
Self-Assessment Questions (SAQs) for Study Session 10
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering the following questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 10.1 (tests Learning Outcomes 10.1, 10.2 and 10.5)
In your Health Post, you use infant immunization cards to record immunizations given to each individual infant, and an EPI Registration Book to record the immunizations you have given.
- What other basic EPI recording tool should you be using and what two things does it enable you to do?
Answer
Tally sheets should also be used to record the number of doses and the lot number of each vaccine given during each immunization session. This enables you to check that the number of doses given tallies (matches) the number recorded in your Registration Book. It also acts as a way of monitoring the number of doses given, and enables you to complete your monthly Summary Report to the higher level. You may also have mentioned your Vaccine Stock Register (see Study Session 5).
SAQ 10.2 (tests Learning Outcomes 10.1 and 10.3)
The percentage of children in the target population who receive the first dose of pentavalent vaccine (Penta1), and the percentage who receive measles vaccine, are commonly used EPI indicators for monitoring an immunization programme. Name two other EPI indicators and, in each case, explain why they are particularly useful.
Answer
The percentage of children in the target population who receive the third dose of pentavalent vaccine (Penta3) is particularly useful, because it indicates the continuity of use of the immunization service by parents and caregivers. A low dropout between Penta1 and Penta3 indicates that parents and caregivers are able to access the service.
The percentage of fully immunized children (FIC) is another particularly useful indicator, as it demonstrates the capability of the system to provide all the vaccines in the schedule at the appropriate times. It also gives an indication of the public demand for the service. Low dropout between Penta1 and measles immunization demonstrates satisfaction with the perceived quality of the service in the community, and also that there is not a general problem of utilisation of health services locally.
SAQ 10.3 (tests Learning Outcomes 10.1, 10.3 and 10.4)
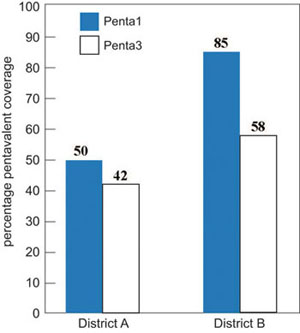
Figure 10.9 shows the percentage immunization coverage for Penta1 and Penta3 in two districts, labelled A and B. Based on the information in this figure, answer the following questions:
- a.Calculate the pentavalent dropout rate for the two districts A and B.
- b.Do the dropout rates suggest that access or utilisation is the major problem for the immunization service in each district? Explain how you reached your answer.
- c.What are the possible solutions for the problems in each district?
Answer
(a) Calculation of dropout rates.
District A:
Figure 10.10 shows that 50% of infants received pentavalent 1 vaccine, and 42% completed the three-dose schedule (using pentavalent 3 coverage as the indicator). The dropout rate is calculated using the equation:
Penta1 to Penta3 dropout rate = (Penta1 – Penta3) ÷ Penta1 x 100%
The dropout rate in District A is therefore (50 – 42) ÷ 50 x 100 % = 16%.
District B:
Figure 10.10 shows that 85% of infants received pentavalent 1 vaccine, but only 58% completed the three-dose schedule (received pentavalent 3). The dropout rate in District B is therefore:
(85 – 58) ÷ 85 x 100% = 32%.
(b) In District A, the major problem is low coverage, as only 50% of children received the first pentavalent dose, which indicates an access problem for parents or caregivers. In District B, the major problem is the high dropout rate of 32%, which indicates a general problem of utilisation of health services.
c) In District A, priority should be given to raising the pentavalent 1 coverage rate, by aiming to immunize the 50% of children who have never been reached by the immunization service. In District B, the priority should be given to following up on defaulters and persuading them to complete the schedule of immunization, so the pentavalent 3 coverage rate rises from 58% to closer to the 85% who received pentavalent 1.
SAQ 10.4 (tests Learning Outcomes 10.1, 10.3 and 10.4)
In a kebele with a total population of 5,000, an estimated 3.6% are surviving infants under 12 months old. In September, nine infants aged under one year and two children aged between 12 and 23 months old were immunized against measles.
- a.What was the measles immunization coverage rate for infants aged under one year in September? Is it lower or higher than the estimated total population of eligible infants in that month? (You can assume that approximately the same number of babies is born alive each month.) Show how you reached your answers.
- b.List some possible reasons for the measles immunization coverage rate in this kebele.
- c.What actions would you take to improve the coverage with measles vaccine?
Answer
- a.An estimated 3.6% of the population of 5,000 in the catchment area are under one year of age and therefore eligible for measles immunization. The total eligible population of infants in this age-group is calculated as follows: 5,000 x 0.036 (or 3.6%) = 180 infants You would expect about 15 of these infants to have been born each month of the year (180 ÷ 12 = 15). However, only nine infants received measles vaccine during September, so the measles vaccine coverage for September was (9 ÷ 15) x 100% or 60%.
- b.The measles immunization coverage rate of only 60% is low, and indicates a problem with utilisation of health services for parents or caregivers.
- c.Possible actions you could take to try to reach more infants in the target age group could include:
- more house-to-house visits in remote areas (using mobile teams)
- more outreach immunization sessions
- ensuring that no opportunities are missed to immunize eligible infants with measles vaccine, e.g. if they are brought to the Health Post for another reason, or when you are visiting the family
- more effective tracing of defaulters by checking entries in the EPI Registration Book every month, and using reminder cards to tell you which infants are due for their next immunization in which month.
SAQ 10.5 (tests Learning Outcomes 10.1 and 10.5)
Meseret completed the Summary Report of the immunization service delivered from her Health Post for the previous month. She carefully recorded the number of doses of vaccines and vitamin A supplements given to infants and women in her catchment area during the reporting period. There were no cases of vaccine-preventable diseases and no serious adverse events following any of the immunizations, so she left this part of the report form blank. She recorded the number of vaccine vials she used during the month and the number wasted. Then she sent the report form to her supervisor.
- a.What mistake did Meseret make when she entered her data in the Summary Report?
- b.What other types of data did she forget to include in the Summary Report?
Answer
- a.Meseret’s mistake was leaving the Summary Report blank where she should have recorded ‘zero’ for cases of vaccine-preventable diseases and any serious adverse events following immunization.
- b.Meseret’s Summary Report should also have included:
- the number of vaccine vials she received as new stock during the month
- any specific problems encountered during the reporting period, e.g. stock shortages, transportation problems, cold chain failures, etc.
Summary of Study Session 10