
It began routinely enough. A patient with severe respiratory disease at the Dr. Soliman Fakeeh Hospital in Jeddah, Saudi Arabia was getting worse and no one knew why. A sample of sputum was sent to Dr. Ali Mohamed Zaki to identify the culprit, as he had identified these diseases many times before. However, this time would be different. The sample showed no positive hits on any of the virus assays he normally used. He contacted Dr. Ron Fouchier, at Erasmus Medical College in Rotterdam, Netherlands, to see if he could be of help. Dr. Zaki's initial idea was that the virus was a paramyxovirus, and Dr Fouchier had recently published a Pan-paramyxovirus polymerase chain reaction (PCR) assay. In Dr. Fouchier's lab, the virus was identified as a novel coronavirus, one that had never been seen before.
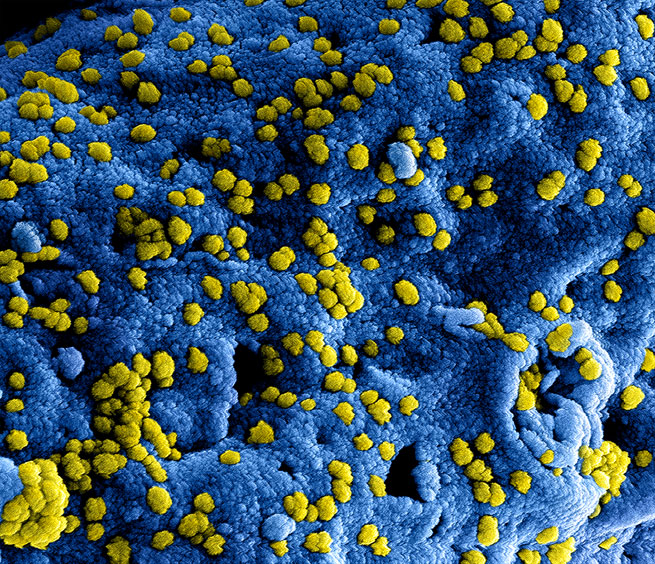 Colorized scanning electron micrograph of Middle Eastern Respiratory Syndrome virus particles attached to the surface of an infected VERO E6 cell.
Colorized scanning electron micrograph of Middle Eastern Respiratory Syndrome virus particles attached to the surface of an infected VERO E6 cell.
This novel coronavirus, now called Middle East respiratory syndrome coronavirus (MERS-CoV), has been identified in several countries across the Middle East and Europe, with primary infections found in Saudi Arabia, Qatar, Jordan, and The United Arab Emirates (UAE). Infections in the United Kingdom, Tunisia, France, Italy, and Germany have been imported by travel from the Middle East. The Italian cluster is believed to be from a patient traveling to Jordan and back, and the French cluster originated from a patient traveling to the UAE. The largest cluster of cases, 23 in total, is in Saudi Arabia. As of July 25, 2013, there were 90 confirmed infections, of which 45 have resulted in death, resulting in a 50% case fatality rate. MERS-CoV has been sequenced from nine infected individuals, and its genome sequence places it in the same sub-family (Group 2) as SARS coronavirus (SARS-CoV), but in a new lineage (called Group 2c).
The initial name of this novel coronavirus was hCoV-EMC, which stood for human coronavirus–Erasmus Medical College, where the first isolate was sequenced. An additional isolate, provisionally named human coronavirus England 1, was isolated from a patient in London, UK, who had been flown from Qatar to London for treatment. A report from the Coronavirus Study Group of the International Committee on Taxonomy of Viruses (ICTV) has proposed naming this virus Middle East respiratory syndrome coronavirus (MERS-CoV). MERS-CoV is provisional until ratified by the ICTV.
The closest phylogenetic neighbors to MERS-CoV are putative bat coronaviruses in China (BtCoV-HKU4 and BtCoV-HKU5), the Netherlands (BtCoV/VM314/2008}, and a recently discovered isolate from South Africa. All four of these bat coronaviruses have been sequenced only from bat samples and have never been isolated as live viruses from either bats or the environment. The natural reservoir of MERS-CoV has not been identified, although its similarity to these other four viruses suggests that it is of bat origin. Importantly, SARS-CoV emerged from bats as well. Anecdotal evidence suggests that MERS-CoV may have been transmitted to humans via livestock (camels or goats); however, there is no scientific data yet to support this theory.
Are there any treatments?
There is no current treatment or vaccination available for MERS-CoV, but, with the continuation of the outbreak, identification of therapeutics is a top priority.
A version of this article was originally published on PLOS Pathogens in 2013. For an up-to-date view of the identification and emerging treatments, visit the WHO FAQ page on MERS.
Formal citation: Coleman CM, Frieman MB (2013) Emergence of the Middle East Respiratory Syndrome Coronavirus. PLoS Pathog 9(9): e1003595. doi:10.1371/journal.ppat.1003595
Rate and Review
Rate this article
Review this article
Log into OpenLearn to leave reviews and join in the conversation.
Article reviews