
4.4 Cervical dilatation
As you learned in Study Session 1 of this Module, the first stage of labour is divided into the latent and the active phases. The latent phase at the onset of labour lasts until cervical dilatation is 4 cm and is accompanied by effacement of the cervix (as shown in Figure 1.1 previously). The latent phase may last up to 8 hours, although it is usually completed more quickly than this. Although regular assessments of maternal and fetal wellbeing and a record of all findings should be made, these are not plotted on the partograph until labour enters the active phase.
Vaginal examinations are carried out approximately every 4 hours from this point until the baby is born. The active phase of the first stage of labour starts when the cervix is 4 cm dilated and it is completed at full dilatation, i.e. 10 cm. Progress in cervical dilatation during the active phase is at least 1 cm per hour (often quicker in multigravida mothers).
In the cervical dilatation section of the partograph, down the left side, are the numbers 0–10. Each number/square represents 1 cm dilatation. Along the bottom of this section are 24 squares, each representing 1 hour. The dilatation of the cervix is estimated by vaginal examination and recorded on the partograph with an X mark every 4 hours. Cervical dilatation in multipara women may need to be checked more frequently than every 4 hours in advanced labour, because their progress is likely to be faster than that of women who are giving birth for the first time.
In the example in Figure 4.2, what change in cervical dilatation has been recorded over what time period?
The cervical dilatation was about 5 cm at 1 hour after the monitoring of this labour began; after another four hours, the mother’s cervix was fully dilated at 10 cm.
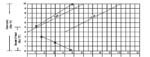
If progress of labour is satisfactory, the recording of cervical dilatation will remain on, or to the left, of the alert line.
If the membranes have ruptured and the woman has no contractions, do not perform a digital vaginal examination, as it does not help to establish the diagnosis and there is a risk of introducing infection. (PROM, premature rupture of membranes, was the subject of Study Session 17 of the Antenatal Care Module.)
4.3 Recording and interpreting the progress of labour