

6.4 Using economic evidence to prioritise interventions
Now that you have seen how incremental cost-effectiveness ratios can be used to compare interventions, try Activity 8 to put what you have learned into practice.
Activity 8: Calculating incremental cost-effectiveness ratios
Table 7 includes information about four healthcare strategies for a hospital to reduce the incidence of hospital-acquired infections. The strategies include current practice and three new strategies (a hand hygiene programme and two screening programs, A and B).
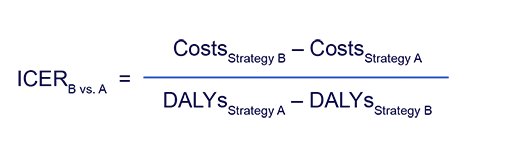
Using the information in Table 7, try to complete the second column in Table 8 by calculating the incremental cost-effectiveness ratios (ICERs) using the equation below. (You should round your answers to the nearest dollar.)
Note that the order of the ICER formula is different in the numerator and denominator when DALYs are used, as greater DALYs indicates worse health outcomes. Therefore, the formula is adjusted to provide cost per DALY reduction. The ICER for cost per DALY averted can be calculated using the following equation:
Having calculated the ICER for each of the pairs of strategies in Table 7, compare the ICERs to the cost-effectiveness threshold to understand whether the strategies are effective compared to the comparator. You need to remember the cost-effectiveness plane here. Record your decisions in the final column of Table 7.
The cost-effectiveness threshold is $9300/DALY averted.
| Interventions | Total cost ($) | Total DALYs |
|---|---|---|
| Current practice | 0 | 15 |
| Hand hygiene programme | 10,000 | 13 |
| Screening programme A | 50,000 | 10 |
| Screening programme B | 60,000 | 7.5 |
| Cost-effectiveness | ICER ($/DALY averted) | Cost-effective? (Yes/No) |
|---|---|---|
| Hand hygiene programme versus current practice | ||
| Screening programme A. versus current practice | ||
| Screening programme B versus current practice | ||
| Screening programme B versus hand hygiene programme |
Discussion
Table 9 shows the correctly completed table.
| Cost-effectiveness | ICER ($/DALY averted) | Cost-effective? (Yes/No) |
|---|---|---|
| Hand hygiene programme versus current practice | 5000 | Yes |
| Screening programme A. versus current practice | 10,000 | No |
| Screening programme B versus current practice | 8000 | Yes |
| Screening programme B versus hand hygiene programme | 9091 | Yes |
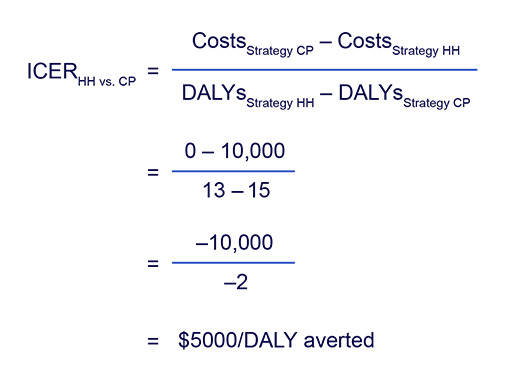
Here’s an example ICER calculation for hand hygiene programme (HH) versus current practice (CP):
Screening programme A was found not to be cost-effective compared to current practice and thus was not compared to the two cost-effective interventions (the hand hygiene programme and screening programme B).
Use your completed Table 6 to answer the following questions:
- Solely using the cost-effectiveness evidence, if only one strategy could be implemented, which should it be?
- Hand hygiene programme
- Screening programme A
- Screening programme B
- Imagine that you have now learned that there are concerns that some costs for screening programme B were omitted from the cost-effectiveness analysis. How might this change your answer?
Discussion
There is no correct answer to the first question, but you might have considered that the ICER of screening programme B versus the hand hygiene programme is less than, but very close to, the CET. Therefore, any increase in the costs of screening programme B will bring the ICER closer to the CET or potentially exceed it, meaning that there is a chance that screening programme B would no longer be estimated to be cost-effective compared to the hand hygiene programme.
6.3 Decision-making using the cost-effectiveness plane

