Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Wednesday, 15 July 2026, 4:03 AM
Study Session 14 Emergency WASH Behaviour Communication
Introduction
Emergencies and disasters can occur anywhere and when they do, lack of clean water, poor sanitation and inadequate hygiene practices put people at risk of contracting communicable diseases. Availability of WASH infrastructures and promotion of proper hygiene practices are of paramount importance when disaster strikes. The aim of emergency WASH communication is to enable people in emergencies to take actions to prevent or mitigate water, sanitation and hygiene related diseases and to facilitate community participation to improve their situation.
This study session will focus on promoting improved WASH practices in the context of an emergency and in particular on hygiene behaviour.
Learning Outcomes for Study Session 14
When you have studied this session, you should be able to:
14.1 Define and use correctly all of the key words printed in bold. (SAQ 14.1)
14.2 Explain why WASH behaviour is important in an emergency situation. (SAQ 14.1)
14.3 Outline the key steps in WASH behaviour communication at different phases of an emergency. (SAQ 14.2)
14.4 Describe the process of rapid assessment of an emergency situation to identify needs for WASH behaviour communication. (SAQ 14.3)
14.1 What is emergency WASH?
An emergency is defined as an unexpected and usually dangerous situation that calls for immediate action (Merriam Webster, 2015). Floods, droughts and earthquakes are all possible causes of emergency situations. In such an emergency, many systems you rely on may not function as well as they usually do. Utilities such as electricity, water and phone services may be disrupted. War and other conflicts can also be the cause of emergencies and may result in many people leaving their homes and moving to safer areas. Refugee camps for people fleeing from natural or man-made disasters may be established in locations that do not have the resources to meet basic human needs for water, food and shelter.
People in emergency situations are generally much more susceptible to illness and death from disease, often caused by a lack of sanitation, inadequate water supplies and poor hygiene. Diarrhoea and infectious diseases transmitted from faeces to mouth are the most significant health problems. Increased risk of disease also arises from overcrowding, exposure to new pathogens and the disruption of routine and safe habits.
Inevitably it is the poorest and weakest in society – children, the elderly and disabled – who are most vulnerable in such circumstances and need particular consideration. It is also important to note that whatever physical distress people suffer in an emergency event they will also be mentally traumatised so psychosocial care and counselling are vital components of any response plan. ‘Psychosocial’ refers to both psychological and social effects, which continually interact and influence each other. ‘Psychological effects’ are those that affect perceptions, memory, thoughts, learning, emotions and behaviour. ‘Social effects’ are concerned with altered relationships with family and community (UNICEF, 2006).
Along with food and shelter, safe water, hygiene and sanitation are the highest priority in emergency situations. Unless adequate emergency WASH services are provided quickly to emergency-affected people, disease and possibly death are likely to follow. And unless good hygiene is consistently practised by affected people, the danger of diarrhoea, cholera and other disease outbreaks will persist. This is true in all types of emergencies, from rapid onset natural disasters to long-term crises caused by a range of complex factors.
The main objective of WASH intervention in emergencies is to reduce the transmission of diseases through the promotion of good hygiene practices, the provision of safe drinking water, as illustrated in Figures 14.1 and 14.2, and the reduction of health risks related to poor sanitation.


14.1.1 Standards for emergency response
The organisations usually involved in responding to emergencies include national and local government and many different international, national and local organisations as well as other local groups. They aim to provide humanitarian assistance to the people affected by the emergency. The Sphere Project is an international initiative that aims to improve the quality of actions taken in response to disaster situations. It provides standards against which all humanitarian response activity can be held to account (Sphere Project, 2011). The Sphere Handbook has core sets of standards for:
- water supply, sanitation and hygiene promotion
- food security and nutrition
- shelter, settlement and non-food items
- health actions.
These standards describe the humanitarian actions that should be taken in the event of an emergency in order for ‘disaster-affected populations to survive and recover in stable conditions and with dignity’ (Sphere Project, 2011). Within the water supply, sanitation and hygiene promotion section, standards are set in several different categories, as you can see in Figure 14.3.
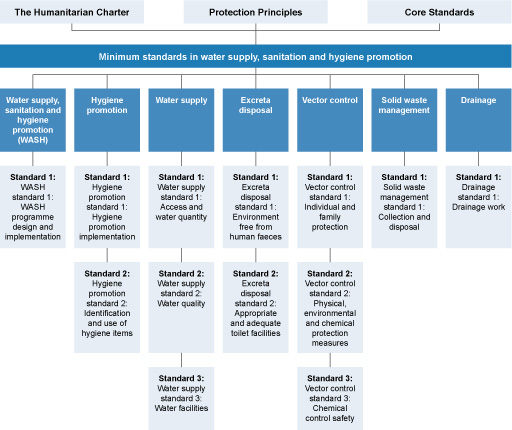
The Sphere Handbook includes standards for responses to meet needs for clean water, basic shelter and sufficient food. It also includes standards for responses concerned with promotional activities and behaviour change, which are the focus of this study session.
Communication interventions for an emergency can be summarised as consisting of three distinct phases: preparedness, response and recovery. We will look at each of these phases in turn in the following sections.
Why is hygiene behaviour critical during emergency?
Hygiene behaviour is critical because disease risks are higher in emergency situations. This is because of overcrowding, lack of safe water and poor sanitation facilities, so has a critical influence on the transmission of disease. In emergency situations it is particularly important to prevent spread of disease.
14.2 Preparedness phase
Preparing for an emergency means planning ahead so that when disaster strikes, there are systems in place to respond quickly and effectively. Being prepared will save lives and help response and rescue operations. Plans for behaviour communication will be part of a broader preparedness plan that covers all aspects of emergency preparation.
For behaviour communication, preparation follows similar principles to those for behaviour and social change communication that you have read about in previous study sessions. Preparedness for behaviour communication in an emergency situation includes a number of steps, outlined below.
1. Develop a communication plan
The first step is to develop an emergency communication plan. Designing a communication plan should begin with bringing the various stakeholders together to determine the objectives of the plan, the methods to be used and the resources required, including financial and human resources (UNICEF, 2012). The stakeholders could include government, NGOs and community representatives. It is important for community representatives to participate in the planning and decision making so that they can provide information about the local situation as well as develop a sense of ownership of the plan.
Remember that effective behaviour change communication is a two-way process and should be a dialogue between the people giving out the information and those receiving it. Working with communities through a process of dialogue can help identify potential barriers to change and specific cultural and social beliefs and practices which might prevent desired behaviour. Sustained dialogue can help bring about community involvement and participation in addressing the emergency.
The communication plan should also consider the roles and responsibilities of different partners, the results in terms of changed behaviour that it is aiming to achieve, and how those results will be monitored at different phases of the emergency (UNICEF, 2006).
2. Identify communication channels
The communication plan will also need to consider the possible methods to be used for providing information. In an emergency, communications need to reach as many people as fast as possible. It is advisable to use both interpersonal methods and mass media methods during an emergency.
Communications to individuals or small groups are unlikely to have the necessary impact but interpersonal methods that reach large numbers of people such as public meetings will be more effective (Figure 14.4). Other options include public address systems with speakers mounted on vehicles.

Mass media, such as radio, television, text messaging via mobile phones, and newspapers can be useful to raise awareness and can also help promote critical behaviours and disseminate programme information (Figure 14.5). These methods help inform large numbers of people quickly but they often do not provide the opportunity for feedback.
Choosing more than one channel for emergency communication means that messages can be repeated and reinforced and can help ensure that as many people as possible are reached. Mass media methods are most effective when combined with interpersonal methods that allow affected people to discuss the information with someone they trust such as community opinion leaders (UNICEF, 2006).

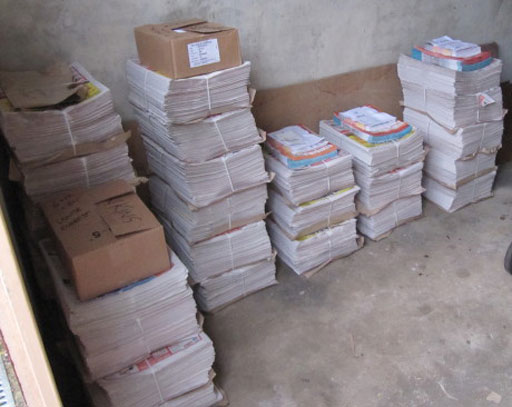
3. Prepare communication materials and keep them ready to use
Some communication materials can be prepared in advance and stored ready for distribution, as shown in Figure 14.6. These would have to be stocked at the district level, so that during an emergency they can be immediately distributed in the field, saving precious time and resources. It may be possible to prepare electronic copies (soft copies) of materials in draft versions that can be finalised and printed (hard copies) when needed.
In the eventuality that new materials need to be produced, it would also be helpful to create a directory of graphic designers, media producers, radio /TV channel contacts and others who you would need to call on for support if an emergency arose.
4. Train service providers in emergency communication skills
In times of stress and trauma caused by an emergency, community level communicators such as Health Extension Workers (HEWs) and members of the Health Development Army (HDAs) need good interpersonal communication skills to inform, motivate, counsel and encourage affected people and communities. Providing the necessary training on interpersonal communication for these frontline workers is an important preparatory activity.
5. Engage communities in preparing and planning for emergencies
The human rights-based approach, supported by the Sphere standards, stresses participatory approaches that engage communities in planning, implementation and monitoring processes. This means that programmes should build on what people already know, and recognise their social and cultural strengths. An important part of preparation, therefore is gathering information from all members of local communities (Figure 14.7).

Communities are, however, made up of many different types of people. Some people may be less able to take part in decision-making processes due to vulnerabilities related to age, gender inequalities, ethnicity, socio-economic status and disability. In areas that are particularly vulnerable to emergency, supporting communities to develop community action plans themselves is a key preparedness activity. The HEWs and HDAs could be instrumental in developing and supervising the implementation of such a plan.
Explain why the following actions are important parts of preparing for an emergency.
- Create a directory of useful contacts for disseminating emergency communications.
- Train frontline health workers in counselling skills.
The answers are as follows:
- Having a directory of useful contacts for disseminating emergency communications would be helpful if there was an emergency because it would save time and enable messages to be sent out more quickly.
- Training health workers in counselling would ensure they had the necessary skills to support their community in the event of an emergency, especially in terms of psychosocial impact. They would also be able to explain messages sent out by other methods such as radio or TV.
14.3 Response phase
The next phase is the response phase which begins when an emergency strikes. An emergency response encompasses the decisions and actions taken to deal with the immediate effects of an emergency. For behaviour communication, UNICEF have described this phase in a number of steps, listed below (UNICEF, 2006; UNICEF, 2012). It should be noted that in some emergency situations, some of these steps may not apply.
1. Participate in rapid assessments
The first step is to assess the situation so that the scale of the emergency is understood. This involves assessments for different sectors including health, water and sanitation, child protection, food etc. When WASH rapid assessments are conducted in the initial phase of an emergency, it is critical that the assessments also identify any high risk practices that have implications for public health of affected communities. Rapid assessment for WASH behaviour is described in more detail in Section 14.3.1.
2. Conduct a rapid appraisal of communication channels and resources
Soon after an emergency is announced, efforts should be made to find ways to reach the vast majority of affected people quickly with information and key messages. This rapid appraisal will revisit the channels identified in the preparedness plan and assess if they are affected by the emergency and which will be the most effective.
3. Revisit and activate the detailed communication plan
Based on the preparedness plan, the details of the implementation of the communication initiative(s) should be activated. All partners should be mobilised to fulfil the roles that had been determined at the planning stage.
4. Focus on re-establishing existing behaviours and norms
In the initial phase, the focus would be on re-establishing the positive behaviours and social and cultural values that existed prior to the emergency. For example, providing handwashing facilities enables people to continue to practice good hygiene behaviour, as shown in Figure 14.8. However, depending on the situation, emergencies might also provide opportunities to promote new behaviours.

5. Forge additional alliances for communication
The emergency might provide opportunities to build additional alliances to include relief workers, service providers, journalists and others so that they are able to directly support desired behaviours among affected people.
6. Facilitate community and children's participation
Through established community level committees, pro-active efforts should be made to create opportunities for affected families and communities, including children and young people, to participate in the response.
7. Working with the media
As a priority, decision makers should come together and decide on what to communicate to the media. The communication should be frequent and effective and through a dedicated spokesperson.
8. Reach the poorest, most vulnerable and hard to reach
You should give particular attention to people who are more vulnerable or marginalised or those who are harder to reach, through special outreach activities.
9. Dealing with psychosocial impact
Emergency can have a variety of psychosocial impacts. People may have strong feelings of fear, insecurity and helplessness. People might not be allowed to undertake usual funeral and mourning practices. Community workers would have to be trained to deal with this situation and community leaders encouraged to help in supporting the community.
Put these actions in the appropriate order when responding to an emergency.
- Create opportunities for children and young people to help out.
- Identify particularly high risk practices.
- Re-establish normal healthy practices and cultural values.
The most appropriate order for these actions would be:
- Identify particularly high risk practices.
- Re-establish normal healthy practices and cultural values.
- Create opportunities for children and young people to help out (see Figure 14.9).

14.3.1 Rapid assessment of hygiene behaviour
As noted above, when responding to an emergency, the first step is to make an assessment so that the situation is understood. Rapid initial assessments will provide information about the nature and scale of the emergency and the likely need for external assistance (WHO, 2002). There will need to be detailed assessments to plan, implement and coordinate responses to meet basic needs for water, food, shelter and medical care. Part of this assessment will be a behavioural situation analysis, such as you encountered in Study Session 8. This will provide understanding of current hygiene behaviours and identify where change is needed and how behaviour change could be achieved. In particular, the assessment should try to identify any key practices that may be putting people at risk, and any alternative or safer practices which would help to mitigate such risks. It should identify any barriers that might prevent people from adopting safer practices and any key motivating factors that will enable change. It should also ascertain preferred communication channels for different participant groups and identify any particularly vulnerable or high-risk groups.
The World Health Organization (2004) recommends the following checklist of questions for a rapid assessment of the public health situation in a community affected by an emergency:
- What health-related behaviours are contributing to public health risks faced by the affected population?
- What are the common health-related practices among the affected population and how have these been affected by the emergency?
- What are the current practices on key hygiene behaviours such as:
- washing hands after defecation?
- disposal of children‘s faeces?
- storage and handling of water?
- storage and handling of food?
- How is the community disposing of their solid waste?
- Is there an understanding in the community of the relationship between water/sanitation/shelter/vectors and disease?
- Does the community have access to water containers with lids/cooking utensils/mosquito nets/soap/sanitary protection/blankets/bathing facilities?
- Are the users involved in the management and maintenance of water sources and latrines?
- What health promotion media are available/accessible to the affected population (radio, posters/leaflets, local folk media and others)?
The answers to these questions will help you identify the key hygiene behaviours in the community affected by the emergency and therefore to target the high-risk behaviours for public health promotion activities. While designing the hygiene promotion campaign in an emergency situation it is important to consider the community’s traditional practices and the facilities available, as well as the damage caused by the emergency. You should also pay special attention to the needs of vulnerable groups such as the sick and wounded, children, the elderly and pregnant women.
What are the main areas of concern for an emergency hygiene promotion programme?
There are many areas of concern, but the main ones are probably:
- safe disposal of faeces
- handwashing after defecation and prior to food preparation
- clean water use and storage
- control of flies and other insect vectors
- personal hygiene (particularly for women and girls)
- food hygiene.
14.4 Recovery phase
The post-emergency or recovery phase is defined as the process of rebuilding, restoring and rehabilitating the community following an emergency. It is a time to revisit the communication plan that was drawn up during the preparedness phase and reassess behaviour to monitor the effectiveness of the plan.
The recovery phase offers an opportunity to expand service delivery and to increase quality and availability of water, hygiene and sanitation related services. In this phase it is important to continue communication activities and to establish and sustain normality as far as is possible in the emergency affected communities. ‘Building back better’ is a principle that takes a positive approach to the opportunities presented post-emergency, underpinning recovery and reconstruction activities that promote more resilient and capable communities. For example, Practical Action (2014) do this through seven principles:
- Do no harm: learn from the past, and avoid unnecessary damage to future recovery.
- Agencies must be accountable to the people they seek to assist.
- People affected by disaster should be the decision makers.
- Recovery of local economy and livelihoods must be a priority.
- Reconstruction and recovery efforts must recognise diversity.
- Communities should be allowed to use their own resources wherever possible.
- Reconstruction must take account of future hazards and risks.
Following these principles can encourage positive developments such as the construction of improved water supply and better sanitation provision for the future. However, the physical reconstruction of buildings and infrastructure following an emergency can sometimes be achieved more quickly than social or psychological rehabilitation (WHO, 2002). The recovery phase in terms of people’s sense of wellbeing may therefore take a long time. Planning for long-term recovery is an important part of emergency planning that needs to be considered as part of the pre-emergency planning phase.
During which phase of emergency should community workers be trained in interpersonal communication skills and why?
Such training should be given during the response phase. This is because people may get strong feelings of fear, insecurity and helplessness during emergencies, and this can have significant psychosocial impact. For example people might not be allowed to undertake usual funeral arrangements and mourning practices and this needs careful handling by people with appropriate training.
During which phase should communication materials be prepared and made ready for dissemination?
Communication materials should be developed, produced and stored ready for distribution during the preparedness phase. This will save precious time and resources. It may also be necessary to produce materials during the response phase.
Summary of Study Session 14
In Study Session 14, you have learned that:
- The main objective of WASH communication intervention in emergencies is to reduce the transmission of diseases from faeces to mouth through the promotion of good hygiene practices, the provision of safe drinking water and the reduction of health risks related to poor sanitation.
- Hygiene behaviour is particularly important in emergency situations where disease risks are acute due to overcrowding, poor water and sanitation, exposure to new pathogens and disturbance of familiar and safe habits.
- Preparing for emergencies involves developing a communication plan with participation from the community. The plan should set objectives, identify communication channels and human and financial resources required in an emergency.
- During the response phase actions are taken to deal with the immediate effects of the emergency. After an initial rapid assessment, activities for behaviour communication will be based on the prepared communication plan using the most effective communication channels to reach people affected with the priority messages.
- Rapid assessment of the public health situation is an important first step in emergency response to identify high risk behaviours that should be targeted for behaviour change communication.
- The recovery phase involves rebuilding, restoring and rehabilitating the community following the emergency. This phase can provide opportunities for improvements in WASH services but recovery from psychosocial impact may take longer.
Self-Assessment Questions (SAQs) for Study Session 14
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions.
SAQ 14.1 (tests Learning Outcomes 14.1 and 14.2)
Give three reasons why emergencies can put people at greater risk of waterborne disease.
Answer
You may have mentioned any three of the following reasons why emergencies can lead to increased risk of waterborne disease:
- Water supply systems may be broken or contaminated so people only have unsafe water to drink.
- Lack of latrines or other safe method for disposing of human waste forces people to defecate in the open.
- Disruption of normal routine and regular habits means that people may not wash their hands at critical times.
- Flies and other disease vectors may increase in the disturbed conditions following an emergency.
- Some emergencies will force people out of their homes to refugee camps which may be in locations with insufficient resources to meet people’s needs. Overcrowding can add to the increased health risk in these camps.
- Displacement of people may possibly expose them to new pathogens.
SAQ 14.2 (tests Learning Outcome 14.3)
Interventions for WASH emergencies can be divided into three distinct phases. What are these three phases? Consider each of the following actions and identify in which of the three phases it would be actioned:
- Production and storage of communication materials.
- Restoring interrupted essential services.
- Contact partners in the media who can help deliver important messages to the community.
- Re-establishing of transportation routes.
- Get information and key messages to affected people quickly.
- Providing food and shelter for those displaced by the incident.
- Designing a communication plan.
- Create opportunities for those affected by the emergency to participate in the response.
Answer
The three phases of emergency WASH communication are preparedness, response and recovery or post-emergency phases. For each of the actions given, the appropriate phase is as follows:
- Production and storage of communication materials – preparedness phase.
- Restoring interrupted essential services – responses and recovery phases.
- Contact partners in the media who can help deliver important messages to the community – preparedness and response phases.
- Re-establishing of transportation routes – response and recovery phases.
- Get information and key messages to affected people quickly – response phase.
- Providing food and shelter for those displaced by the incident – response phase.
- Designing a communication plan – preparedness phase.
- Create opportunities for those affected by the emergency to participate in the response – response phase.
SAQ 14.3 (tests Learning Outcome 14.4)
Look at the suggestions given in Section 14.3.1 of questions you might ask as you undertake a rapid assessment of hygiene behaviour. Select four questions which you think would be most helpful in identifying the key practices that are putting people at risk. How might the answers to these questions help in identifying the key high risk behaviours? What actions could help mitigate the risks? Present your answer as a table, with one column for the key question, a second column for how the answers could help identify the key practices, and a third column for the actions.
Answer
Most of the questions listed would help to identify the key practices which are putting people at risk, but you have probably selected four of the six most crucial questions listed in the table below.
| Key question | How answers to this question could help | Actions to mitigate the risks |
| What are the common health-related practices among the affected population and how have these been affected by the emergency? | Identify what has become more of a risk now that the emergency situation has arisen | Target the behaviour communication interventions at these specific practices |
| What are the current practices on the key hygiene behaviours such as washing hands after defecation? | Identify if handwashing has been compromised as a result of the emergency and whether there has been an increase in the practice of open defecation | Provide handwashing facilities and latrines |
| What method is being used for disposal of children‘s faeces? | Identify if children’s faeces are a source of infection | Using appropriate communication channels, explain that children’s faeces are no different from adult faeces as a health risk |
| What practices are being used for storage and handling of water and of food? | Identify whether water and food could be getting contaminated and could therefore be an additional source of infection. | Provide storage containers and explain why correct storage is important to prevent contamination |
| How is the community disposing of their solid waste? | Identify whether solid waste might be an additional source of infection or encouraging disease vectors such as flies | Establish a waste collection site and organise proper disposal e.g. burning |
| Does the community have access to water containers with lids/cooking utensils/mosquito nets/soap/sanitary protection/blankets/bathing facilities? | Identify particular items which need to be provided urgently | Provide and distribute required items |