and other health workers in making one.
Although this session has provided some examples, every charter will be different if many people are involved in contributing to it. To finish the session make a plan for creating a charter for your own workplace and discuss it with your colleagues. Plan how you will involve children and make it meaningful to improve their experience of health care. There are other references at the end of the session that you could use if you have access to the internet.
4.8 Summary
- Making health settings child friendly is a vital part of helping to ensure that children are treated in accordance with their rights.
- Sometimes extra resources are needed but mainly it is a matter of reorganising the physical environment and changing attitudes.
- Achieving a child-friendly environment can be supported by using standards and charters.
You can use the information in this study session to think about your own health environment and plan changes to make it more child-friendly.
4.9 Self-assessment questions
Question 4.1
Give three examples of what makes a health facility child-friendly.
Question 4.2
List three reasons why standards and charters can be important in establishing a child-friendly environment.
5 Answers to self-assessment questions
Study session 1
Question 1.1
Some benefits of children’s participation for the child are:
- Involving children in their own health care makes children feel more respected, and less vulnerable.
- It helps relieve anxiety and enables children to cope better with treatment.
- It gives them confidence that actions will be taken without their knowledge or understanding.
Some benefits of child participation for the health professionals are:
- It will help you understand the child’s condition better, and enable you to treat them more effectively.
- It encourages co-operation, as children are likely to be less frightened and therefore more willing or able to co-operate in treatment. This, in turn, makes interventions more painful and distressing.
- It encourages children to take more responsibility for their own health because they develop a better sense of the causes and consequences of their actions or inactions.
Question 1.2
Evolving capacities refers to the process of children gaining skills, knowledge and understanding as they grow older. As this happens, they are able to take increasing levels of responsibility for decisions that affect their lives. This is relevant in health care as it means you need to think about, for example:
- the way you give information to children
- the level of involvement they have in their own health care
- their growing need for privacy and confidentiality
- their right to take responsibility for decisions about their health care and treatment
Question 1.3
Many objections are raised to children participating for example:
- Children do not have the capacity to participate in their own health care. However, even very small children can tell you what they like or dislike about being in hospital and can produce ideas for making their stay less frightening and distressing. It is necessary for health professionals to explore the many ways that enable the child to articulate these views, concerns and opinions.
- Involving children in decisions burdens them and takes away their childhood. Neither the UN Convention nor the African Charter imposes obligations on children to express their views. Rather, they provide a right for child to do so.
- Participation can lead to disrespect for parents. Listening to children is about respecting them and helping them learn to value the importance of respecting others. It is not about teaching them to ignore their parents. The UN Convention, for example, states that education should teach children respect for their parents. Children should not be led to believe they alone have a right to have a voice; wherever possible, their families should be involved too.
Question 1.4
Your answer in identifying two things will be unique to your own facility but it is vital that you translate this learning into changes in the workplace.
Study session 2
Question 2.1
- The best interests of the child can be understood as the principle that all adult actions and decision-making that impacts on children’s lives must be directed towards promoting and ensuring the well-being and dignity of the child. In other words, children’s well-being must be at the centre of adult decisions and actions at all levels of society. It is a principle that applies to decisions affecting individual children as well as those affecting broader groups of children, or children as a whole.
- The right to non-discrimination can be defined as the right to protection from any distinction or exclusion, based on a particular ground such as race, colour, sex, language, religion, political or other opinion, national or social origin, property, disability, birth or other status.
Question 2.2
Your three options should be represented in this list:
- You should always talk to the child and find out what she or he thinks is important, what is of concern to them, what they want to happen. The child’s best interests should always be guided by the child’s own perspective if she or he is old enough to have a view.
- You need to be guided by the rights in the UN Convention and the African Charter as these treaties were produced to provide the basic entitlements that are necessary for children’s well-being. In other words, the implementation of children’s rights will promote their best interests.
- There may be situations where there is a tension between the different rights of a child. For example, the child’s right to family life may not be consistent with their right to protection from violence, if one of the parents is abusing or violating the child. You would need to decide what would be in the best interests of the child overall – to be separated from the family but ensure the right to protection, or preserve their family life but at the cost of continued vulnerability to abuse.
- There may be situations where the rights of one child are in conflict with those of other children. For example, a child might be infectious with a serious disease. This may mean that although the best interests of the individual child would be to remain with her family with their continued care and support, the best interests of children in the community would be best served by that child being isolated from others.
Question 2.3
- Direct discrimination is when an action, activity, law or policy deliberately seeks to exclude a particular group of people. For example, a law that prevents women from inheriting property, but has no such limitation for men, or a policy that specifically excludes children with disabilities from education.
- Indirect discrimination is when an action, law or policy has the consequence of excluding or harming particular groups of children, even if that was not its intention. For example, a clinic or hospital that fails to provide a ramp to enable a wheelchair user to access the building would indirectly discriminate against children with physical disabilities. Or if clinics are only located in affluent areas, this would discriminate against poorer communities’ access to health care.
Question 2.4
You should already have identified which groups of children you know are discriminated against from your work on activity 2.4. It is important that here you have made a response for each one about action that you can take to address this discrimination.
Study session 3
Question 3.1
UN Convention Article 19 (see also 34)
African Charter Article 16 (see also 27)
Question 3.2
Physical abuse, sexual abuse, emotional abuse, neglect.
Question 3.3
There are lots of possible points here but your answer should have included at least:
- respond sympathetically to the child
- ensuring they are safe form immediate danger
- following the reporting procedure for your workplace.
Study session 4
Question 4.1
There are a lot of examples you could have given here but some of the most important points are
- The attitude of staff – which includes being friendly, reassuring and respectful
- The physical environment – which includes being welcoming and accessible to all children
- Access to information for children and young people on health care and their rights
- Procedures in place that support staff focusing on the rights and needs of children.
Question 4.2
- They can help change practice if everyone agrees to follow the same set of standards.
- They can ensure minimum standards and a more consistent delivery.
- Drawing up a charter can give children the opportunity to participate in changing the environment.
- To ensure that children can access health services in safety.
- To protect and advocate for children’s rights.
- To ensure that staff and other representatives are competent and committed to protecting the best interest of the child while accessing health services.
- To maintain the reputation and credibility of your individual facility.
Bibliography
ANPPCAN Uganda Chapter, Protecting Children from Abuse and Neglect: Tips and Skills, ANPPCAN. Available at www.anppcan.org/ (Accessed 19 February).
Centers for Disease Control and Prevention (CDC) (2006) Adverse Childhood Experiences Study, National Centers for Injury Prevention and Control, Atlanta. Available at http://www.cdc.gov/NCCDPHP/ACE (Accessed 12 May 2014).
Hall, D. and Elliman, D. (eds) (2003) Health for All Children, 4th edn, Oxford, Oxford University Press.
Krug, E.G. et al (eds) (2002) World Report on Violence and Health, Geneva, World Health Organisation.
Lansdown, G. (2011) Every Child’s Right to be Heard, Save the Children, UK. Available at www.savethechildren.org.uk/resources/online-library/every-childs-right-be-heard (Accessed 19 February 2014).
Ministry of Gender, Labour and Social Development (2008) The National Child Participation Guide for Uganda: Creating an Environment for Children to be Heard, Ministry of Gender, Labour and Social Development , Uganda, Child Rights Network, and UNICEF Uganda. Available at http://toolkit.ineesite.org/toolkit/INEEcms/uploads/1033/The_National_Child_Participation_Guide_Uganda.pdf (Accessed 12 May 2014).
Naker, D. (2004) ‘Raising Voices Uganda’, cited in Derib, A. (2005), Regional Report on Physical and Humiliating Punishment Against Children, Save the Children.
Nicholson, S. and Clarke, A. (2007) Child Friendly Healthcare: A Manual for Health Workers in Burr, S. and Southall, D. (eds) Abridged by Alice and Oliver Ross. MCAI & Community Fund, pp. 24–79. Available at www.cfhiuk.org/publications/cfhi_manual.htm (Accessed 19 February 2014).
NSPCC (2010) ‘The definitions and signs of child abuse’, Child Protection Fact Sheet. Available at www.nspcc.org.uk/inform/trainingandconsultancy/consultancy/helpandadvice/definitions_and_signs_of_child_abuse_pdf_wdf65412.pdf (Accessed 19 February 2014).
Save the Children (2003) So You Want to Consult with Children?: A Toolkit of Good Practice. Available at www.savethechildren.org.uk/resources/online-library/so-you-want-consult-children-toolkit-good-practice (Accessed 19 February 2014).
Save the Children (2008) Protect the Children! A Guide to Support Those Working and Living with Children Affected by Violence. Available at www.crin.org/docs/protectchildren.pdf (Accessed 19 February 2014).
Southall, D.P., Coulter, B., Ronald, C., Nicholson, S. and Parke, S. (eds) (2002) International Child Health Care – A Practice Manual for Hospitals Worldwide, Child Advocacy International, London, BMJ Books.
Terenzio, F. (n.d.) ‘Why is child participation so important?’, Global Movement for Children. Available at www.gmfc.org/en/action-within-the-movement/gmc-actions/actions-by-imperatives/6-listen-to-children/past-actions/40-why-is-child-participation-so-important (Accessed 19 February 2014).
UNICEF (n.d.) Fact Sheet: A Summary of the Rights under the United Nations Convention on the Rights of the Child, UNICEF. Available at www.unicef.org/crc/files/Rights_overview.pdf (Accessed, 4 April 2014).
UNICEF (n.d.) UN Convention on the Rights of the Child in Child Friendly Language. Available at www.unicef.org/rightsite/files/uncrcchilldfriendlylanguage.pdf (Accessed 6 May 2014).
United Nations General Assembly (1989) The United Nations Convention on the Rights of the Child. Articles 9, 24, 25, 3. New York, United Nations. Available at www.unicef.org.uk/Documents/Publication-pdfs/UNCRC_PRESS200910web.pdf (Accessed 4 April 2014).
United Nations (2006) World Report on Violence Against Children. Available at www.unicef.org/violencestudy/reports.html (Accessed 4 April 2014).
United Nations (2009) Committee on the Rights of the Child, General Comment No. 12: The Right of the Child to be Heard, CRC/C/GC/2009. Available at www.coe.int/t/dg3/children/participation/CRC-C-GC-12.pdf (Accessed 4 April 2014).
Whitehead, M. (1992) ‘The concepts and principles of equity in health’, Int J. Health Service, vol. 22, pp. 429–45.
Acknowledgements
This is one of five modules in the CREATE curriculum on children’s rights education for health care workers in Ethiopia, Kenya, Tanzania and Uganda. It has been developed through a partnership between the MS Training Centre for Development Cooperation based in Arusha in Tanzania, The Open University in the UK and Child Rights Education for Professionals (CRED-PRO), an international programme committed to strengthening the understanding and application of children’s rights in professional practice.
We would like to thank the Oak Foundation in Geneva for its generous funding for the development of this programme and OPITO for additional funding to support advocacy and engagement activities.
CREATE was produced by a team of experts from the four participating countries, including representatives from government, academia, professional practice and the NGO sector. They were led in Child Rights Advocacy by Gerison Lansdown from CRED-PRO and trained and supported by experts in blended learning pedagogy from the CREATE team at The Open University. Many thanks to the governments and agencies who enabled them to participate. The authors are:
- Humphrey Onyango Wandeo, Children Services, Government of Kenya
- Kellen Karanu, Deputy Director of Children’s Services, Government of Kenya
- Kabanda Obed, MD, Executive Director, Action for Community Development (ACODEV), Uganda
- James Kaboggoza Ssembatya, Assistant Commissioner/Children’s Affairs, Ministry of Gender, Labour and Social Development, Uganda
- Hajat Safinah Kisu Museene, Principal, Jinja School of Nursing and Midwifery, Uganda
- Sarah Bunoti, PhD, Lecturer Department of Psychology, Faculty of Education, Kyambogo University, Uganda
- Stella Ayo-Odongo, Executive Director, Uganda Child Rights NGO Network (UCRNN), Uganda
- Yodit Tesfaye, Child Protection and Promotion Officer, Ministry of Health, Ethiopia
- Samrawit Tassew Mekuria, MD, Medical Education Team Coordinator, Ministry of Health, Ethiopia
- Stephen Ataro Ayella, MD, Save the Children, Tanzania.
The contributors of original material are:
- Gerison Lansdown, Co-Director, Child Rights Education for Professionals
- Andy Rixon, Lecturer in Faculty of Health and Social Care, The Open University, UK
- Tony O’Shea-Poon, Head of Equality and Information Rights, The Open University, UK
- Anna Peachey, Deputy Director (Academic) for International Development, The Open University, UK.
We would like to particularly acknowledge the additional material for this curriculum that was produced by TAMASHA in collaboration with District Youth Networks in Temeke (Dar es Salaam), Arusha and Magu. This was research conducted with young people by young people in Tanzania on their experiences of health care.
We would also like to thank those who acted as critical readers for the CREATE curriculum:
- Kate McAlpine, Freelance Consultant, Caucus for Children’s Rights, Tanzania.
- Els Heijnen-Maathuis, Technical Adviser Education, Save the Children International (Uganda)
- Richard Mabala, Director, Tamasha
- Dr Terry DiPaolo, Freelance Consultant
- Dr Helen Yanacopulos, Senior Lecturer in International Development, The Open University, UK.
The CREATE Team are:
- Gerison Lansdown, Co-Director, Child Rights Education for Professionals
- Andy Rixon, Lecturer in Faculty of Health and Social Care, The Open University, UK
- Tony O’Shea-Poon, Head of Equality and Information Rights, The Open University, UK
- Lindsay O’Dell, Senior Lecturer in Faculty of Health and Social Care, The Open University, UK
- Lesley-Anne Long, Deputy Director (Academic) for International Development (until April 2013), The Open University, UK
- Anna Peachey, Deputy Director (Academic) for International Development (after April 2013), The Open University, UK
- Ellen Scott, Senior Project Manager for International Development, The Open University, UK
- Alison Robinson, Senior Operations Manager for International Development, The Open University, UK
- Gail Vardy, Projects Coordinator for International Development, The Open University, UK
- Delphine Mugisha, Training Coordinator, MS-TCDC, Tanzania
- Steven Ndosi, Manager for Cross Cultural Department, MS-TCDC, Tanzania
- Anna Mbwambo, Programme Assistant, MS-TCDC, Tanzania.
Photographs and illustrations:
- Courtesy of Action for Community Development (ACODEV)
- Child-to-Child in collaboration with Unicef Ethiopia, March 2010.
All editing by Learning and Teaching Solutions at The Open University.
The opinions expressed in the CREATE materials are those of the authors and do not necessarily reflect the views of the donor organisations whose generous support made the production of this material possible.
Grateful acknowledgement is made to the following sources:
Cover image: African Child Getting a Vaccine, ©iStockphoto.com/ranplett.
Illustrations
Page 67: Child friendly health facilities; Page 74: Mother using mosquito net; Page 75: Play area in Ugandan hospital. Taken from Nicholson, S, Clarke, A. Child Friendly Healthcare: A Manual for Health Workers, Child Friendly Healthcare Initiative.
Every effort has been made to contact copyright holders. If any have been inadvertently overlooked the publishers will be pleased to make the necessary arrangements at the first opportunity.