4.7 Treatment duration and adherence

A treatment review should be performed after 3 years of zoledronic acid therapy and 5 years of oral bisphosphonate treatment.
Continuation of bisphosphonate treatment beyond 3-5 years can generally be recommended in individuals age >75 years, those with a history of hip or vertebral fracture, those who sustain a fracture while on treatment and those taking oral glucocorticoids (steroids). A repeat BMD measurement can be helpful in reassessing risk. More detailed advice, and the following algorithm, can be found in section 7 of the NOGG full guidance.
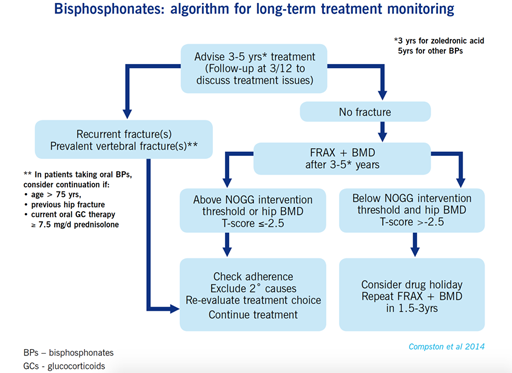
If treatment is discontinued, fracture risk should be reassessed after a new fracture, regardless of when this occurs. If no new fracture occurs, assessment of fracture risk should be performed again after 18 months to 3 years.
The beneficial effects of denosumab wear off very quickly once it is stopped, so specialist advice should be sought when doing this.
People with Parkinson’s can find concordance with their medication schedule challenging. Adding osteoporosis treatment to an often, already, complicated regime, presents a further challenge and burden. Aligning medication timings can help adherence and the use of a combination of pill organisers, reminders and alarms can help concordance with medication schedules [Tip: hold Ctrl and click a link to open it in a new tab. (Hide tip)] (Straka et al 2018). Bisphosphonate compliance is often sub-optimal and it is imperative to review this at follow-up. Non-concordance is often secondary to mild gastrointestinal side effects and intravenous zoledronic acid can be considered in these circumstances.
4.6 Drug treatment for osteoporosis: other treatment options