Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Tuesday, 21 July 2026, 9:41 PM
Hygiene and Environmental Health Module: 21. Latrine Utilisation – Changing Attitudes and Behaviour
Study Session 21 Latrine Utilisation – Changing Attitudes and Behaviour
Introduction
There is poor utilisation of latrines among individuals and families in some communities in Ethiopia. In the previous study session, you have learned about the alternative types and construction of latrines. In this study session, you will learn how to encourage latrine utilisation. You will be able to identify and take into account the factors that may influence people against using latrines. Involving model families to share their experiences and participate in regular inspections will help households to properly use their latrines, to seek technical advice when they need it and to solve any problems they encounter. The purpose of this study session is to teach you about approaches that are currently being used to achieve behavioural changes of individuals, families and communities towards good practice of hygiene and sanitation.
Learning Outcomes for Study Session 21
When you have studied this session, you should be able to:
21.1 Define and use correctly all of the key words printed in bold. (SAQ 21.1)
21.2 Identify various factors that affect the utilisation of latrines and handwashing facilities. (SAQ 21.2)
21.3 Describe ways of motivation used to enhance latrine utilisation. (SAQ 21.2)
21.4 Explain to selected model families, how to share their experiences of latrine utilisation to others. (SAQ 21.3)
21.5 Describe some approaches to community behaviour change. (SAQ 21.4)
21.6 List the tools used to conduct baseline surveys and regular inspections of latrine utilisation. (SAQ 21.5)
21.1 Benefits of hygiene and sanitation behaviour change
In the previous sessions of this Module you have learned that proper hygiene, adequate sanitation and safe drinking water have significant benefits for human health. You have also learned about the need to practise positive behaviours. Any change from bad habits to good practice is described as behaviour change.
When are the critical times for a person to wash his/her hands?
Critical times for handwashing are after visiting the latrine, after cleaning a child’s bottom, before preparing food and before eating meals or feeding children.
Promotion of hygiene and proper sanitation is the single most important way to improve the health of your community (Figure 21.1). However, the right approaches need to be used to change behaviour and get people to take better care of themselves, their family’s health and their environment. As health is an asset to a community, its improvement enhances economic development and brings wealth to a society.
Did you know? A gram of human faeces can contain 10 million viruses and 1 million bacteria.

21.2 Factors affecting the use of latrines and handwashing facilities
21.2.1 Latrines
The possession of an improved latrine, on its own, will not halt the transmission of faeco-orally transmitted diseases among the people of your community. For this to have an impact on health, the people have to use their latrines and handwashing facilities effectively.
What factors do you think affect the utilisation of latrines in your community?
There are several possible answers including the bad smell of a latrine, lack of privacy if the shelter is inadequate, childhood habits that are hard to break and many more.
The factors will vary from place to place depending on the local context. Behavioural, demographic, geographic, climatic, social, cultural and economic reasons can deter families from using latrines. For example, elderly or uneducated people in rural areas may find it difficult to get used to new technologies and may resist the adoption of new behaviours. In some local cultures, people may not want to share latrines with others; for example, women may not want to share the same facility as their father-in-law and there are some cultural practices that inhibit the use of one latrine by both the husband and wife. Children’s faeces are often mistakenly considered not to be a potential health hazard and it may be considered unimportant for children to use the latrine. Household members may be discouraged from using the latrine at night because of the fear that ‘evil’ or ‘devils’ inhabit the latrine during that time. Another factor is the misconception that prevails among some farmers that using the ‘cat-system’ (i.e. burying excreta or leaving it open in a field) will improve the soil condition.
There are other more practical reasons such as the use of inappropriate materials for latrine construction, the collapse of latrines due to termites, flooding problems or loose soil conditions, and the need for frequent maintenance.
You need to identify the factors affecting the use of latrines that are relevant in your community. Once these are defined, then you can discuss them in a transparent way. Open discussion of these issues within the community will ease the construction and use of latrines.
21.2.2 Handwashing facilities
Despite the health benefits, some family members in rural households may not practise proper handwashing.
Why do you think that some people in your village don’t wash their hands properly?
Possible reasons include they can’t afford to buy soap, they have a poor attitude to handwashing and can’t be bothered to do it, they lack the utensils and equipment, the inappropriate placement of the handwashing facility or lack of water, but other reasons are also possible.
You should focus on individual and communal communication to change the attitude of people towards the direct (health) and the indirect (economic) benefits of handwashing. You can recommend the use of locally available materials such as ash for detergent purposes, and tin cans or jerrycans as handwashing devices (as described in Study Session 20). You can check that the handwashing facility is conveniently placed near latrines and that the water is clean to avoid further contamination.
21.3 Motivating people to change their behaviour
Health education is frequently delivered by someone lecturing about hygiene and sanitation in health facilities and community gatherings. However, such an approach is not recommended as the sole means to achieve individual behaviour change. Because human behaviour is influenced by the surrounding environment and social context, specific messages instead of universal messages of hygiene and sanitation are more important. Hygiene messages must be contextually and culturally suitable, and comfortable, for your community.
If you are trying to change behaviour by targeting individuals, you need to consider not only their prior experience but also their learned behaviours. These are the habits gained by social learning channels, i.e. from parents, friends and opinion leaders in their community. Each individual has their own beliefs, values and knowledge about health practices. People may ask themselves, before adopting a new behaviour, if the new practices are going to fit with their ideas and way of life. They need to be convinced that there will be important benefits from changing their behaviour.
Different motivational techniques can be used to good effect (see Box 21.1).
Box 21.1 Case study: Reasons for building latrines
In villages of Achefer woreda, different promotional techniques were used to encourage households to build pit latrines. Community members were asked which of these techniques was most effective. They were asked to choose the three most important reasons out of seven techniques that had been used. Table 21.1 shows the responses from 300 people.
| Rank | Motivator/Reason | Points | % |
|---|---|---|---|
| 1 | House-to-house promotion of latrine building | 92 | 31.3 |
| 2 | Coffee ceremony to bring people together for discussion | 73 | 24.8 |
| 3 | Rewarding good practice with a coloured flag to be publicly displayed | 39 | 13.3 |
| 4 | Government enforcement | 36 | 12.2 |
| 5 | Influence of friends and neighbours (peer pressure) | 27 | 9.2 |
| 6 | Video show that demonstrated positive behaviour by others | 23 | 7.8 |
| 7 | Fear of being publicly shamed | 4 | 1.4 |
House-to-house promotion by Health Extension Practitioners and health promoters, and holding coffee ceremonies specifically for hygiene promotion, were more effective than other methods in Achefer. Health promoters, including you, should use all possible ways of hygiene promotion in order to bring positive behaviour at community level.
In order to have an impact on health, any change in health practice needs to be adopted by many individuals in your community. Shared behaviour is only achieved when the community members themselves feel there is a problem, and are motivated to solve the problem by jointly taking actions that would permanently improve health conditions.
21.3.1 Using model households
Model households and families, also known as household models or role models, provide a valuable opportunity for you for to improve the exchange of learned behaviours to others. These households are often early adopters of new behaviours. You can select and recruit these families on the basis of their expressed interest and willingness to be involved in the promotion of hygiene and sanitation.
Your role would be to ensure they have the necessary knowledge and skill, and develop the right attitude, to help other households in learning about hygiene and sanitation. It is also important that model households are recognised and rewarded by the community leaders, both traditional and formal, and acknowledged by community members, friends and neighbours in order to sustain the existing achievements and encourage others to progress well.
21.3.2 Community motivation
UNICEF uses the term Community Approaches to Total Sanitation (CATS) to encompass a range of different community-based sanitation programmes. The aim of these approaches is total sanitation which means the complete separation of wastes from humans, i.e. no open defecation and 100% of excreta to be hygienically contained. An important goal for villages and other communities is to achieve open defecation free (ODF) status. Box 21.2 summarises the key elements of CATS.
Box 21.2 Essential elements of Community Approaches to Total Sanitation (CATS)
- CATS aim to achieve 100% open defecation free (ODF) communities through affordable, appropriate, acceptable technology and behaviour change.
- CATS depend on broad engagement with diverse members of the community, including households, schools, health centres and traditional leadership structures.
- Communities lead the change process and use their own capacities to attain their objectives.
- Subsidies – whether funds, hardware or other forms – should not be given directly to households.
- CATS support communities to determine for themselves what design and materials work best for sanitation infrastructure rather than imposing standards.
- CATS focus on building local capacities to enable sustainability.
- Government participation from the outset – at the local and national levels – ensures the effectiveness of CATS and the potential for scaling up.
- CATS have the greatest impact when they integrate hygiene promotion into programme design.
- CATS are an entry point for social change and a potential catalyst for wider community mobilisation.
The next section describes two particular approaches to community motivation that are becoming increasingly popular throughout the developing world.
21.4 Two approaches to communal behaviour change
Participatory Hygiene and Sanitation Transformation (PHAST) and Community-Led Total Sanitation (CLTS) are among the CATS techniques used to achieve total sanitation. These methods introduce community mobilisation and behaviour change as their core principles to improve sanitation and integrate hygienic practices.
Traditional methods of sanitation and hygiene promotion were teacher-driven, i.e. the educator taught by lecture and the community listened passively. CATS approaches are demand-driven, community-led and emphasise the sustainable use of user-friendly, affordable and safe sanitation. The following sections outline the basic principles of PHAST and CLTS but to be a facilitator of these techniques requires further study and training to develop the skills required. Such training might be sought from NGOs involved in water and sanitation (also known as WASH) projects.
21.4.1 Participatory Hygiene and Sanitation Transformation (PHAST)
PHAST is a widely used community approach to hygiene promotion. It uses participatory techniques to promote good hygiene behaviours, sanitation improvements and community management of water supply and sanitation facilities. It is derived from a community appraisal method of health practice that, in the process, empowers community members (participants) to be able to identify their community problems. Community appraisal is a process for analysing the existing community health problems by mapping water and sanitation, and identifying good and bad hygiene behaviour in relation to community hygiene practices and the spread of diseases. Figure 21.2 shows PHAST participants involved in group discussion and Figure 21.3 represents a group using a map they have drawn to identify the sanitation problems.
 |  |
| Figure 21.2 PHAST Community conversation. (Source: Addis Continental Institute of Public Health Students presentation, 2010) | Figure 21.3 PHAST participants looking at WASH mapping. |
The next step in the process is for participants to make plans for solutions. During this planning process, they will look at the ways of blocking the paths for the spread of disease. Men and women share the tasks and select options for sanitation improvements and improved hygiene behaviour. This is followed by identifying who does what and noting what might go wrong. They also put in place the monitoring and evaluation process. Monitoring is meant to check the progress of the implementation of WASH activities, while evaluation looks at what improvements (health, social or economic) were brought about at community level. In all these steps, the facilitator’s role is to guide the participants as they work through the PHAST process.
Box 21.3 describes a case study of the PHAST process.
Box 21.3 Case study: PHAST in Amba kebele
Tsehaye is a Health Extension Practitioner in Amba kebele. The kebele does not have adequate access to improved drinking water. A baseline survey of giardiasis prevalence was conducted and was found to be 25% among children under 10 years old.
Tsehaye had received training in the PHAST approach so that she could train others. She decided to put this training to good use and trained nine village volunteers in hygiene promotion specifically aimed at the prevention of giardiasis. These volunteers then mobilised 2,500 community members, both adults and children, in the kebele. During the training, the community members identified the bad behaviour they were aware of (such as open field defecation, disposal of child faeces in open spaces, not washing hands after visiting latrines and after cleaning a child’s bottom). The community members, with the help of the nine village volunteers, planned to avoid those bad practices and in contrast, adopt and sustain good behaviour. The training and community mobilisation continued for one year. People started to change their behaviour as a result of increased awareness and a positive attitude towards healthy behaviour. Consequently, the prevalence of giardiasis among children in the Amba community was reduced to 10%.
Amba kebele is now planning to achieve open defecation free status within the coming 3–6 months. The achievement of Tsehaye and the volunteers was recognised and they took the best practitioner prize of the year from the kebele leader. They are highly motivated to work more to overcome the public health challenges in Amba kebele.
This case study demonstrates the use of PHAST as a tool for identifying the community WASH problems, planning the solutions and finally monitoring and evaluating the WASH performance. You should notice that the focus of PHAST is always on the involvement of the community to determine and solve its problems.
21.4.2 Community-Led Total Sanitation (CLTS)
CLTS aims to bring community-wide elimination of open defecation by raising awareness and promoting affordable technology options. NGOs, multinational organisations and government health programmes in many countries in developing regions of the world (including Ethiopia) are adopting this approach. It has become the most successful community approach to total sanitation.
Like PHAST, the core principle of CLTS is that it is a community-driven approach. The role of outsiders, possibly including you as a Health Extension Practitioner, is to guide the community to assess its sanitation situation, determine a strategy for improvement, implement the solution and develop a way to measure success.
CLTS relies on the skill of the facilitators using a set of activities and demonstrations to communities to study their situation (Figure 21.4). This includes open defecation patterns in their village and faeco-oral contamination that occurs in their community.

CLTS encourages community members to change by going through an ‘ignition’ moment when they are ‘triggered’ into action, for example, the moment when they collectively realise that open defecation amounts to eating each others’ faeces. In the ‘ignition’ process, the facilitator talks to a gathering of all community members (including men, women, children, youth and elderly) in direct language about sanitation in a way that is normally taboo in the community. By engaging them in frank and transparent discussions, for example asking them to assess the amount of faeces they produce, you will ‘trigger’ them by creating a sense of shame and disgust, which in turn mobilises the community to take immediate action to end open defecation. The facilitator will guide (not prescribe!) the participants in developing their own low-cost latrine designs and a sanitation plan of action for their villages. Hopefully, with the help of locally available expertise and resources, the participants can immediately start constructing latrines.
As part of the CLTS process, activists and enthusiastic members of the community called ‘natural leaders’ should emerge and take the lead. Natural leaders will play a vital role in encouraging communities to adopt and go through with the planned activities. These natural leaders could subsequently become ‘consultants’, triggering and providing engagement and support to communities other than their own.
School-Led Total Sanitation (SLTS) is a related form of community approach to total sanitation. You can engage school teachers and students in similar sanitation activities with the aim to clean up the school environment and promote hygiene among school children and staff. School sanitation clubs can be actively engaged in SLTS. Though the targets are slightly different, the techniques are similar to the CLTS approach.
In CLTS, it is very important for you to consider and understand the cultural and contextual differences between communities. There might be incidences when the community members may be angry or sensitive to discussions at times of triggering and when they are ignited. You must know how to handle these events in order to get back on track. So instead of adopting the whole practice of CLTS applied elsewhere, you may need to adapt it to fit your community’s cultural and social conditions.
Box 21.4 Case Study: CLTS in Fura kebele
Fura kebele declared Open Defecation Free (ODF) status in September 2, 2007.
Fura is in Shebedino Woreda in the Southern Nations Nationalities People’s Region of Ethiopia. Like other areas of Ethiopia, Shebedino suffered with open defecation in the fields, around the home, on footpaths and in the bush. Plan Ethiopia Shebedino Programme, an NGO, technically facilitated the implementation of CLTS in this kebele in February 2007. Local leaders and the Health Extension Workers and health promoters were first trained in CLTS approaches and then community members were involved. With CLTS training, the participants were overwhelmed with shame and disgust because of their open defecation practices. They promised to end open defecation and they achieved this within four months. CLTS mobilised community residents to identify their problems and design their own solutions to improve hygiene and sanitation behaviour. CLTS also facilitated development of local rules, such as ‘any person caught defecating in the open, will be forced to shovel and carry his faeces to the nearest latrine’. All households, 1265 of them, had latrines and 7 communal latrines were constructed along the main road to the market place to be used by passers-by. About one third of household latrines were constructed after CLTS was introduced.
The progress towards total sanitation and the year when 100% coverage was achieved is shown on a chart on the wall of Fura Health Post (Figure 21.5).
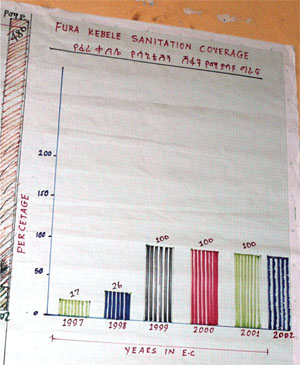 | Figure 21.5 Wallchart at Fura Health Post showing the rapid increase in sanitation coverage in the kebele. 100% coverage was achieved in 1999 in the Ethiopian calendar, 2007 in the European calendar. (Photo: Pam Furniss) |
Open Defecation Free was declared and celebrated on September 2, 2007. Project personnel, local leaders and the kebele residents, in total about 500 people, participated in the celebration which was organised in the compound of Fura School. Poems, drama, songs and posters that condemn open defecation were presented. One of the dramas (Figure 21.6) focused on the need to punish anyone who defecates in the open air.
 | Figure 21.6 Community members demonstrating in drama how they punish open defecators. |
Slogans and sign boards that strongly promote the importance of hygiene and sanitation adorned the school compound. One slogan read: ‘Fura: the kebele where all households constructed pit latrines on their own initiative, and where all use latrine, saying no to open defecation’. Other slogans read: ‘Bury faeces not people’; ‘Fura enters the New Ethiopian Millennium open defecation free’. Community members were very happy about the recognition they had for being Open Defecation Free. They were highly committed and promised to keep their kebele ODF in the future. Neighbouring kebele leaders and Health Extension Workers were invited to share the experience of the Fura ODF event. This resulted in the establishment of school clubs, advocating CLTS in churches and mosques, and establishment of CLTS Committees in other communities.
21.5 Latrine utilisation monitoring and evaluation
Any programme that is promoting behaviour change needs to have a process for assessing how effective it is – in other words, a monitoring and evaluation process. Latrine utilisation promotion and other WASH projects therefore need to include monitoring and evaluation activities. This means setting specific, measurable and achievable objectives, and clearly stating the monitoring activities and indicators to be used.
There is an important preliminary step which is to gather baseline data of the situation before the intervention for comparison with the data gathered by the monitoring activities. The same indicators should be used both before and after so you can compare like with like. Important measurable indicators for latrine use and handwashing include:
- no visible human excreta in likely sites
- percentage of households that have a latrine and which is seen to be in use
- percentage of latrines with no faeces and urine soiling on walls and floors
- presence of handwashing facility and water near the latrine
- presence of soap, ash or other cleaning agent near latrine
- percentage of communities/villages certified as ODF
- percentage of households that have upgraded their latrine to an improved system
- percentage of households with clean compounds without any excreta.
A sample checklist for these indicators is shown in Box 21.5.
Box 21.5 Sample checklist for latrine utilisation
| Name of kebele | |
|---|---|
| Name of village | |
| Questions to asked | Response (yes/no) |
| Is there a latrine? | |
| Is the latrine functioning? | |
| Is there faeces and urine around the latrine? | |
| Is there faeces and urine around the house? | |
| Is there a handwashing facility near the latrine? | |
| Do the family members wash their hands after latrine use? (observe) | |
| Is there water available for handwashing at the time of your visit? | |
| Is there soap or ash in the handwashing facility for handwashing? | |
| Do you observe fresh faeces inside the latrine? | |
| Is the footpath to the latrine free from any barrier? | |
| Name of data collector | |
| Date | |
| Signature | |
Summary of Study Session 21
In Study Session 21, you have learned that:
- Proper community hygiene and sanitation programmes have useful health and socio-economic benefits.
- Identifying the possible reasons for not using latrines and handwashing facilities properly is important in order to promote and sustain positive hygiene behaviours.
- Latrine utilisation and handwashing practices are affected by behavioural, cultural, social, custom, demographic and economic factors.
- Motivating individuals, families and community members using various stimulating techniques will help to bring and sustain hygiene behavioural changes.
- There are different behaviour change models and practical approaches that are applicable for hygiene and sanitation practice.
- CLTS and PHAST approaches are community-driven, facilitator-guided methods for promoting total sanitation and good hygiene practices.
- Monitoring and evaluating the performance of changed behaviour is always important in order to sustain established healthy behaviours.
Self-Assessment Questions (SAQs) for Study Session 21
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 21.1 (tests Learning Outcome SAQ 21.1)
Rewrite the paragraph below using terms from the list provided to fill the gaps.
The terms to use are: PHAST; behaviour change; CLTS; CATS; total sanitation; ODF status.
Improving latrine utilisation requires ________ by the people in the community. Some people may need to be persuaded that ________ and _______ are valuable aims that will help prevent the spread of disease. There are various approaches that can be used to try to achieve _________. Two examples of these approaches are _______ and _________. Both these methods depend on involving the whole community in the process and they are grouped together as _______.
Answer
Improving latrine utilisation requires behaviour change by the people in the community. Some people may need to be persuaded that total sanitation and ODF status are valuable aims that will help prevent the spread of disease. There are various approaches that can be used to try to achieve behaviour change. Two examples of these approaches are PHAST and CLTS. Both these methods depend on involving the whole community in the process and they are grouped together as CATS.
SAQ 21.2 (tests Learning Outcomes 21.2 and 21.3)
Imagine a small village of about 20 households where open defecation is the normal practice. You have visited the village and, from discussions with the people there, you know that most of them are ignorant of the importance of sanitation. They say to you that they have always lived in this way and so did their parents and grandparents before them. They are reluctant to change their habits. What methods would you consider to motivate change in their behaviour?
Answer
The people in this village are not aware of the importance of sanitation so you would need to find ways to educate them about the connection between hygiene and sanitation, and their health. You could ask to speak to a community meeting but this approach may not be successful if you simply stand and talk to the villagers. You could suggest a coffee ceremony or other social gathering as a means to initiate discussion about the issue and to encourage people to attend. You could consider individual house-to-house visits to have more private conversations with individuals and families about hygiene and sanitation. Individual visits may help you identify potential model households that you could also use in your campaign. With the cooperation of the community, and if you had had the appropriate training or could call on the support of others who had, you may also consider using a CLTS approach. You may have to adopt several of these approaches and be flexible according to the responses you get from the community. You should also recognise that it may take time to convince the people of the benefit of change.
SAQ 21.3 (tests Learning Outcome 21.4)
In the same village as SAQ 21.2, imagine there was one family that had their own latrine. You think they might be willing to be a model household to demonstrate good hygiene and sanitation to the others. What would you say to them to encourage them to volunteer as a model household?
Answer
To encourage the family to become a model household you will need to explain to them the purpose and benefits of the role. You should discuss the importance of correct latrine construction and use, and the importance of handwashing with them to check they have a complete understanding. You should check the condition of their latrine and that they have handwashing facilities and use them routinely. You could explain that being a model household will bring respect and admiration from others and they can be proud of their position and achievements. You should also explain that their attitude to others needs to be supportive and encouraging, not bossy and dictatorial.
SAQ 21.4 (tests Learning Outcome 21.5)
Identify one similarity and one difference between PHAST and CLTS approaches.
Answer
PHAST and CLTS are both community-based approaches to achieving total sanitation. They aim to promote behaviour change in the community.
PHAST uses techniques such as mapping and community discussions to promote change. CLTS uses similar techniques but also depends on confronting the community members with questions that make them realise the impact of open defecation. By bringing these questions out into the open, the community is ‘triggered’ into action to change their behaviour.
SAQ 21.5 (tests Learning Outcome 21.6)
Assume you have successfully implemented a CLTS programme. How do you really know if you have been successful?
Answer
To assess the success of the programme you would need to survey latrine use in the community. You would also need to have done a baseline survey before the CLTS programme so that you had the data of latrine utilisation beforehand to compare with. The data you would need to collect would include the number of households with a latrine and handwashing facility, how many of them use their latrine, and whether there were any signs of open defecation anywhere in the area such as faeces visible in fields, paths, compounds, etc.