3.4.1 Activity
Below are four example patients. Use these to generate risk figures using each tool. Not all patients would need a Qfracture score (the algorithm suggests it only for co-morbid or life-limited patients) but it is useful practice to perform it, and think about whether you would do this in practice. Go to the sites (links below) and use the clinical information given to fill in the boxes or answer the questions. If information is missing, as it sometimes is in a clinical setting, then assume a negative answer.
FRAX Fracture risk assessment tool [Tip: hold Ctrl and click a link to open it in a new tab. (Hide tip)]
QFracture 2016 risk calculator
Mr C
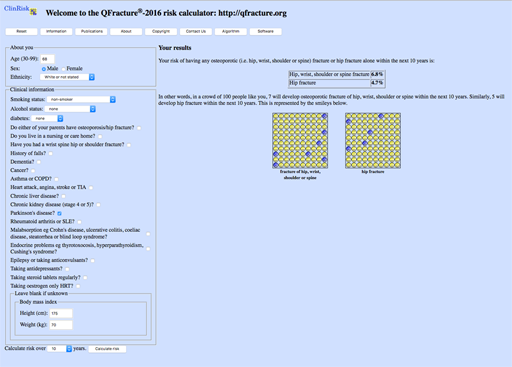
Mr C is 68, independent at home, and has had Parkinson’s for a number of years. He is on herbal treatment for depression and has chronic kidney disease stage 3a and hypertension. He has had no previous falls. He weighs 70kg and he is 1m 75 tall.
Answer
| Result: | FRAX MOF: | 7.6% | HIP: 2.3% |
| Qfracture MOF: | 6.8% | HIP: 4.7% |
You can see that Mr C’s risk is below the ‘rule of thumb’ thresholds mentioned above. Using the algorithm suggested, you can follow that NOGG guidance would be simply to give lifestyle advice (more on this in the next section). Qfracture gives a pictorial illustration of his risk but as he is unlikely to have a life expectancy below 10 years there is no particular reason to use Qfracture. His risk should be reviewed yearly as it will change with age and other factors.
Mr D
Mr D is 84 years old with Parkinson’s and dementia. He is a residential care home resident and has had 4 falls in the last year. His height is 180cm and he weighs 84kg. He has had a previous transient ischaemic attack (TIA).
Answer
| Result: | FRAX MOF: | 12% | HIP: 7.3% |
| Qfracture MOF: | 36.1% | HIP: 34.5% |
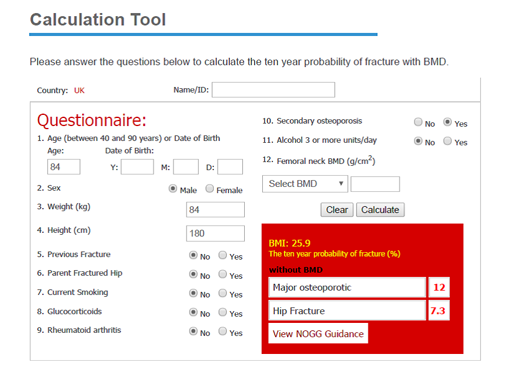
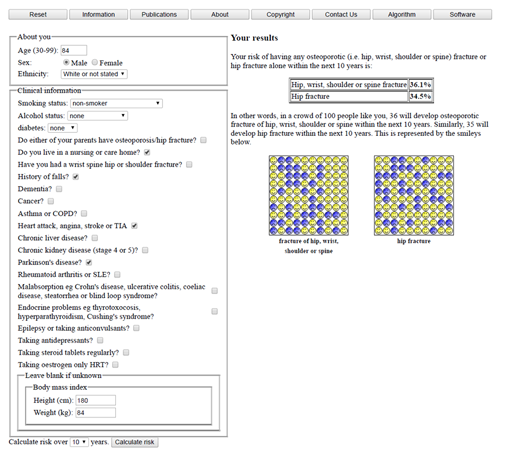
You can see that Mr D’s FRAX MOF risk is below the ‘rule of thumb’ threshold mentioned above, but his hip fracture risk is above 5%. Qfracture gives a very high estimate for his risk (probably an overestimate but clearly raising the question over treatment to reduce fracture risk). Using the algorithm suggested, you can follow that NOGG guidance would be to obtain a DXA. In someone frail and living in a care home, this may not be appropriate or feasible, but the algorithm makes it clear that it would be reasonable to treat according to his hip fracture risk without further investigation.
Mrs E
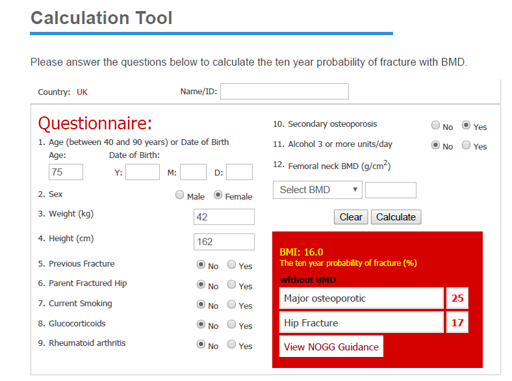
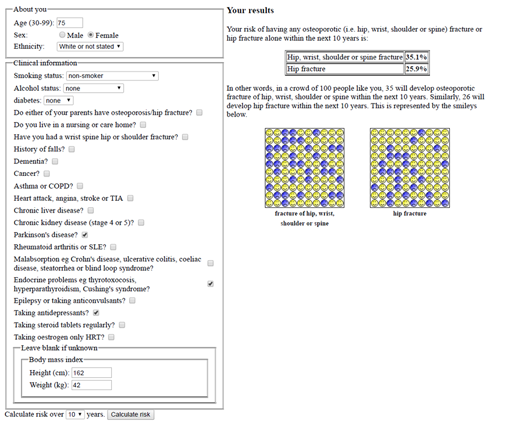
Mrs E, who is 75, has had Parkinson’s since her 60s. She has a history of thyrotoxicosis. She has suffered with depression and takes an SSRI. She weighs 42kg and she is 162cm tall. She has had no falls. She is a non-smoker and drinks no alcohol. She has not had any previous fractures.
Answer
| Result: | FRAX MOF: | 25% | HIP: 17% |
| Qfracture MOF: | 35.1% | HIP: 25.9% |
You can see that Mrs E’s risk is well above the ‘rule of thumb’ thresholds mentioned above. Qfracture gives a pictorial illustration of her risk. Using the algorithm suggested, you can follow that NOGG guidance would be simply to treat, without the need for a DXA. However, presuming she has a life expectancy of more than 5 years, a DXA would be ideal to monitor treatment response and guide decision making after 5 years of treatment. There is no need to await the DXA results before starting treatment.
Mrs F
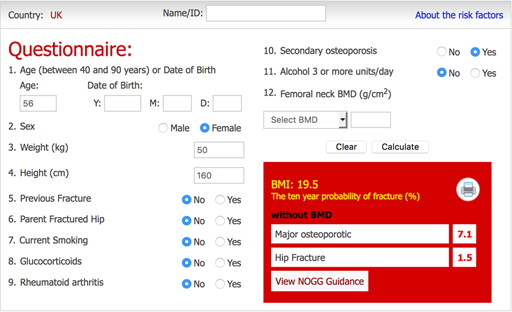
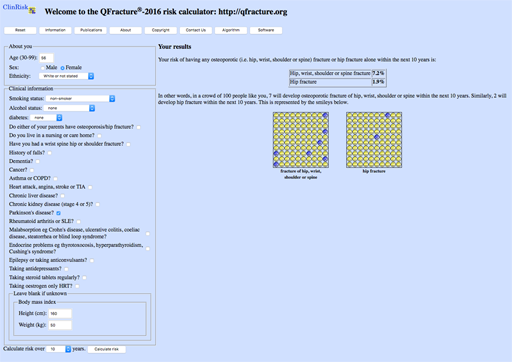
Mrs F is 56, with Parkinson’s but no other health issues. She had an early menopause at 44 but was on HRT until the age of 50. She weighs 50kg and she is 160cm tall.
Answer
| Result: | FRAX MOF: | 7.1% | HIP: 1.5% |
| Qfracture MOF: | 7.2% | HIP: 1.9% |
You can see that Mrs F’s risk is below the ‘rule of thumb’ thresholds mentioned above. Using the algorithm suggested, you can follow that NOGG guidance would be simply to give lifestyle advice (more on this in the next section). Qfracture gives a pictorial illustration of her risk but does not need to be performed unless this is helpful to her. Her risk should be reviewed yearly as it will change with age and other factors.
3.4 An approach to fracture risk assessment in Parkinson’s