3.4 An approach to fracture risk assessment in Parkinson’s
In light of the particular fracture risks in Parkinson’s, Lyell et al (2015), suggested an algorithm for assessing and responding to Parkinson’s fracture risk. In 2017 the NOGG thresholds were updated and, accordingly, a revised algorithm was proposed (Henderson et al, 2019). This protocol is shown in the diagram below and is applicable to people with Parkinson’s, who are seen in primary or secondary care settings, and who are not in the very final stages of illness. It proposes a 4-step approach to ascertaining fracture risk that will then serve to inform treatment options.
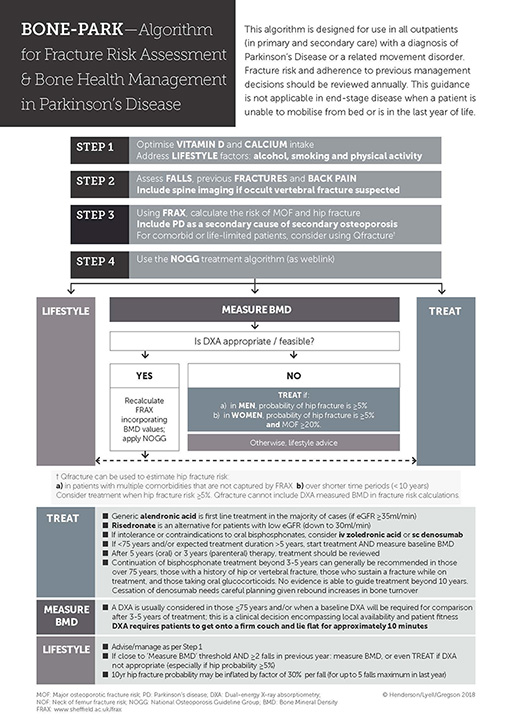
Accessible Powerpoint version of image [Tip: hold Ctrl and click a link to open it in a new tab. (Hide tip)]
Step 1 is to address lifestyle factors such as smoking, alcohol use and physical activity. More detail is provided in Section 4.1. Vitamin D and calcium intake should be optimised and this is described in Section 4.2.
Step 2 is to assess the number of previous falls. Some patients may have vertebral fractures but be unaware of them. If they complain of back pain, or have a flexed posture which is not correctable, consider requesting X-rays of the spine. If a vertebral fracture is identified, this can be incorporated into risk assessment, where it will increase future fracture risk scores.
Step 3 FRAX should be used to calculate fracture risk. There are some particular aspects of using FRAX in PD that should be considered.
FRAX is, broadly speaking, the best tool to use to calculate fracture risk in PD. However, QFracture should be considered in patients with a limited life expectancy as risk can be calculated over a shorter period of time (<10 years). In addition, Qfracture facilitates the inclusion of multiple comorbidities and the number of falls an individual has experienced.
As falls are a major fracture risk and common in Parkinson’s, FRAX probabilities could be inflated in the presence of recorded falls (Masud et al, 2011).
KEY POINT
Each fall, up to a maximum of 5, in the last year, can be used to inflate the calculated probability by 30%.
For example, if the FRAX calculated MOF probability was 15% over 10 years, but the patient had fallen twice in the last year, 30% of this risk (4.5%) would need to be added on for each fall. This would make the total risk 15 + 4.5 + 4.5 = 24%.
The clinician can then interpret the inflated probability against NOGG thresholds. Whilst this may be too cumbersome to use routinely, it underlines the point that FRAX underestimates risk in fallers and it is reasonable to allow for this added risk when making decisions.
Secondly, Parkinson’s is associated with poor bone health with a low BMD. Parkinson’s is currently not included in the list of secondary osteoporosis conditions in FRAX.
However, the wording ‘enter yes if the patient has a disorder strongly associated with osteoporosis’ allows for Parkinson’s to be included by proxy. When using the FRAX tool in Parkinson’s the question 10, ‘secondary osteoporosis’ box should be ticked. New NOGG guidance acknowledges the increased risk in Parkinson’s too.
KEY POINT
Selecting ‘YES’ to the FRAX question 10 ‘Secondary osteoporosis’, allows Parkinson’s to be considered as a condition that is strongly associated with osteoporosis.
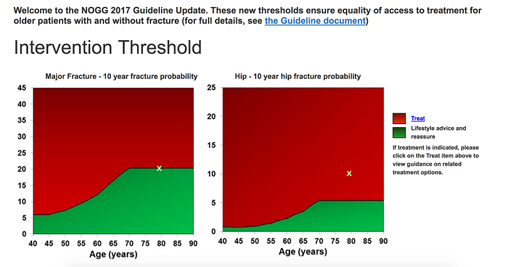
Step 4. Using the NOGG treatment algorithm to guide your management. This graph is found if you click the link after the FRAX results.
This graph relates to MOF risk, rather than hip fracture risk. This can disadvantage those with Parkinson’s in whom hip fracture risk is disproportionately high. The body of the NOGG guidance supports the use of a threshold of 5.4% for hip fracture risk over the age of 70 (there are lower, age specific thresholds for younger patients – see image ‘Hip fracture thresholds NOGG’). It also supports the use of a threshold of 20.3% for MOF risk.
KEY POINT
It is therefore reasonable to treat and/or measure BMD in those with a probability of hip fracture above 5.4%, even if the probability of MOF is not above the intervention threshold on the NOGG guidance graph.
For patients under 70, you should obtain a DXA and recalculate FRAX including the measured BMD. Your patient’s results can be plotted on this graph using the NOGG Manual Data Entry form and entering the MOF and hip fracture probabilities. This will indicate whether your patient should have lifestyle advice only, or be recommended for treatment. There is also a link to straightforward treatment options. In the example image here, you can see that the patient is recommended for treatment based on the hip fracture probability, although the Major Fracture probability is not above the threshold.
If these thresholds are not reached, but MOF probability is over 11%, it is appropriate to obtain BMD measurement and recalculate FRAX. For younger people, these thresholds are lower and increase with age.
3.3 Adapting these tools to Parkinson’s