Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Wednesday, 24 June 2026, 7:37 PM
Communicable Diseases Module: 17. Tuberculosis Infection Control
Study Session 17 Tuberculosis Infection Control
Introduction
TB infection control is a combination of measures aimed at minimising the risk of TB transmission within a population. The foundation of TB infection control is early and rapid diagnosis, and proper management of TB patients.
In this study session you will learn about TB infection control and the methods you can use to control TB infection at the health facility, in your community and at home. You will learn that when you use more than one method at a time, you will get better results than when you use only one method. Your knowledge of the methods will enable you to provide proper advice to the community members you are hoping to help, in order to control TB infection at home, in the community and health facility. The different approaches you will learn about need to be promoted as a package because their adoption in that way reduces transmission of TB in healthcare facilities.
Learning Outcomes for Study Session 17
At the end of this study session, you should be able to:
17.1 Define and use correctly all of the key words printed in bold. (SAQ 17.1)
17.2 Define the general principles of infection control applied during handling of TB suspects or TB cases. (SAQ 17.1)
17.3 Explain how you would limit TB transmission in the community and at household level. (SAQs 17.1, 17.2 and 17.3)
17.4 Describe the main elements of TB infection control measures used at the community health facility level. (SAQs 17.1 and 17.2)
17.5 Describe the measures for TB infection prevention in areas where many people gather, at homes and in the community. (SAQ 17.3)
17.6 Explain how you would inform, educate and persuade community members to participate in TB infection control. (SAQ 17.3)
17.1 Principles of TB infection control
In this study session you will learn about the general principles of infection prevention measures that should be taken when dealing with patients and in particularly about infection control of TB. First, three main TB control measures that are used to prevent TB infection are sometimes called the three Is, given that they all three start with that letter. You already know about the first two from reading earlier study sessions and it is the last topic we are going to focus on in this study session.
- Intensified case finding for TB
- Insoniazid preventive therapy (IPT) for prevention of TB amongst people living with HIV
- Infection control for prevention of TB.
17.1.1 What is infection control?
In general, infection control refers to the interventions required to prevent the transmission of micro-organisms from infected patients to other patients and health workers. Infection control measures are based on an understanding of how different diseases are transmitted. Types of infection control include:
Standard precautions, which should be applied regardless of disease or type of institution. For this reason, they are also known as universal precautions.
Transmission-based precautions, which should be applied in specific circumstances, depending on the transmission routes of various diseases.
17.1.2 What are standard or universal precautions?
Standard precautions are those which should always be applied when dealing with any patients, including TB patients. These include:
- Hand washing and antisepsis
- The use of personal protective equipment (e.g. gloves)
- Appropriate handling of patient care equipment and soiled cloths
- Prevention of accidental needle stick/sharp injuries to healthworkers
- Environmental cleaning and spills management
- Appropriate handling of clinical waste (e.g. swabs).
For TB, the transmission-based precautions are those that protect people from airborne bacteria entering the body through inhalation, as you will now learn.
17.2 TB infection control measures at community health facility level
The control measures — or interventions — that need to be brought into play at the level of the health facility fall into the four broad categories shown in Box 17.1. They begin with managerial activities and under that heading a range of national and sub-national interventions are listed that help give managerial order and direction to what happens at the level of the health facility to enable effective TB infection control. The other categories give similar detail on what happens by way of administrative controls, environmental controls and also at the level of the individual health worker.
Describing TB control measures using the headings in Box 17.1 is a useful way of explaining their importance to you as a health worker. We will introduce each of these categories in turn — you will then have a sound understanding of how each intervention operates at a particular point in the airborne TB transmission process. In a later section, we’ll use the same four headings to describe the interventions that are appropriate for places where people gather (congregate settings) in the community and at the level of the household.
Box 17.1 Interventions for TB infection control in health-care settings
Managerial activities
- Identify and strengthen coordinating bodies, and develop a comprehensive human resources plan for planning and implementation at all levels
- Conduct surveillance and assessment at all levels of the health system
- Engage civil society and promote communication and social mobilisation
- Conduct monitoring and evaluation
- Enable and conduct operational research.
Administrative controls
- Develop strategies to promptly identify potentially infectious cases (triage), separate them, control the spread of pathogens (cough manners) and minimise time in healthcare settings.
Environmental controls
- Natural ventilation
- Mechanical ventilation
- Ultraviolet germicidal irradiation (UVGI) fixtures
- Health facility design and renovation.
Personal protective interventions
- Respirators
- Package of prevention and care for healthcare workers, including isoniazid preventive therapy (IPT) for HIV-positive health-care workers.
17.2.1 Managerial controls
Managerial activities need to be given a high priority in this package of measures since they establish the overall programme for the implementation, operation and maintenance of the other interventions. As a health worker, you do not have the responsibility of taking on these managerial activities but it is important you know about them. You will see from Box 17.1, that these managerial activities include assessing the scale of the problem, setting up the periodic evaluation of activities, establishing coordinating bodies at all levels, and planning and evaluating the outcomes of the control interventions.
17.2.2 Administrative controls
This component of TB infection control is more important for you since you need to apply these interventions at the health facility level. As you will read later on, these same interventions are also important in places where people gather and at the level of the household.
Administrative control interventions needed at healthcare facility level are described below:
Triage
The term triage refers to the process of identifying of TB suspects and referring them for investigation. People who you suspect of having TB must be separated from other patients and placed in well-ventilated areas, where the movement of the air is in a direction from non-TB suspects to TB suspects. Instruct TB suspects on cough manners, following advice you will learn about in a moment. Once you have separated the TB suspects from those who do not have TB (i.e. reduced the risk of airborne transmission), you should refer them for diagnosis and treatment.
Why do you think it is important that the movement of air should be in a direction from non-TB suspects to TB suspects?
The spread of TB is largely by inhalation of droplet nuclei containing the bacteria. By making sure non-TB suspects are not downwind from TB suspects you reducing the risk of transmission.
Separation
Separation of potentially infectious patients needs to continue after the process of triage, isolating suspects or confirmed pulmonary TB cases as much as possible. In particular, patients living with HIV and other forms of immunosuppressive illnesses should be physically separated from those with suspected or confirmed infectious TB. Drug-resistant TB suspects or patients should be separated from other patients, including other TB patients. In general, after providing the immediate services that TB suspects and cases might require, try to shorten their stay in the health facility; send them home as soon as possible, in order to minimise exposure for non-infected patients.
Cough manners (or cough etiquette)
In order to minimise the generation of potentially infective droplet nuclei, any coughing patient with a respiratory disease — in particular TB patients or those suspected of having TB — should be educated on good cough manners. The key points of cough manners are listed below and illustrated in Figure 17.1:
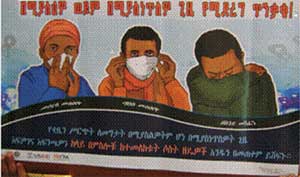
- To cover their nose and mouth when sneezing, coughing or talking by using a gabi, nethela, handkerchief or scarf, piece of cloth, tissue paper and if there is nothing available, place the arm in front of the mouth.
- The same applies to health workers, visitors and families in healthcare (or indeed all places where people gather). Those who cough should cover their mouth and nose with a physical barrier which can be a piece of cloth, a tissue, a surgical mask or an arm placed in front of the mouth.
- The information, education and communication (IEC) activities given at health facilities should strongly focus on cough manners.
- Good respiratory hygiene includes proper disposal of tissue paper, pieces of cloth and masks used for covering the mouth. Proper disposal of sputum should be enforced immediately when a TB suspect is identified. Spitting on floors has to be stopped; collect sputum in a cup and bury it.
Patients and their families should also be educated on the signs and symptoms of TB disease. TB is a treatable disease; explain the risks of not completing treatment. Public health and awareness messages can be delivered as simple posters on the walls and presentations by health educators.
17.2.3 Environmental controls
When environmental controls are implemented, managerial activities and administrative controls need to be in place to ensure proper use and maintenance of equipment and the effective training of staff. The most successful approach is to use the administrative and environmental control measures together. Environmental controls aim to reduce the concentration of infectious respiratory particles in the air. The most important steps are outlined below.
Natural ventilation
A simple but effective approach — and one that is not expensive — is to ensure air from areas where there are TB patients is diluted and moved away from areas where there are patients without TB. This you can do by increasing natural ventilation through open windows and doors, as shown in Figure 17.2.

As a healthworker, always try to be upwind of a TB patient — which should ensure that clean air will flow from behind you towards the patient, rather than the other way round.
Ventilation refers to the removal of old, stale or ‘diseased’ air, and replacing it with new, fresh or ‘clean’ air. This has the effect of removing infectious particles, and diluting those that remain, so that the chances of inhaling infectious particles are kept to a minimum. Good ventilation means that air flows from less contaminated to more contaminated areas, not the other way round.
The important point for you is to ensure that at your health facility, doors and windows should be opened, to encourage natural ventilation.
You might ask the question ‘Is mechanical ventilation (air conditioning) better than natural ventilation?’ The problem with mechanical ventilation is that it is costly, needs regular maintenance, a reliable electricity supply and testing which can be especially difficult for developing countries such as Ethiopia. A research study done in Peru, which measured how much of the air within a room is replaced over a period of time, showed that natural ventilation is almost always more effective in maintaining ventilation than mechanical ventilation.
17.2.4 Personal protective interventions

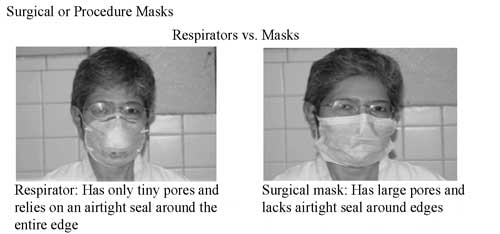
Personal protective equipment helps to prevent the individual healthworker or other TB-free individuals from getting infected. Key items for personal protection against TB are respirators and surgical masks (sometimes called procedure masks) and there are important differences between them (see Figures 17.3 and 17.4).
Respirators
There are different respirators and the most commonly used type in the prevention of TB is the N95 class of respirator (also recommended by the WHO); examples of this type of respirator are shown in Figure 17.3. Respirators have very small pores (too small to see with the naked eye) that allow the wearer to breathe but prevent infectious agents from passing through (they are too big to pass through the pores). Importantly, these respirators form a tight seal around their entire edge so that the air you breathe has to pass through the respirator. Wearing these devices substantially reduces the risk of acquiring a TB infection. Health workers should use respirators when providing care to infectious TB patients or suspects, particularly those individuals who you suspect of having a drug-resistant form of the disease.
It is important that you know how to fit a N95 respirator, ensuring that you have a good seal between the mask and your skin.
Masks
Surgical masks prevent the spread of micro-organisms from the wearer (the surgeon, healthworker or TB patient, etc.) to others by capturing the large wet particles found in the wearer’s breath near the nose and mouth, and also limiting the distance aerosols are expelled when coughing, sneezing and talking. Surgical masks do not provide adequate protection to the wearer from inhaling infectious droplet particles produced by TB patients (Figure 17.4). This is because masks fit loosely over the mouth and nose, which means they allow free entry of aerosols that may be contaminated with M. tuberculosis.
Surgical masks do not adequately protect wearers from inhalation of air contaminated with M. tuberculosis and should not be used for that purpose.
17.3 Infection control where people gather, at community and household level
We can now build on your understanding of the control interventions already outlined at health facility level to look at other places in the community where people gather. You will learn about interventions that operate at the managerial, administrative and environmental level, as well as personal protective interventions, following the structure adopted in the last section. The term congregate settings is used in the following sections of this study session — the term applies to all the types of public place where people gather (or congregate).
17.3.1 Infection control for congregate settings
The recommendations for congregate settings are less specific than those for healthcare facilities, because congregate settings are so diverse. They include a mix of settings that range from correctional facilities and military barracks, to homeless shelters, refugee camps, dormitories and nursing homes. Each facility differs in the type of population it contains and the duration of stay; in turn, this affects the dynamics of TB transmission. Congregate settings are often divided into two categories — long-term (e.g. prisons) and short-term (e.g. jails and homeless shelters) — to reflect the different duration of stay of the inhabitants.
Managerial activities in congregate settings
The full set of national and sub-national managerial activities already described should also apply to congregate settings. This level of activity may involve other ministries besides the Federal Ministry of Health, such as the Ministry of Justice, plus a range of other stakeholders. In any congregate setting, overcrowding should be avoided because it can lead to non-infected individuals being exposed to TB. Any information, education and communication (IEC) material needs to include a specific focus on congregate settings, including the monitoring and evaluation of TB infection control measures at this level.
Administrative controls in congregate settings
The administrative controls used in healthcare facilities were introduced earlier in this study session and they are also equally important in congregate settings. Cough manners and respiratory hygiene should be implemented, as should early identification of TB suspects and cases, followed by separation and proper treatment of infectious cases.
In long-term residential facilities and similar long-stay congregate settings, occupants should be screened for TB before entry. All staff should be given appropriate information and encouraged to undergo TB diagnostic investigation if they have signs and symptoms suggestive of TB. People suspected of having TB should be diagnosed as quickly as possible. In short-term residential congregate settings, such as jails and homeless shelters, a referral system for proper case management should be established.
In congregate settings with a high prevalence of HIV (particularly in correctional services), patients living with HIV and other forms of immunosuppression should be separated from those with suspected or confirmed infectious TB. All staff and persons residing in the setting should be given information and encouraged to undergo HIV testing and counselling. In congregate settings with patients having, or suspected of having drug-resistant TB, such patients should be separated from other patients (including other TB patients), and referral for proper treatment should be established.
Environmental controls in congregate settings
Buildings in congregate settings should fulfil national norms and regulations for ventilation in public buildings, and the specific norms and regulations for prisons, where these exist. In congregate settings in which there is a high risk of TB transmission and where adequate ventilation cannot be achieved, other (mechanical) ways of maintaining ventilation should be adopted.
Personal protective equipment in congregate settings
When a person is a long-term resident and suspected or diagnosed as having TB, but is physically separated from other people, then the same recommendations on personal protective equipment apply as for healthcare facilities (outlined in Section 17.2.4). In short-term residential congregate settings, appropriate strategies for referral should be organised.
17.3.2 Infection control in households
The important steps in effective infection control in households is the early identification of cases, adherence to treatment and implementation of proper TB infection control measures (e.g. cough manners and respiratory hygiene), before and after a diagnosis of TB in a family member. To reduce exposure in households the following additional measures should be taken:
- Houses should be adequately ventilated, by opening doors and windows, particularly rooms where people with infectious TB spend considerable time. Natural ventilation can be sufficient to reduce the likelihood of transmission of infection.
- Smear-positive TB patients should spend as much time as possible outdoors. They should sleep alone in a separate, adequately ventilated room, and spend as little time as possible in congregate settings or on public transport.
- The importance of infection control in the community should be promoted.
- In households with TB patients, additional guidance is important. Cough manners (including use of masks) and respiratory hygiene need to be adopted when in contact with people. Ideally, health service providers should wear respirators when attending patients in confined spaces.
Ideally, family members living with HIV, or family members with strong clinical evidence of HIV infection, should not provide care for patients with culture-positive drug-resistant TB. If there is no alternative, HIV-positive family members should wear respirators, if available. Children below five years of age should spend as little time as possible in the same living spaces as culture-positive drug-resistant TB patients. Such children should be followed up regularly with TB screening and, if positive, should be tested for drug-resistance and treated. If possible, renovation of the patient’s home should be considered, to improve ventilation (e.g. constructing a separate bedroom, or installation of a window or wind catcher, or both).
17.3.3 Community-based TB control
It is useful at this point to remind you of a range of TB control measures that are important at the level of the community. Importantly, these are the community-based TB control measures that need to be coordinated and delivered by you as the health worker and include the following:
- Create community awareness about TB transmission, the treatment of TB and the prevention methods used to stop the spread of the disease
- Identify and refer TB suspects in the community as early as possible
- Provide BCG vaccine to children at birth
- Refer TB patients for sputum examination or arrange for sputum collection
- Monitor adherence to prescribed anti-TB drugs during the intensive and the continuation phases of treatment
- Keep records on what you are doing for TB control
- Trace patients who miss doses or default on medication and ensure medication is resumed
Ensuring that treatment is resumed reduces the risk that the patient will develop Multi-Drug Resistant TB.
- Give support for patients throughout the course of treatment
- Ensure TB/HIV co-infection patients benefit from both programmes; advise TB patients to be screened for HIV and HIV-positive patients to be screened for TB
- Coordinate TB control activities of volunteers/model families in their kebeles and report their monthly activities.
17.3.4 Information, education and communication (IEC)
The aim of communication is to increase awareness of the community regarding basic information about tuberculosis. By giving adequate information about this disease and raising levels of community awareness you can influence what is socially normal and acceptable. This has an impact on TB control; it also changes behaviour in both individuals and groups of people. It is a good idea to involve previously treated and cured TB patients in what you do — they can help improve communication and counselling between people with TB, their families and providers.
Do all you can to ensure that the community you are part of is well-educated about TB infection, prevention and control. Patients should understand that they should know their HIV status, that they may be eligible for isoniazid preventive therapy (IPT) and have a right to rapid TB diagnosis and treatment. They should know that TB can be spread by coughing and they should be encouraged to adopt good coughing manners. IEC campaigns should include messages such as ‘Our community is TB-safe’ or ‘Our health facilities are stopping TB’, which will help create a positive and forward-looking attitude in your community that you will have helped to establish.
Summary of Study Session 17
In Study Session 17, you have learned that:
- TB infection control is a combination of measures aimed at minimising the risk of TB transmission within the population. Its foundation is the early and rapid diagnosis of people with TB and their proper management.
- TB infection control is part of the national infection prevention and control policies for health in general. It also extends the national policy by targeting airborne infections.
- The interventions of TB infection control fall into four main categories; managerial, administrative, environmental, and personal protective interventions.
- Managerial activities involve assessment, establishing coordinating bodies at all levels and planning and evaluating the performance of infection control interventions.
- Administrative controls include policies and procedures which promptly identify potential and known infectious cases of TB, separating and treating them with minimal delay.
- Natural ventilation is a simple, but effective and inexpensive environmental technique to move and dilute air from TB-patient areas away from people without TB, by maximising airflow through open windows and doors.
- The use of personal protective equipment, such as respirators and masks, helps to protect healthworkers from airborne transmission of TB. They should also follow standard precautions for infection control.
- Healthworkers have an important role in community-based TB control, especially in identifying TB suspects and guiding, supporting and following-up patients during treatment.
- Healthworkers can make an important contribution to TB control in their communities by providing information and education (for example, about cough manners) and communication more generally, helping to change social norms and behaviours.
Self-Assessment Questions (SAQs) for Study Session 17
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 17.1 (tests Learning Outcomes 17.1, 17.2, 17.3, 17.4 and 17.6)
- a.What is meant by TB infection control?
- b.What are the standard (universal) precautions that should be taken when dealing with TB suspected cases?
Answer
- a.TB infection control is a combination of measures aimed at minimising the risk of TB transmission.
- b.Standard universal precautions include:
- hand washing and antisepsis
- use of personal protective equipment (e.g. gloves)
- appropriate handling of patient care equipment and soiled cloths
- prevention of needle stick/sharp injuries
- environmental cleaning and spills management
- appropriate handling of clinical waste.
SAQ 17.2 (tests Learning Outcomes 17.4, 17.5 and 17.6)
- a.What administrative control interventions are needed for TB control at the level of the healthcare facility?
- b.What are the personal protective measures you would recommend for a healthworker giving care to drug-resistant TB patients in their homes?
Answer
- a.Administrative control interventions needed at healthcare facility level are: triage (identify TB suspects and refer them for investigation), physical separation (cohorting) or isolation of patients or TB suspects, cough manners and minimizing time spent in healthcare settings.
- b.Respirators for health workers and surgical masks for the patients.
SAQ 17.3 (tests Learning Outcomes 17.3, 17.4, 17.5 and 17.6)
What community-based TB control measures could you use in your village to limit the spread of TB? Try to think of at least five ways you could help to reduce TB in your community.
Answer
You could use the following measures:
- Create awareness about TB on routes of transmission, diagnosis, treatment and prevention.
- Identify and refer TB suspects to a higher health facility for diagnosis and treatment.
- Educate on TB vaccination (BCG), cough manners and respiratory hygiene.
- Supervise TB treatment for patients on anti-TB drugs.
- Keep TB patients’ records updated.
- Advise TB patients to have HIV screening and HIV patients to have TB screening.
- Involve the community members and previous TB patients in TB awareness and prevention campaigns (advocacy, communication, social mobilisation).