Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Thursday, 9 July 2026, 1:10 AM
Non-Communicable Diseases, Emergency Care and Mental Health Module: 5. Cataracts, Eye and Ear Injuries
Study Session 5 Cataracts, Eye and Ear Injuries
Introduction
The eye and ear are special organs of the human body that are designed to detect information about the world around us. Any impairment of function in these two organs is experienced as a big problem, particularly by people in rural communities. But this does not always mean that people with eye or ear problems are totally disabled and cannot contribute anything to help themselves or the community at large. Difficulties in seeing or hearing can seriously interfere with normal daily life, but you can help by organising some form of rehabilitation for affected people and their families. (Study Session 16 of this Module is on community-based rehabilitation).
In this study session you will learn about the basic anatomy of the eye, how the eye functions, what cataract means, and the common manifestations of cataract. You will also be learning how to deal with common types of eye and ear injuries, and how to provide emergency care for these problems.
Learning Outcomes for Study Session 5
When you have studied this session, you should be able to:
5.1 Define and use correctly all of the key words printed in bold. (SAQ 5.1)
5.2 Describe the main structures of the eye and their functions. (SAQ 5.1)
5.3 Describe the clinical manifestation of cataract. (SAQ 5.2)
5.4 Explain how cataracts can be treated, using language that an affected person in your community can understand. (SAQ 5.2)
5.5 Describe the main types of eye injuries and what first aid you would give in each case. (SAQ 5.3)
5.6 Describe how you would educate people in your community on the prevention of blindness. (SAQ 5.2)
5.7 Describe the effects of a foreign body in the ear and how to remove it. (SAQ 5.4)
5.1 Anatomy and function of the eye
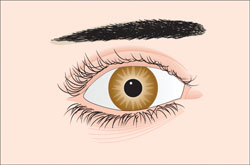
You first need to study the structures of the human eye and their functions. Knowing this will help you understand about the different causes of blindness, such as cataract. As you read the following descriptions, see if you can identify the structures in Figure 5.1, which intentionally has no labels.
The eyeball is a small organ in size, only about 2.5 cm in diameter, but it serves a very important function, which is your sight. Vision is the primary means that you use to gather information from your surroundings. The eye is usually compared to a camera. Each eye gathers light and transforms it into signals to your brain, which interprets what you see as a picture or image. Both the eye and the camera have lenses to focus the incoming light so that the image formed will be clear and understandable.
5.1.1 Eyelids and eyelashes
The eyelids are muscular folds of skin above and below your eyes that can open and close like a gate covering and revealing the eye. They protect the eye from foreign matter, such as dust, dirt and other debris that might damage the eyes. When you blink, the eyelids also help spread tears over the surface of the eye, keeping it moist and comfortable. Eyelashes are small hairs growing from the edges of the eyelids. They filter out dust and debris from the air close to the eye, preventing it from getting into the eyeball.
5.1.2 Sclera and conjunctiva
The sclera is a tough, leather-like, white tissue that extends all around the eye. Similar to an eggshell surrounding an egg and giving its shape, the sclera surrounds the eye and gives the eye its shape. The sclera is also attached to small muscles around the eye, which, in turn, move the eye left and right, up and down, and diagonally. When you look at yourself in the mirror the white part of your eye that you see is the front part of the sclera. Outside the sclera is a very thin transparent membrane, called the conjunctiva.
5.1.3 Cornea, iris and pupil
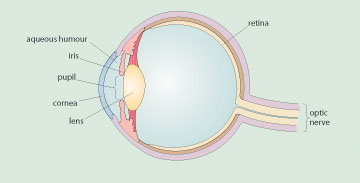
The cornea is a clear layer at the front of the eye which is continuous with the sclera, as you can see in Figure 5.2. You can also see that the cornea is located in front of the iris. The main purpose of the cornea is to help focus light as it enters the eye. The iris is the coloured part of your eye and is made of muscle. The iris controls the amount of light that enters the eye through the pupil. The central opening in the ring-shaped muscular tissue of the iris is called the pupil, and the amount of light that enters the eye, can be altered by the iris changing its shape.
5.1.4 Lens and aqueous humour
The lens of the eye is a clear flexible structure that is located just behind the iris and the pupil. The lens focuses the light as it passes through the eye onto the retina at the back of the eye. The aqueous humour (it means ‘watery matter’) is the fluid found just behind the cornea; its function is to nourish the lens.
5.1.5 Retina
The retina is a complex layer of tissue at the back of the eye, where the image from the light entering the eye is focused. When light hits the retina, it send signals to the brain along the optic nerve. The brain interprets these signals and turns them into information about what the eye is seeing. Damage to any of the structures of the eye due to physical injury or infection, or their gradual wearing out due to age, reduces the quality of vision.
Now try this exercise to test your knowledge of the structures of the eye.
Look at Figure 5.3. Can you add the correct names to the structures labelled (a) to (e)?
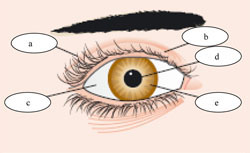 Figure 5.3 Can you name these structures?
Figure 5.3 Can you name these structures?Figure 5.3: The labels you should have added are (a) eyelashes; (b) eyelid; (c) sclera; (d) pupil; (e) iris.
Next we turn to a major cause of blindness all over the world that results from problems in one of the structures you just learned about.
5.2 Cataracts
Cataracts are changes in clarity (clouding) of the lens in the eye, which interferes with the passage of light into the eye. As the lens gets increasingly cloudy (opaque), less and less light can get through it.
What effect will this have on the signals reaching the brain about what the eye is seeing?
If less light can reach the retina at the back of the eye through the cloudy lens, then the signals reaching the brain will be weaker and less focused. The cataract will gradually impair the quality of the person’s vision and result finally in blindness, when light can no longer get through the lens.
In 2002 (European calendar) the World Health Organization estimated that there were 37 million people in the world who were totally blind (unable to see with both eyes), and 161 million people with some sort of visual impairment affecting their sight. Cataracts are the most common cause of blindness worldwide, contributing to 48% of the 37 million people who cannot see at all. Ethiopia is making strong efforts to tackle sight problems in our population (Figure 5.4).
5.2.1 Recognition of cataracts
You should suspect cataracts are the problem when a person comes to you with complaints of visual changes, such as blurred vision, difficulty in seeing in bright light, inability to see distant objects or scenes, poor colour vision, and difficulty in reading. As cataracts continue to progress and the lens become more opaque, the person will say they feel like they are looking through cloudy glass. The area of the pupil appears white or cloudy when the cataract is found at a late stage.
Cataracts are usually progressive and painless, and not associated with any redness of the eye. When you look at a person with advanced cataract you can see the clouding or milky appearance of the lens, which is particularly obvious if you shine a light into the eye (Figure 5.5).

Cataracts can sometimes develop in children, but usually the person is above the age of 40 years. If someone complains of these problems, you should suspect cataract and refer this person to the nearest hospital or health centre. The diagnosis that cataract is the cause of the visual problems will be confirmed by examination with a special instrument called a slit-lamp microscope (or simply ‘eye microscope’) to look into the eye.
You should tell the person with suspected cataracts that after the examination at the hospital or health centre, the doctor will discuss if a solution is possible for their sight problems. A simple surgical treatment could transform their vision from not seeing well to being able to see much better again. We will tell you about treatments for cataract later in this study session.
5.2.2 Classification and causes of cataract
Cataracts may be classified based on several factors, including the age of the person when the cataract was first detected, the cause of the cataract and whether it is an inborn (genetic) or acquired problem. Some of the causes include physical injury to the eye, long-term exposure to very bright sunlight, or to the fumes and smoke from household cooking fires, cigarette smoking, poor control of diabetes mellitus (the high sugar levels in the blood damages the eye), and so on. All of these factors reduce the clarity of the lens over time. The susceptibility to develop cataracts can also be transmitted in the genes from parent to child.
You should also know that deficiency of vitamin A from the food we eat is an important cause of blindness. To prevent blindness from vitamin A deficiency, infants are given a supplement of vitamin A drops with measles vaccine, repeated every six months until the age of five years.
Refer to the Immunization Module, Study Session 3 and the Communicable Diseases Module, Study Session 4 for the doses of Vitamin A drops. More details of blindness due to nutritional deficiency are given in the Nutrition Module, Study Session 5.
5.2.3 Prevention of cataracts
The purpose of classifying cataracts is to help you understand the different causes, so that you can educate your community about those causes which are preventable.
What specific causes of cataract can you prevent or delay from causing visual impairment?
Did you say poorly controlled diabetes mellitus, eye injury, or direct exposure to sunlight, smoke and fumes? You are right!
How would you advise people to reduce their risk of developing cataracts?
By getting treatment if they are diabetic, because effective blood-sugar control delays the progression of cataracts; by shading their eyes with dark glasses to protect them from the harmful rays from the sun; and by not smoking cigarettes, and ventilating their room if smoke from a cooking fire is collecting in the house.
Though there is no really effective way of preventing cataracts at present, interventions such as these can significantly alter the disease burden of cataracts by minimising exposure to factors that promote them to develop. A healthy lifestyle might also help, just as it helps prevent other non-communicable diseases: eat a balanced diet, get regular exercise and rest, and do not smoke or drink much alcohol.
5.2.4 Treatment of cataracts
The most important step in the treatment of cataracts is early detection of the problem. Once it is detected at the early stage, the initial treatment is to slow down the clouding of the lens by following the preventive measures described in the previous section. For late-stage cataract with blindness, the best intervention is surgical treatment to remove the cloudy lens (Figure 5.6).

Taking out the lens improves the person’s sight because light can get all the way to the back of the eye again. However, without a lens to focus the light, the restored vision is more blurred than before the cataracts developed. Cataract surgery may be available that includes replacing the cloudy lens with an artificial one, which restores good sight.
So, besides advocating and practicing the preventive measures, you have to facilitate transfer of people affected by cataracts to a hospital or health centre with an eye-care unit. You should tell the person you refer about the big transformation of life after the treatment of cataract blindness (Case Study 5.1), so that the person will decide on travelling for treatment. At times cataract operation campaigns may come to your village and you should take part in actively mobilising affected people in the community to come for treatment.
Case Study 5.1 Mr K had never seen his grandson
Mr K is 71 years old and has worked as a farmer all his life. His daughter recently gave birth to his first grandson, but he was very depressed when he realised that he cannot see the baby because he is blind from cataracts in both eyes. As a Health Extension Practitioner, you recognised several years ago that Mr K’s sight problems were due to his cataracts, but he would not take your strong advice to go to the health centre for assessment and possible treatment. When you went to his house for a visit after his grandson was born, you again encouraged him to travel for cataract surgery. This time he decided to go for treatment. The surgery was very quick and it did not cause him pain. The outcome was successful and when he came back to the village he prepared a big feast to celebrate his ability to see his new grandson.
Does this story help you in referring other people for cataract treatment? We hope that it does, as you know it is a great blessing for anyone to reach the age of having grandchildren and great-grandchildren. But being unable to see them is sad. When this disability is corrected by cataract surgery it is like being reborn. So, such a success story is useful in encouraging people to go for cataract treatment.
5.3 Eye injuries
Eye injuries are very common in most communities, especially in children and people younger than 30 years. Injury to the eye is one of the causes of cataracts. Eye injuries are the leading cause of blindness in only one eye worldwide. When you study the types of injuries described below, you will understand why young people are more likely than older people to suffer a blinding injury to one eye.
5.3.1 Causes and types of eye injuries
There are several common causes of eye injury, which have different outcomes depending on the extent of the injury and degree of disability that follows. Some of the common causes are listed below.
Chemical injury (splash)
A splash in the eye by anything other than clean water can be dangerous. Some substances sting when they get into the eye accidentally (e.g. lemon juice, salty water), but are harmless. Others can cause serious damage (e.g. cleaning fluids, agricultural chemicals). Acids cause more damage to the delicate structures of the eye than most other chemicals.
Scratch by a foreign body
Any foreign body (e.g. a speck of dust or some dirt) that gets into contact with the eye accidentally causes a scratch to the cornea or sclera. This can be painful at the time it happens, and cause the eye to ‘water’ as a way of flushing the dirt out of the eye. If the scratch is not deep it will usually soon heal. However, a deep scratch can cause impaired vision if it leaves a scar on the cornea.
Penetration by sharp objects
Penetration of the cornea (or rarely the sclera) can happen due to sharp objects accidentally entering the eye and penetrating the eyeball. This causes intense pain, redness and excessive weeping of tears from the eye and can lead to permanent sight problems. The objects causing the injury can be fragments of wood, metal or stones, and such accidents often happen at work (Figure 5.7).

Blunt (non-penetrating) injury
The eye can get injured by a blow, for example in a fight or a fall, without any penetration in the eye structure externally. The surface of the eye looks very red, due to bleeding from tiny blood capillaries in the sclera. The eye may swell and vision may be affected, but usually the swelling will go down and the blood will be absorbed into the body over several days or weeks.
Injury to the eyelids
You may come across someone who has got a cut to the eyelids following a blow or sharp injury. There may also be swelling without a cut over the eyelids..
Now it is time to tell you about first aid supportive care for such a problem, and all the other eye injuries described above
5.3.2 Supportive care in the case of eye injury
If you are treating someone with a chemical splash injury, or dust in the eyes, simply rinse the eye with plenty of clean water. Foreign bodies which are not attached to the eye, or do not cause penetration to the eyeball, can simply be removed with the edge of a clean piece of cloth. Getting the chemicals, dirt or other foreign body out of the eye quickly protects it from further damage. If the foreign body is difficult to remove because it is attached to the eye, or if there is penetration or injury to the eyeball (Figure 5.8), cover the eye with clean cloth and transfer the person to the health centre or hospital.

If you happen to see a person with injury to the eyelids, or swelling, you should stop the bleeding and help reduce the swelling by applying gentle pressure to the eye using a pad of clean cloth. Refer the person to the health centre or hospital.
5.4 Trachoma
Trachoma is described in detail in the Communicable Diseases Module, Part 4, Study Session 39.
We will briefly mention a very common cause of blindness in Ethiopia – bacterial infection with Chlamydia trachomatis leading to a condition called trachoma. The infection causes inflammation of the conjunctiva, the thin transparent membrane covering the eyeball and the inner surface of the eyelids. The upper eyelid is particularly affected and over time it becomes so swollen and scarred that the eyelashes turn inwards and scratch across the surface of the cornea every time the person blinks. The cornea is damaged by the scratching eyelashes and it gradually becomes opaque (unable to transmit light).
Corneal opacity is a major cause of sight loss. Over 80 million people suffer from trachoma worldwide, and in Ethiopia there are estimated to be more than 238,000 people who are blind because of it (Figure 5.9).

Mild trachoma is easily treated with tetracycline eye ointment (1%). Trachoma scarring can be reduced or prevented by simple eye surgery to turn the eyelashes outwards so they don’t scratch the eye. Prevention of trachoma is through avoiding the infections from getting into the eyes. The bacteria are transmitted mainly by flies landing on the face and carrying the infected discharge from the eyes to another person, or the bacteria are transferred on dirty hands or cloths used to wipe the sore eyes. Regular washing of faces and hands, disposing of rubbish and other waste to keep flies away from houses, and penning animals away from homes at night, are all ways to reduce the risk of trachoma.
Next you will be studying about foreign bodies in the ear, which is a common problem in children.
5.5 Ear injuries due to foreign objects
As you learned in the Communicable Diseases Module (Study Session 35), children are prone to develop infections of the inner ear, which may have spread from the respiratory tract up the Eustachian tubes into the ears (Figure 5.10).
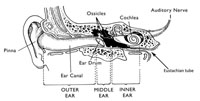
Another very common ear problem in children is caused when they put foreign objects into the ear canal (on the left of Figure 5.10) when they are playing. They often put small objects such as beans, peas, rice, beads, fruit seeds or small stones into their ears. If these foreign bodies remain in the ear for a long time, they make it more likely that the child will develop an ear infection. This in turn may lead to a loss of hearing, if untreated. You should suspect the possibility of something foreign in a child’s ear if the child complains of pain in the affected ear, a bad smell or discharge comes from the ear (Figure 5.11), or the parents or school teacher tell you that the child doesn’t seem to hear them talking if they speak into that ear.

Simple removal of a foreign object from the ear helps to reduce the risk of deafness resulting from chronic (long-term) infection. Shine a torch into the child’s ear and if the foreign object is visible, try to remove it by using a thin blunt instrument (Figure 5.12) – the end must not be sharp! If the ear drum is broken or scarred by infection, the child could suffer some permanent hearing loss in that ear. If you don’t see a foreign object when you look into the ear with a torch, transfer the child to the nearest health facility for specialist help. If there is any discharge from the ear, the child will need medical treatment with antibiotics.
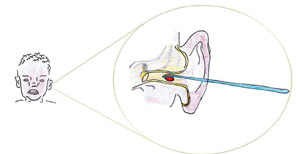
![]() Be careful not to push the instrument too far into the ear, or you may puncture the delicate ear drum!
Be careful not to push the instrument too far into the ear, or you may puncture the delicate ear drum!
In the next study session you will study another important but often neglected topic for your health promotion and disease prevention practice – oral health and the prevention of dental problems.
Summary of Study Session 5
In this study session, you have learned that:
- The eye serves an important purpose of vision and its function is comparable to the function of a camera in taking a photo.
- The main structures of the eyeball are the sclera, cornea, pupil, iris and lens, all of which have the important function of transmitting light onto the retina at the back of the eye where the image is formed.
- Cataracts and eye injuries are important causes of blindness worldwide, where cataract alone contributes to 48% of all people who are totally blind.
- The early symptoms of cataract are blurred vision, difficulty seeing in bright light and poor colour vision.
- Cataract progression can be slowed by preventing eye injury, strict control of blood sugar, and avoiding exposure to smoke from cigarettes and indoor fires. Lack of vitamin A in the diet and measles infection are other causes of blindness.
- Common causes of eye injury are scratches, chemical splashes, penetrating and blunt injuries, and cuts to the eyelids.
- Damage to the cornea by the eyelashes turning inwards and scratching it is an important cause of blindness. It is due to a chronic eye infection called trachoma.
- Children often insert small foreign objects into their ears, which can lead to problems of ear infection and deafness. Some of the common objects they play with are beans, peas, beads and fruit seeds.
- Careful removal of foreign objects from the ears prevents ear infection, which is an important cause of deafness, especially in children.
Self-Assessment Questions (SAQs) for Study Session 5
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 5.1 (tests Learning Outcomes 5.1 and 5.2)
Which structures of the eye are serving the purpose of defending the eye, and which ones are for transmission of light into the eye?
Answer
The eyelids and eyelashes protect the eye from foreign materials getting into it. The sclera, cornea, pupil, iris and the lens serve the purpose of light transmission onto the retina at the back of the eye.
Read Case Study 5.2 and respond to the questions that follow.
Case Study 5.2 Mr Worku can’t see well
Mr Worku, a 75-year-old man from your village, complains of having blurred vision and difficulty seeing in the bright sunlight whenever he goes to the market. He very frequently holds his hands above his eyes to shade them from the sun, and he finds it difficult to see who is approaching him when he meets people in the village.
SAQ 5.2 (tests Learning Outcomes 5.3, 5.4 and 5.6)
- a.What is the most likely cause of the visual problems this man is having? What signs in the case study suggested your diagnosis?
- b.What advice will you give to Mr Worku about how his condition can be delayed from getting worse? What do you tell him about possible treatment in the future?
Answer
- a.Mr Worku is an elderly man who is having problems seeing in bright sunlight; his vision is blurred and he has increasing difficulty in seeing the world around him clearly. These are typical early symptoms of cataract
- b.You should advise him to do everything he can to delay the cataracts from getting worse, such as wearing dark eye glasses to protect his eyes from sunlight, avoiding exposure to smoke, eating a balanced diet, and effective blood-sugar control if the man has got diabetes. Explain to him that if his cataracts progress to the stage where his sight has almost gone, he can get surgical treatment to remove the cloudy lenses and restore his sight – at least to some extent. Tell him that the operation is quick, simple and painless.
SAQ 5.3 (tests Learning Outcome 5.5)
Why do you think that children and young adults are more likely than older people to suffer an injury to one eye that results in long-term damage?
Answer
Injuries to one eye usually result from chemical splashes, accidental scratches, penetration by sharp objects, or non-penetrating blows. This type of injury is most likely to happen during jobs such as welding or stone work, or during fights or play with sharp objects such as sticks or stones. These types of activities are more likely to involve children and young adults than older people.
Read Case Study 5.3 and respond to the questions that follow.
Case Study 5.3 A child has a bad-smelling ear discharge
A three-year-old child was brought to you with earache, pulling her external ear now and then, and you can see a whitish-yellow ear discharge. The parents also report that the child is not hearing well when they speak to her in a normal voice. They say they have to speak very loud so that the child hears what they say.
SAQ 5.4 (tests Learning Outcome 5.7)
- a.What possible problem would you look for in this child?
- b.How would you treat her condition?
Answer
- a.The symptoms described by this child’s parents should make you suspect the child has a foreign body in her ear. At three years old she is too young to be able to tell you if she has put something into her ear.
- b.Shine a torch into her ear to look for the possibility of a foreign body in there. If you can see the object, try very carefully to remove it with a thin blunt tool. Then refer the child to a health facility. The whitish-yellowish discharge from her ear tells you that it is infected and she needs medical treatment with antibiotics.