Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Monday, 6 July 2026, 11:08 PM
Communicable Diseases Module: 19. Leprosy Treatment
Study Session 19 Leprosy Treatment
Introduction
As you learned in Study Session 18, early detection combined with prompt treatment is an effective way to prevent the spread of leprosy in the community. In this study session, you will learn how to treat a leprosy patient, monitor treatment progress, what you need to do if a patient interrupts treatment and what kind of advice you can give to a patient or a family member while a patient is on treatment.
Multidrug therapy (MDT) kills the bacteria responsible for leprosy and stops the spread of the disease. Leprosy patients can lead completely normal lives and if the disease is detected early and treated with MDT, leprosy need not lead to disabilities. In this study session you will learn about how to detect and manage leprosy complications to alleviate the sufferings of your patients.
Learning Outcomes for Study Session 19
When you have studied this session, you should be able to:
19.1 Define and use correctly all of the key words printed in bold. (SAQs 19.1, 19.6 and 19.8)
19.2 Explain how you would classify leprosy patients for the purpose of treatment. (SAQ 19.2)
19.3 Explain key features of leprosy treatment and management. (SAQ 19.3)
19.4 Explain how you would identify and manage patients who interrupt or default from leprosy treatment. (SAQ 19.4)
19.5 Describe how you would inform leprosy patients and supporters about their treatment in an effective way. (SAQ 19.5)
19.6 Describe how you would discharge leprosy patients after completion of treatment. (SAQ 19.6)
19.7 Describe the main complications of leprosy and what actions you would take. (SAQ 19.7)
19.1 Classification of leprosy
Classification of leprosy patients is based on the clinical features (see Table 19.1). The World Health Organization (WHO) distinguishes between two major types, one of which (multibacillary leprosy) was introduced in Study Session 18. Paucibacillary leprosy is characterised by the low number of skin lesions and the low number (or absence) of visible Mycobacterium leprae in microscope slides taken from these patients.
| Clinical features | Paucibacillary (PB) | Multibacillary (MB) |
|---|---|---|
| Skin lesions | One to five lesions | Six or more lesions |
| Nerve damage | Only one nerve involved | Two or more nerves involved |
Paucibacillary is pronounced pore-see-bass-ill-ary’. Pauci comes from the Latin word meaning ‘few’.
19.2 Multidrug therapy (MDT) for the treatment of leprosy
Multidrug therapy (MDT) is the treatment of choice for all leprosy patients. It entails the swallowing of a combination of anti-leprosy drugs on a daily basis, in the recommended doses for the recommended duration of treatment and according to the WHO leprosy classification.
19.2.1 MDT drug regimens
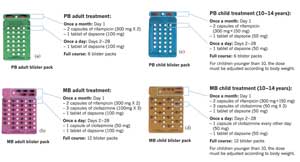
The drugs used in MDT leprosy treatment are rifampicin (R), dapsone (D) and clofazimine (C). There are two MDT regimens: PB-MDT for paucibacillary patients and MB-MDT for multibacillary patients, in dosages for adults and for children in blister packs; see Figure 19.1(a) to (d). Each blister pack contains treatment for four weeks.
Regimen is the term used to describe the drug dosages, the number of times the drugs are taken in any given period (e.g. per day), and the duration of treatment in days, weeks, months or years.
19.2.2 How to administer MDT for leprosy
Box 19.1 summarises how to administer multidrug therapy to treat leprosy.
Box 19.1 Before giving MDT you should:
- Count the number of skin patches and check nerve involvement in order to classify the patient as PB or MB for treatment, (see Table 19.1 above and Figure 19.2). If in doubt, classify as MB.
- Inform the patient and anyone accompanying the patient about the disease and its treatment. Encourage them to ask questions and clear up any doubts.
- Give the patient the first dose at home or in the Health Post under your supervision. Show them which drugs from the MDT blister pack should be taken every day for days 2–28. Give the patient enough blister packs to last until the next visit.
- Give patients the full course of treatment if it is difficult for you to visit them at home, or for them to come to the Health Post. Explain to them what they have to do (see later in this study session).

19.2.3 Accompanied MDT
Normally, patients are given their MDT drugs every month when they come to the health facility for the next blister pack and their check-up. However, this is not always possible. Accompanied MDT is a type of treatment strategy where a patient is able to receive all the MDT drugs needed for the full course of treatment on their first visit after diagnosis. It is designed to address a frequent problem in rural programmes. Patients often have to interrupt their treatment because of a shortage of drugs at the health centre, poor access to the health services or simply because no one is at the health centre when they come to collect their drugs.
This approach means that the patient has to take more responsibility for adherence to the drug regimen, although a treatment supporter should accompany the patient when they collect the drugs. If the patient chooses accompanied MDT, give PB patients six PB blister packs and MB patients 12 MB blister packs. Reassure patients that they can lead normal lives. Tell patients to report any problems and to come back when treatment is completed.
Yacob, a new leprosy patient, lives two streets away from a health centre. Should he be given accompanied MDT or not? Explain your answer.
No. He is close to the health centre and is likely to be able to collect more drugs when he needs to.
19.2.4 Side-effects of anti-leprosy drugs
Serious side-effects of leprosy treatment are rare. The most serious side-effects are serious allergy to one of the drugs, or jaundice (yellowness of the eyes). If either of these happens, you should stop the treatment and refer the patient to a clinician. Whenever you refer a patient, write down details of the complaint, when this first occurred and medicines taken. Send this referral note with the patient to show to the clinician.
The patient may have other, less serious side-effects such as rifampicin turning urine red, or black spots on the skin due to dapsone, or change of the colour of the skin due to clofazimine. When this happens it is important to continue the treatment. You should let the patient know that they are not serious side effects and will go away when the treatment is finished.
19.3 Identifying and managing defaulters
A defaulter is an individual who fails to complete treatment within the maximally allowed period of time. Whenever a PB patient has missed more than three months treatment, or an MB patient more than six months treatment, they should be declared as defaulters from treatment and should be referred immediately to the clinician for further management. Any defaulter, particularly one who remains very irregular on treatment and repeatedly defaults despite every effort on the part of the health staff, should also be referred, so that a more experienced person can decide if further treatment is required and if so, how much.
You have an important role to play in helping prevent patients from interrupting treatment and becoming a defaulter. You can also retrieve a defaulter — taking steps to bring patients back into treatment by getting information about those who fail to show up on clinic day, by asking other patients or by sending a reminder directly to the patient. But if she/he does not turn up after 28 days, you should visit him/her at home to find out the reason for non-attendance. Then you should complete the defaulter retrieval form (make sure you know where these forms are located in your place of work) and take any other appropriate action, such as referring the patient to a clinician for assessment.
There are a number of ways in which you can help ensure that patients keep to their treatment until completion. You should always inform patients of what’s required by way of treatment and why, and you should make sure that drug collection is accessible and flexible. Giving medicines regularly and identifying and referring patients with complications promptly are also important. Also, you should try to trace patients who miss a drug collection date or clinic day, carry out regular patient’s review and discuss findings with them during clinic visits. As a Health Extension Practitioner, you have a big responsibility for helping to motivate patients by adopting a professional attitude and by using encouraging words. Box 19.2 summarises the key points you need to remember for patients and their families.
Box 19.2 Key points for patients and their families
- Educate patients, their families and the public about leprosy treatment.
- Ensure that patients adhere to treatment and that they get the support and encouragement they need.
- Tell patients and their families that leprosy is curable, and the drugs help stop the disease from spreading.
- Tell patients to keep the drugs in a safe, dry, shady place and out of the reach of children.
- Make sure patients know that if the drugs are spoiled (change colour or broken), they will be replaced, as MDT drugs are free of charge.
- Make your patients aware that leprosy drugs can turn their urine red or skin darker, but they should not worry if this happens because it will go away when treatment is completed.
- Tell your patients that MDT is safe during pregnancy, and safe for patients being treated for tuberculosis (TB) and those who are HIV-positive.
- Make sure patients tell you about any problems and that they come monthly for their check-up and to collect their medicines.
19.4 Discharging patients after treatment
Finally in this section, what about discharging leprosy patients after completing MDT treatment? Remember that MDT is therapy of fixed duration. When six doses of PB-MDT have been completed stop the treatment, examine the patient and record all clinical findings. Then refer the patient to the health centre for discharge as treatment is completed. Do the same when 12 doses of MB-MDT have been completed by MB patients.
19.5 Leprosy complications and management
You will remember that you learned in Section 18.1.1 that leprosy reactions are the body’s immune response to the leprosy bacteria and are natural reactions as part of the normal course of the disease. Your patients need to understand that reactions are not adverse side-effects of MDT and do not mean that the disease is becoming worse or that the treatment is not working. Reactions can occur before, during or after the discharge of the patient from treatment.

19.5.1 Signs and symptoms of leprosy reactions
The symptoms and signs of inflammation in a leprosy patient include the appearance of new skin lesions, redness and/or swelling of skin lesions, swelling and/or increased tenderness of the skin lesions, plus the appearance of tender nodules in the skin. Figure 19.3 shows typical reactions of this type in two patients.
Other reactions relate to the affected nerves; there can be swelling and tenderness of peripheral nerves, with or without loss of nerve functions, and sudden nerve function impairments or loss, such as weakness of muscles of the hands and feet or inadequate closure of eyelids, due to untreated inflamed nerves. You will recall that you learnt about nerve examination in Study Session 18, so that you are able to spot signs and symptoms such as these and take appropriate steps by referral to a clinician.
19.5.2 Managing leprosy reactions
A range of factors can lead to or help bring about leprosy reactions. They include stressful conditions such as pregnancy and childbirth, acute infections, vaccination, physical exhaustion, mental stress and strain. You should be on the lookout for the presence of any of these conditions — including asking your patients directly about problems they face.
![]() Refer patients with leprosy reactions urgently to a higher health facility.
Refer patients with leprosy reactions urgently to a higher health facility.
If a patient has any of the symptoms or signs of reaction, refer them immediately to a higher level health centre or hospital for appropriate management. Reactions require urgent treatment with special medicines as they can lead to irreversible deformities. Give aspirin or paracetamol to reduce pain and fever, but stress that it is important that patients continue to take MDT while they go to the higher health facility.
19.5.3 Disability
Disability in leprosy is an inability to perform some or all of the tasks of daily life. The disabilities associated with leprosy are mainly due to nerve damage. As you learned in Study Session 18, some nerves are responsible for the movement of the hands or feet or closure of the eyelids; others signal the sensation of pain, hotness or coldness, or trigger sweating in the skin. When leprosy reactions go untreated for a few months, they may result in damage of nerves which control the functions of the hands, feet or eyes; you saw some examples of these in Figure 18.1 in the previous study session. Primary nerve damage can lead to complications, which in turn affects other nerves (so-called secondary nerve damage); for example:
- Dryness of skin, leading to cracked skin, which may become infected.
- Loss of sensation, which may lead to ulcers (areas of damaged infected tissue that won’t heal, usually on the legs).
- Weakness or paralysis, which may lead to ‘claw’ fingers or toes.
You should watch out for reduced skin sensation, impaired nerve function such as weakness in the hands or feet and/or eye closure, which you can detect using simple observation and history-taking; you learnt about voluntary muscle tests (VMTs) and sensation tests (STs) in Study Session 18. Where you see such indications of damage, refer the patients to the clinician for advice on how to manage them. You can prevent primary nerve damage by early diagnosis, prompt and adequate treatment and by regular VMTs and STs. Secondary complications can be prevented by teaching patients how to carry out self-care, which we will discuss in more detail shortly.
19.5.4 Measures to prevent and manage disabilities
Patients with insensitive hands or feet injure themselves without noticing it. They can develop wounds which can get infected and, over time, lead to irreversible deformities. It is the task of all health staff working with leprosy patients to preserve nerve function and to prevent further deformity and disability in those cases where there is some irreversible disability present at the time of diagnosis. The process and measures undertaken to preserve nerve function is often referred to as prevention of disabilities (POD) by:
- Early diagnosis and prompt treatment.
- Recognising signs and symptoms of leprosy reactions with nerve involvement and referring to a clinician for advice on what to do.
- Carrying out VMTs and STs regularly to detect nerve function impairment.
- Encouraging and training patients in the practice of self-care.
- Educating patients to recognise early signs of nerve function impairment and to report this immediately.
POD depends, to a very large extent, on the patients themselves. So, priority should be given to POD through training on self-care, i.e. what the patients can do themselves to prevent development and/or worsening of disabilities and by wearing protection on feet and hands. You should tell leprosy patients with insensitive feet not to wear closed plastic shoes because such shoes can lead to more sweating, formation of blisters and skin infections in the feet. Where wounds occur, you should manage them just like any other cuts or wounds, dry skin, or eye problems. Use Table 19.2 to guide you on simple measures you can take to prevent and manage disabilities at the community or health post level. Use it to teach your patients about self-care.
| Care of the hands | |
|---|---|
Injury on hand while working/cooking | Clean wound and apply clean dressing. Advise rest. Advise and teach patient to use a cloth to protect the hands when touching hot or sharp objects. |
Hands with dry cracks and fissures | Advise and teach patient to soak hands for 20 minutes every day in water and to apply Vaseline or cooking oil regularly. |
| Care of the feet | |
Feet with dry cracks and fissures | Advise and teach patients to soak their feet for 20 minutes every day in water and apply cooking oil/Vaseline regularly. Advise them to use shoes or slippers to protect their feet from injury.  Source: WHO, 2000, as for Figure 19.1 |
Blister on the sole or between toes | Dress blister with clean cloth. Apply cotton wool and bandage. Teach patient how to do the same. |
Feet with ulcers without any discharge | Clean the ulcer with soap and water. Cover with clean dressing. Advise rest. |
| Feet with ulcers with discharge | Clean the ulcer. Apply antiseptic dressing. Advise rest. If no improvement in four weeks, refer to hospital. |
| Care of the eyes | |
Patient presents with red eye, pain, blurring of vision and discharge | Give aspirin or paracetamol. If available apply 1% atropine drops and steroid ointment. Keep eye covered with a pad. Whenever possible, advise to go to the hospital. |
Patient with injury on cornea (corneal ulcer) | Apply antibiotic ointment if available. Keep eye covered with a pad. Wherever possible, advise to go to the hospital. |
Summary of Study Session 19
In Study Session 19 you learned that:
- Leprosy is a disabling disease and complications can occur before, during and after treatment.
- Patients are classified using WHO guidelines into paucibacillary (PB) and multibacillary (MB) for the purpose of treatment with multidrug therapy (MDT).
- Prompt treatment with MDT is an effective way to prevent the spread of leprosy in the community. The duration of treatment for PB and MB patients is 6 and 12 months respectively.
- If detected early and treated with MDT, leprosy will not lead to disabilities. Leprosy patients can lead completely normal lives.
- Patients can collect their treatment at regular intervals from you or from the health centre, or (with accompanied MDT) take the entire course away with them when diagnosed.
- As a health worker, you have an important role to play to ensure treatment adherence and completion and prevent patients from defaulting from treatment.
- Leprosy patients can develop reactions, as part of the natural course of the disease. Urgent treatment is essential, otherwise irreversible impairments (e.g. reduced or partial loss of nerve function in the hand, foot or eye, along with loss of sensation, weak grips, impaired vision), or deformities (total or partial loss of hand, foot or eye functions, clawed fingers and toes, partial or total blindness) will develop.
- Many complications of leprosy are due mainly to nerve damage and occur when reactions go untreated for a few months. The main result is damage of nerves which control the functions of the hands, feet or eyes.
- Disabilities can be prevented and managed by early diagnosis and prompt treatment, plus a range of simple protective measures requiring patient self-care of the hands, feet and eyes.
Self-Assessment Questions (SAQs) for Study Session 19
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 19.1 (tests Learning Outcomes 19.1 and 19.2)
How would you classify the following leprosy patients?
- a.Tesfaye with four skin lesions and weakness of both hands.
- b.Hiwot has three skin lesions with loss of sensation.
- c.Getachew reported with five skin lesions and inability to close his eyelids.
Answer
First, count the number of skin patches and check whether a peripheral nerve is involved in order to classify the type of leprosy into PB or MB (Section 19.1). If in doubt, classify as MB.
- a.Tesfaye is MB because he has four skin lesions and weakness in both hands, which is a sign of nerve involvement.
- b.Hiwot is PB because she has only three skin lesions.
- c.Getachew is MB because he has five skin lesions and eyelid gap, an indication of involvement of the nerves serving both eyes.
SAQ 19.2 (tests Learning Outcome 19.3)
What is the correct treatment for each of the following leprosy patients? Classify each person for either PB-MDT or MB-MDT and explain why you reached your decision.
- a.Bizuwork has four skin patches located on the right upper arm.
- b.Ato Mesele complains of weakness in both hands and there is also a big skin patch on his back.
- c.Yohanes has three skin lesions on his back and two lesions on his face, but no muscle weakness.
Answer
First determine the classification of the leprosy patient, then decide whether to give PB- or MB-MDT.
- a.Bizuwork is a PB patient because she has four skin lesions. She should be given PB-MDT.
- b.Ato Mesele is an MB patient because although he has only one skin patch he also has weakness in both hands (an indication that the nerves responsible for movements of both hands are involved). He should receive MB-MDT treatment.
- c.Yohanes has a total of five skin lesions and no muscle weakness. He is a PB patient and should receive PB-MDT.
SAQ 19.3 (tests Learning Outcome 19.3)
What would you do when a leprosy patient on treatment comes to you for a monthly visit and why?
Answer
You should ask the patient how she/he feels and whether she/he has any complaint since the last visit. Then carry out VMT/ST and record your findings. Then inform the patient about treatment, looking for feedback to check what you say has been understood and clarify any issues the patient may raise. Finally, give/supervise and record the first dose of MDT for the new month, give the patient the blister pack, and remind the patient to inform you about any complaints during the month.
SAQ 19.4 (tests Learning Outcome 19.4)
Briefly describe all the actions and attitudes of healthworkers like you that will help to prevent your leprosy patients from defaulting.
Answer
You can prevent patients from defaulting by giving medicines regularly and informing the patient about what is required. In addition, make drug collection accessible and flexible, identify and refer patients with complications promptly. It is also important that you trace patients who miss a drug collection date or clinic day, carry out regular patient reviews and discuss any findings or concerns during clinic visits. Overall, you need to display an encouraging and positive attitude, to help motivate patients.
SAQ 19.5 (tests Learning Outcome 19.4)
Hailemariam started MB-MDT treatment eight months ago under your care but has not collected his MDT drugs in the last three months due to illness. He returns to see you today. What should you have done before now? What will you do today?
Answer
Before now, you should have visited him at home to find out why he has been absent from treatment and discuss how to prevent future treatment interruption. You should have reminded him about the need to keep treatment appointments to avoid worsening of illness and possible resistance of the bacteria to treatment.
On his return today, you should ask him about the progress of treatment and carry out a physical examination. Remind him that he has to complete the remaining seven blister packs within 11 months without fail. Tell him to always inform you in advance if he needs to be away from home so that you can give him his medicines for self-administration for the anticipated period of absence.
SAQ 19.6 (tests Learning Outcomes 19.1 and 19.5)
How would you educate a leprosy patient who is about to commence MDT?
Answer
Look back at Section 19.1 to check your recall of what to do; see how many of the following points you have remembered. You need to:
- Educate patients about leprosy treatment to ensure that she/he adheres to the treatment plan.
- Tell patients that leprosy is curable, and the drugs stop the disease from spreading.
- Remind patients to keep the drugs in a safe, dry, shady place, out of the reach of children.
- Mention that if the drugs are spoiled (change colour or broken), they will be replaced, as MDT drugs are free of charge.
- Tell your patients that leprosy drugs can turn their urine red or skin darker, but they should not worry because this will go away when treatment is completed.
- Make sure your patients know that MDT is safe during pregnancy, for patients being treated for tuberculosis (TB) as well as those who are HIV-positive.
- Ask your patient to inform you when they notice any problem and that she/he will be seeing you monthly for a check-up and to collect MDT.
SAQ 19.7 (tests Learning Outcome 19.6)
What should you do before discharging a leprosy patient from MDT treatment?
Answer
Prior to discharge from MDT you should examine the patient and record all clinical findings.
SAQ 19.8 (tests Learning Outcomes 19.1 and 19.7)
John has been on MB-MDT treatment for six months. He has come to you today to complain of redness and pain in his skin lesions. He feels unwell and has not been able to go to the farm for four days. What is wrong with John? What would you do and why?
Answer
Redness and pain in skin lesions of a leprosy patient are signs/symptoms of a leprosy reaction. So, in John’s case you should inform him about his sickness, as you learnt in Section 19.3, then give him some aspirin or paracetamol tablets to relieve his pain, before referring him to a clinician for immediate management. John must continue to take MDT. If possible, you should accompany him to the clinic.