Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Friday, 24 April 2026, 4:51 AM
Communicable Diseases Module: 8. Malaria Case Management
Study Session 8 Malaria Case Management
Introduction
You have now learned how the malaria parasite is transmitted, the life cycle of the parasite, the symptoms and signs of the disease and the diagnosis of malaria. The objective of this study session is to give you the required knowledge and skills to provide effective and prompt treatment for malaria cases. You are going to learn:
- How to treat uncomplicated (non-severe) malaria in adults, in children and pregnant mothers.
- The pre-referral treatment of severe malaria cases.
- How to educate people about the benefits of early treatment of cases and adherence to the treatment course.
This study session will describe the procedures of malaria treatment, the anti-malaria medicines used under different situations, and the procedure of providing pre-referral care to patients that cannot be managed at your Health Post level. Providing early and effective treatment is one of the most important interventions of any malaria control programme. In fact, the most important indicator used to measure the success of malaria interventions is the proportion of people with malaria getting anti-malaria treatment within 24 hours after the onset of fever.
Unlike many communicable diseases, malaria is an acute infection that requires immediate attention after the onset of symptoms. The disease can quickly progress to a severe form, and death can occur within 48 hours of the onset of signs and symptoms. As a Health Extension Practitioner deployed within a village, you are the most important person, and probably the only person, who can provide early and effective treatment for malaria cases, within 24 hours. This is probably one of the most satisfying parts of your job because it is directly linked to saving lives.
Learning Outcomes for Study Session 8
When you have studied this session, you should be able to:
8.1 Define and use correctly all of the key words printed in bold. (SAQs 8.1 to 8.6)
8.2 List the different anti-malaria drugs and the dosage given to uncomplicated and severe cases of malaria. (SAQs 8.2, 8.4 and 8.6)
8.3 Describe the procedure for treating uncomplicated malaria and giving supportive treatment in different age groups and in pregnant mothers. (SAQs 8.1, 8.2 and 8.6)
8.4 Describe the procedure for the pre-referral treatment of cases of severe malaria and when to refer them to the health centre. (SAQs 8.3, 8.4 and 8.6)
8.5 Explain how you would identify and address the challenges in malaria case management. (SAQs 8.5 and 8.6)
8.1 Treatment of uncomplicated malaria
In Study Session 7 you learned the different methods for diagnosing malaria and how the clinical diagnosis and Rapid Diagnostic Test (RDT) methods are applied at the Health Post level. In this section you will learn about the treatment of uncomplicated (non-severe) malaria cases.
In order to prescribe an anti-malaria treatment for malaria-suspected fever cases, you should make a confirmed diagnosis using a multi-species RDT. This is an RDT that can test for different species of the malaria parasite. However, if you do not have this RDT at your Health Post, you can still make a malaria diagnosis based on the patient’s history and based on findings of physical examination. The summary of the steps you follow to make a diagnosis and prescribe treatment for malaria is indicated in Box 8.1 below.
Box 8.1 Steps to follow to treat malaria cases
- Take history of the patient, including history of travel to malarious areas. Take enough time to pay proper attention to what the patient has to say.
- Do a physical examination, measure temperature, blood pressure and count the pulse rate.
- Consider if there is another obvious cause of fever other than malaria.
- Test for malaria parasites using multi-species RDTs (if you have the test kits and have been trained to use them).
- Treat the patient based on the result of the RDT.
- If you do not have RDTs in your Health Post, diagnose malaria based on the clinical findings from the patient’s history and the physical examination.
In the next section you will learn the course of action to take when you use either an RDT, or clinical diagnosis, to determine the treatment of malaria. Carefully note the slight differences between the two approaches.
8.1.1 Treatment of uncomplicated malaria based on RDT confirmation
Scenario 1
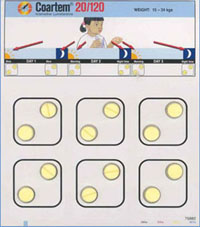
If RDT indicates P. falciparum infection then treat the patient with appropriate doses of Coartem (one of the artemisinin-based combination drugs), or artemisinin combination therapy with chemical ingredients of artemether-lumefantrine. Before you give the patient Coartem, make sure that the patient is able to swallow the medication, and is not vomiting. (See the treatment doses of Coartem in Table 8.1). Coartem tablets are given according to the body weight or age of the patient, in six doses to be taken over three days. Give the first dose to the patient in front of you. Advise your patient to take fatty foods if available. If fatty food is not available, advise the patient to take any foods or fluids after swallowing Coartem. Explain that a fatty meal or milk improves absorption of Coartem, hence the patient can recover faster.
One tablet of Coartem contains 120 mg artemether, plus 20 mg lumefantrine, in a fixed dose.
| Weight (kg) | Age | Day 1 | Day 2 | Day 3 | |||
|---|---|---|---|---|---|---|---|
| Morning | Evening | Morning | Evening | Morning | Evening | ||
| 5–14 | 4 months–2 years | 1 tablet | 1 tablet | 1 tablet | 1 tablet | 1 tablet | 1 tablet |
| 15–24 | 3–7 years | 2 tablets | 2 tablets | 2 tablets | 2 tablets | 2 tablets | 2 tablets |
| 25–34 | 8–10 years | 3 tablets | 3 tablets | 3 tablets | 3 tablets | 3 tablets | 3 tablets |
| 35+ | 10 + years | 4 tablets | 4 tablets | 4 tablets | 4 tablets | 4 tablets | 4 tablets |
Scenario 2
If the RDT indicates mixed infection of P. falciparum and P. vivax, then treat the patient with appropriate doses of Coartem, as in Table 8.1.
Scenario 3
Chloroquine tablets are 150 mg base, and the syrup is 50 mg base per 5 ml dose.
If the RDT reveals P. vivax only, then treat the patient with Chloroquine (see the treatment doses in Table 8.2). Chloroquine is prepared in tablet or in syrup form. Chloroquine dose is 10 mg/kg of the patient’s body weight, taken orally immediately (day 1), followed by 10 mg/kg at 24 hours (day 2), and 5mg/kg at 48 hours (day 3).
How many tablets of Chloroquine to take home do you give to a woman aged 36 years who is diagnosed with P.vivax malaria? Note that you give her the first dose, i.e. 4 tablets, while she is in front of you.
You give her the remaining 6 tablets to take home. She will swallow 4 tablets on the second day and 2 tablets on the third day.
| Weight (kg) | Age | Day 1 | Day 2 | Day 3 |
|---|---|---|---|---|
| 5–6 | less than 4 months | ½ tablet OR 5 ml syrup | ¼ tablet OR 5 ml syrup | ¼ tablet OR 2.5 ml syrup |
| 7–10 | 4–11 months | ½ tablet OR 7.5 ml syrup | ½ tablet OR 7.5 ml syrup | ½ tablet OR 5 ml syrup |
| 11–14 | 1–2 years | 1 tablet OR 12.5 ml syrup | 1 tablet OR 12.5 ml syrup | ½ tablet OR 7.5 ml syrup |
| 15–18 | 3–4 years | 1 tablet OR 15 ml syrup | 1 tablet OR 15 ml syrup | 1 tablet OR 15 ml syrup |
| 19–24 | 5–7 years | 1½ tablets OR 20 ml syrup | 1½ tablets OR 20 ml syrup | 1 tablet OR 15 ml syrup |
| 25–35 | 8–11 years | 2 tablets | 2 tablets | 1 tablet |
| 36–50 | 12–14 years | 3 tablets | 3 tablets | 2 tablets |
| 51+ | 15 + years | 4 tablets | 4 tablets | 2 tablets |
Scenario 4
If the RDT is positive for P. falciparum in:
- women who are less than 3 months pregnant,
- children whose weight is less than 5 kg or whose age is less than 4 months,
give quinine oral treatment. (See the treatment doses of quinine tablets in Table 8.3 below).
Quinine tablets may contain 200 mg or 300 mg. Check carefully when you calculate the dose.
| Weight (kg) | Age | Dosage to be given daily | |
|---|---|---|---|
| 200 mg tablets | 300 mg tablets | ||
| 4–6 | 2–4 months | ¼ | - |
| 6–10 | 4–12 months | ⅓ | ¼ |
| 10–12 | 1–2 years | ½ | ⅓ |
| 12–14 | 2–3 years | ¾ | ½ |
| 14–19 | 3–5 years | ¾ | ½ |
| 20–24 | 5–7 years | 1 | ¾ |
| 25–35 | 8–10 years | 1½ | 1 |
| 36–50 | 11–13 years | 2 | 1½ |
| 50+ | 14 years and above | 3 | 2 |
For all of Scenarios 1 to 4, if the patient vomits within 30 minutes after swallowing the drug, the medicine will not work. So give the patient the same dose again from your own stock (not from the tablets you give to the patient or the mother/caregiver to take home) and let the patient swallow it.
If a child vomits within 30 minutes of taking drugs at home, advise the patient/caregiver to take another dose, and to come back to the Health Post to collect another replacement dose from you so that the patient still takes the complete course of treatment.
To ensure appropriate intake of prescribed drugs, patients/ caregivers should be well informed on the treatment schedule to ensure intake of the complete dose.
Advise the patient/caregiver to come back if the patient does not show any improvement after three days of treatment with anti-malaria drugs, or if the signs and symptoms get worse at any time.
Whenever you encounter a suspected malaria case, use Figure 8.1 to guide you on the details of the procedures and steps that you need to follow to identify uncomplicated and severe malaria cases using RDTs, and manage them appropriately.

If the RDT result of Bekele, who is a 7-year-old child, shows P. falciparum infection, what anti-malaria drug would you give him? How many tablets will be a complete course of treatment? If Bekele vomited 25 minutes after swallowing the first dose you gave him, what should you do next?
The appropriate anti-malaria drug to give Bekele is Coartem.
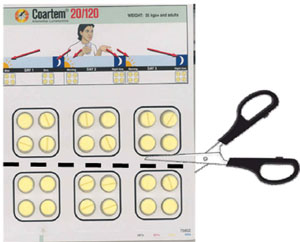 Figure 8.3 Cutting an adult Coartem strip with scissors into two to give to children.
Figure 8.3 Cutting an adult Coartem strip with scissors into two to give to children.The total number of tablets you give a 7-year-old child is 12 (go back to see the doses in Table 8.1 above). The Coartem strip that contains 12 tablets is shown in Figure 8.2. Bekele should be given 2 tablets in the morning and 2 tablets in the evening for 3 days.
To replace the vomited dose, which is 2 tablets, give the child another 2 tablets to swallow again from your own stock — not from the tablets you gave to the mother/caregiver. The mother/caregiver must have 10 tablets to take home to continue the treatment.
Note that if the strip in Figure 8.2 (which is appropriate for Bekele) is not available, you can still cut out 12 tablets from the strip of adult doses as shown in Figure 8.3. While cutting the strips be careful not to cut the plastic or the blisters that contain individual tablets.
Coartem shelf life and contraindications
Coartem has a short shelf life of two years only. So use those packages which are closer to the expiry date first. Do not expose Coartem to moisture and high temperature. Store it at temperatures of below 30oC in dry and cool places.
Coartem absorbs moisture from the surrounding environment very fast. To protect the drug from absorbing the moisture it is covered by plastic blisters. Therefore, do not remove the tablet from the blister if it is not going to be used immediately.
Coartem is contraindicated (not given) for some people. Box 8.2 gives you specific warnings on the groups who should not get Coartem.
Box 8.2 Contraindications of Coartem
Previously, Coartem was contraindicated for breastfeeding mothers of infants less than 5 kg or under 4 months old. WHO Malaria Treatment Guidelines, 2010, now state that Coartem should be given to these patients.
Do not give Coartem for the following groups of people:
- For use as prophylaxis, that is for a healthy person who wants to swallow the drug in order to protect himself or herself from getting malaria
- Pregnant women in the first trimester (three months of pregnancy) and infants less than 5 kg or less than 4 months old
- Persons with a previous history of reaction after using the drug.
8.1.2 Treatment of uncomplicated malaria based on clinical diagnosis
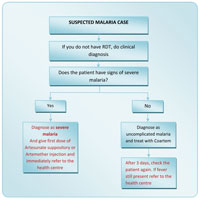
If you do not have the RDT in your Health Post, then use clinical methods (as described in Study Session 7) to diagnose suspected malaria in people seeking your help. If the diagnosis is clinical rather than parasite-based, treat uncomplicated malaria cases as follows:
- If the person does not have signs of severe malaria, then treat the patient with Coartem. After three days, check the patient again. If fever is still present refer the patient to the health centre.
- If the person has signs of severe malaria (as described in Section 8.2) then diagnose him/her as having severe malaria. Give first dose of Artesunate suppository or Artemether injection and immediately refer the patient to the nearest health centre.
- Advise the patient/caregiver to come back if the patient does not show any improvement after three days of treatment with anti-malaria drugs, or if the signs and symptoms get worse at any time.
Whenever you encounter a suspected malaria case and you do not have RDTs, Figure 8.4 will guide you in the details of the procedures and steps that you need to follow for the treatment and referral of patients diagnosed clinically.
8.1.3 Supportive treatment of uncomplicated malaria cases
Many malaria patients have other clinical problems associated with malaria infection. While most of these problems get resolved when the patients are treated for malaria, some conditions need treatment at the same time as the malaria, that is, supportive treatment. Some of the supportive treatments that you should give the patient are as follows:
- If high fever is present, give the patient paracetamol tablets. Also advise the patient or caregivers to cool the fever by wetting the body of the patient with clean pieces of cloth dipped in slightly warm water, or by fanning.
- For patients with moderate dehydration, give oral rehydration salts (ORS) and advise them to drink more clean water or other fluids. In the case of breastfed infants, encourage mothers to provide extra breastfeeding.
- If you suspect mild or moderate anaemia is present, give ferrous sulphate (iron tablets), 200 mg once daily for two months, and advise the patient to return for a recheck in two months.
In addition to the diagnosis and treatment services you give to the patient with uncomplicated malaria, advise or educate the patient or the caregiver on the following issues and tell him or her that:
- He or she has a malaria infection.
- Early treatment within 24 hours of fever onset is important to prevent severe illness and death.
 Figure 8.5 Give food and fluids prior to malaria treatment.
Figure 8.5 Give food and fluids prior to malaria treatment. - To take/give the patient enough food, if possible a fatty meal, prior to taking the drug (Figure 8.5).
- To complete the full dose of treatment of the drug given, for example six doses of treatment for three days for Coartem.
- To return to the Health Post if the fever does not stop or if the patient does not get well after three days. The patient should also return to the Health Post if at any time before three days the condition gets worse — for example if the patient is unable to avoid vomiting up the drug, or there is persistent vomiting, dehydration, confusion, or excessive sleepiness.
8.2 Pre-referral treatment of severe malaria at the Health Post level
It is important that all patients are assessed for the danger signs of severe malaria that you learned about in Study Session 7 (Section 7.2.2). If a patient comes to the Health Post with danger signs, or is found to have any of them, he or she will require urgent medical attention and should be referred to a health centre as soon as possible.
![]() Always remember that a delay in referral could cause death of the patient. The risk of death for severe malaria is greatest in the first 24 hours.
Always remember that a delay in referral could cause death of the patient. The risk of death for severe malaria is greatest in the first 24 hours.
Before referring the patient, give pre-referral treatment for all patients presenting with any of the danger signs of severe malaria, regardless of whether the RDT result is negative or positive. The pre-referral treatments that you should give the patient include:
- The first dose of rectal Artesunate (see Table 8.4 below for the dosages), or if available, an intramuscular injection of Artemether in a dose of 3.2 mg/kg body weight.
- If an Artesunate suppository is expelled from the rectum within 30 minutes of insertion, insert a second suppository.
- In young children, hold the buttocks together for 10 minutes to ensure retention of the rectal dose of Artesunate.
| Weight (kg) | Age | Artesunate dose (mg) | Formulation of the regimen (given all at the same time) |
|---|---|---|---|
| 5–8.9 | 0–12 months | 50 | One 50 mg suppository |
| 9–19 | 13–42 months | 100 | One 100 mg suppository |
| 20–29 | 42–60 months | 200 | Two 100 mg suppositories |
| 30–39 | 6–13 years | 300 | Three 100 mg suppositories |
| 40–59 | >13 years | 400 | One 400 mg suppository |
| 60–80 | Adults | 800 | Two 400 mg suppositories |
| 80+ | Adults | 1,200 | Three 400 mg suppositories |
- Remember to give supportive treatment as indicated in Section 8.1.3 of this session if the patient has high fever, or dehydration, and in case of breastfed infants, encourage mothers to provide extra breastfeeding.
- If the patient is unconscious, in addition to the above mentioned pre-referral treatments, perform the activities indicated in Box 8.3.
Box 8.3 Steps in managing an unconscious patient
Ensure ABC of life support, as follows:
- A = Airway: in the unconscious or convulsing patient it is imperative that the airway is free of obstructions. In the convulsing child you may thrust the jaw forward to ensure a clear airway. Show family members how to position the patient (on his or her side) to ensure a clear airway is maintained.
- B = Breathing: check that the patient is breathing by looking for chest movements and listening for breath sounds.
- C = Circulation: feel or observe that hands and fingers are not cold, and colour is normal. Also check that the capillaries are refilling with blood by applying pressure for few seconds to a fingernail bed, then release the pressure to see if the blood returns fast, which is normal. Monitor and record vital signs (blood pressure, pulse, respiration rate).
For all the patients you are referring, ensure that the referral form is completed with detailed information, including:
- Clinical presentation/patient’s medical history.
- Suspected diagnosis.
- RDT tests performed and results.
- List of all drugs/medication given, route, dose and time of administration.
- Reason for transfer to health centre.
8.3 Management of malaria in special groups
Special population groups such as infants below the age of four months or below 5 kg weight, and pregnant mothers in the first trimester, need different treatment and special attention.
What is the drug you give to treat malaria for an infant less than 5 kg body weight?
You give quinine oral tablets three times a day for 7 days, with the dose as indicated in Table 8.3 earlier in this study session.
Pregnant women
Now we will tell you about pregnant women. Pregnant women are at high risk of developing severe malaria. In addition, malaria during pregnancy can cause premature labour, stillbirth or abortion, as well as severe anaemia in the mother. The baby that is born may have low birth weight.
Therefore, you must give effective anti-malaria treatment to pregnant women with malaria immediately.
Pregnant women in the first trimester (the first three months) of pregnancy should NOT take Coartem. During the first trimester give oral quinine three times a day for 7 days (for dosage see Table 8.3 above). However, you can give Coartem if there is no quinine, or if you strongly believe that the mother may not comply with the seven days of quinine treatment. The first dose should be given under your direct supervision.
If vomiting occurs within 30 minutes after swallowing the drug, the dose should be repeated with a replacement dose to ensure completion of treatment.
Advise the patient to take food while taking the drug, as quinine might cause low blood sugar (hypoglycaemia). Also assure her that symptoms like dizziness, ringing in the ears, blurred vision and tremors might occur, but these are not severe enough to stop treatment, and they will end when the drug treatment is finished. Explain to her the importance of completing her malaria treatment for the health of her unborn baby.
8.4 Adherence to malaria treatment
Adherence to malaria treatment, that is taking all the doses that are given, is very important for successful malaria treatment outcome. If patients do not adhere to the treatment they will not get cured completely and the disease will come back. Not adhering to the treatment can also lead to the parasites becoming resistant to the drug, so in future the drug will be less effective against the parasites.
Critical to patients’ adherence is good communication between you and your patients. Adherence to malarial medication in patients has been linked to knowledge of malaria, access to information on medication for malaria, perceived benefit from the medication, and perceived barriers to treatment.
To ensure adherence, identify high risk patients that might not adhere to the treatment that is given to them. Do this identification during history-taking and clinical assessment. If the patient has one of the risk factors in Box 8.4, then he or she may not adhere to the full course of the drug treatment they received.
Box 8.4 Patients at high risk of low adherence to treatment
- Patients with chronic medical illness.
- Lack of transportation to come back or to send a sick family member.
- History of psychiatric conditions.
- Lack of economic support.
- Pregnant mothers.
- History of poor drug adherence for anti-malaria treatment.
Therefore, arrange a follow-up visit or link the patient to volunteer community health promoters or family members, if he or she is at risk of non-adherence.
During the first contact, if the patient is identified as a malaria case and has the high-risk features shown in Box 8.4, the following are the actions and key messages that you should tell to the patient:
- Ensure the first dose of the malaria treatment is taken under your observation and is well tolerated and not immediately vomited.
- Advise the patient to complete the treatment and educate him or her on the risk of not completing. If the full course is not taken the malaria will occur again.
- Advise patients not to share the drug with other sick members of the family. Advise them to send the sick ones to the Health Post.
- Visit the patient on the second day of the treatment and ensure that he or she takes the drugs properly (this can be aligned with your routine home visit).
- Link the patient to volunteer community health promoters or family members, who will ensure the patient takes the drugs properly.
8.5 The role of the Health Extension Practitioner in malaria treatment
Malaria is a curable and preventable disease, but it still kills many people. The main reasons for this unsatisfactory situation are:
- Some people do not come for treatment until they are very ill because:
- They do not realise they might have malaria (people often think they have a common cold or other simple common infection).
- They do not realise that malaria is a very dangerous disease.
- Many people do not know what causes malaria or how it is spread, so they are not able to protect themselves from the disease. (Prevention is covered in Study Sessions 9, 10 and 11.)
As a Health Extension Practitioner you can improve the situation by:
- Educating people to seek treatment immediately if they have a fever. This is especially important in young children and pregnant women, who should receive treatment against malaria within 24 hours of becoming ill.
- Recognising and treating malaria to prevent severe illness and death.
- Explaining how to take the treatment correctly, so that people can avoid repeated attacks of malaria.
- Advising patients who do not improve within 48 hours after starting treatment, or whose condition is serious, to go immediately to the nearest health centre that is capable of managing severe malarial disease.
8.5.1 Key messages and instructions
The problem of poor adherence may be overcome with simple health messages even when the majority of individuals are illiterate and lack formal education. Explain to people in your community that:
- Malaria is a killer disease if the treatment is not taken properly.
- Make sure that the patient has clearly understood drug labels and instructions.
- Clearly explain how to complete the treatment for malaria.
- Tell them not to interrupt taking medication. To take all (full course) of the anti-malaria drugs, prescribed to them.
- Do not share anti-malaria drugs with others.
- Whenever a family member has a fever, take them to the Health Post immediately.
Summary of Study Session 8
In Study Session 8, you have learned that:
- Treatment of uncomplicated malaria should be based on diagnosis of malaria parasites using RDTs, but in the absence of RDTs, treatment can be given based on clinical diagnosis of malaria.
- Different anti-malarial drugs that are used to treat malaria are based on the type of the malaria parasite species. All uncomplicated falciparum malaria patients and patients with mixed infections, except pregnant mothers in the first trimester, and infants less than four months old, are treated with Coartem. Plasmodium vivax cases are treated with Chloroquine.
- It is equally important to treat other symptoms like high fever, dehydration and anaemia in uncomplicated malaria cases with the appropriate supportive treatment methods.
- Severe malaria should be referred to the nearest health centre very fast. Before referring the patient it is important to give pre-referral treatment; this will help to prevent the patient’s condition from getting worse.
- The key messages you have to give to your community should focus on seeking early treatment and adherence to treatment.
Self-Assessment Questions (SAQs) for Study Session 8
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 8.1 (tests Learning Outcomes 8.1 and 8.3)
Which of the following statements about supportive treatment is false? In each case, state why it is incorrect.
A Supportive treatment is given to kill the malaria parasites in the blood circulation of the patient.
B Malaria patients with high grade fever should be given supportive treatment.
C Patients with moderate dehydration have to be immediately referred to a health centre without giving any supportive treatment.
D No supportive treatment is required for women with malaria, with normal temperature, who can breastfeed very well and with no anaemia.
E If the malaria patient has moderate anaemia, then treat with ferrous sulphate (iron tablets).
Answer
A is false. Supportive treatment is what is given to treat other conditions at the same time as the malaria treatment. It is not the supportive treatment that kills the parasites; rather it is the anti-malaria drugs that you give to the patient that kills the parasites in the blood circulation.
B is true. Malaria patients with high grade fever should be given supportive treatment such as paracetamol tablets, or cooling the body of the patient with clean pieces of cloth dipped in slightly warm water, or by fanning.
C is false. Malaria patients with moderate dehydration should be given oral rehydration salts (ORS) as supportive treatment. The patient should also be advised to drink increased amounts of clean water or other fluids.
D is true. If the temperature is normal, there is no sign of dehydration and no anaemia, you do not need to give supportive treatment to a malaria patient even if she is breastfeeding. Just treat the malaria.
E is true. Malaria patients with mild or moderate anaemia should be treated with ferrous sulphate (iron tablets) 200 mg once daily for two months, and advised to return for recheck in two months.
SAQ 8.2 (tests Learning Outcomes 8.2 and 8.3)
What anti-malaria drug would you give a patient with a clinical diagnosis of uncomplicated malaria, if you cannot do an RDT? How many times a day does the patient take this drug?
Answer
If you diagnose malaria clinically (if there is no RDT) you give the patient Coartem, unless the patient is a pregnant woman in the first trimester, or an infant under 5 kg or under four months (they get quinine tablets instead).
Coartem is given two times a day (in the morning and in the evening) for three days. The first dose is given in front of you immediately after the diagnosis of malaria. The rest of the drug is given to the patient/caregivers to take at home.
SAQ 8.3 (tests Learning Outcome 8.4)
Molamo is a 15 year-old boy who came to your Health Post. You diagnosed him with malaria and gave him Coartem. He took the medicine correctly as you ordered. Three days after his first visit he came back to your Health Post with no improvement of the fever. Describe the actions that you have to take.
Answer
Give pre-referral treatment to Malomo (one 50 mg rectal suppository of Artesunate — see Table 8.4) and immediately refer him to the nearest health centre.
SAQ 8.4 (tests Learning Outcomes 8.2 and 8.4)
Describe what you would do if you found that a patient who came to your Health Post is a suspected severe malaria case?
Answer
Severe malaria should be referred to the health centre very fast. Before referring the patient it is important to give a pre-referral treatment with rectal Artesunate (or intramuscular injection of Artemether, if available). This will help to prevent the patient’s condition from getting worse.
SAQ 8.5 (tests Learning Outcome 8.5)
What could happen if a malaria patient does not take the full course of treatment or does not adhere to the treatment?
Answer
If the patient does not adhere to the treatment he or she will not get cured completely and the disease will come back. It also leads to the development of resistance to the drug by the malaria parasites.
Read Case Study 8.1 about Beka and answer the questions that follow it.
Case Study 8.1 Is Beka sick with malaria?
Beka is a five-year-old boy. His mother brought him to you to seek treatment. Beka and his family are living in your catchment area, which is malarious. The mother says he was well until this morning when he woke up and said he was feeling tired and refused his breakfast. When the mother touched him, he felt hot and she gave him ½ a tablet of paracetamol.
When you examined Beka, you found a well-nourished 15-kg child, not pale, alert and with temperature of 38.5°C measured with the thermometer under his armpit. You could not do a RDT because you used the last kit two days ago. In the rest of the examination, Beka is normal.
SAQ 8.6 (tests Learning Outcomes 8.2, 8.3, 8.4 and 8.5)
- a.What is your diagnosis?
- b.What treatment will you give Beka? And what dose?
- c.What will you tell his mother?
Answer
- a.Uncomplicated malaria is the diagnosis you should give to Beka.
- b.Coartem is the correct treatment for a child of five years. The full dose is 12 tablets. Beka takes two tablets in the morning and two tablets in the evening for three days. You give two tablets to swallow immediately and give the remaining 10 tablets to Beka’s mother to take home.
- c.Advise Beka’s mother on the following issues:
- Tell her the reason for giving the drug.
- Demonstrate to her on how to give the correct dose.
- Tell her to watch while Beka is taking each dose of the drug.
- Explain that the drugs must be finished even if Beka feels well.
- Advise her on when to return if Beka does not improve.