

3 Vaccination programme
The vaccination programme against COVID-19 in the UK started in January 2021, with priority given to older people and those with weak or suppressed immune systems. Over the following 6 months the programme worked down through the age groups and then paused in late Summer, as there was some debate about whether vaccination was necessary for school-age children. The programme was taken up again later in 2021 for the younger age groups, partly because a wave of COVID-19 infections had start to spread in the community from July 2021. Also by Autumn, the benefits of vaccination in children were becoming clearer – although COVID-19 is not usually a serious disease in children, preventing infection and disruption to their education was at least as important as protection against disease.
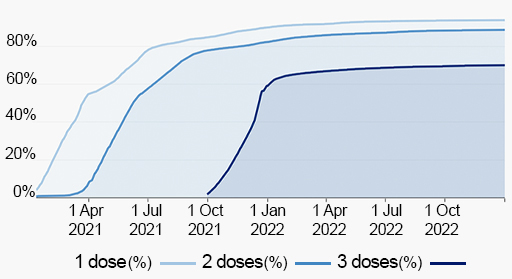
In the UK the Pfizer/Biontech mRNA vaccine and the Oxford/AstraZeneca vector vaccines were both used in the initial vaccination programme. Later the mRNA vaccine from Moderna was also used. All of the initial vaccination schedules required two doses of vaccine spaced at an interval of 3-10 weeks. For booster doses, (3rd injection) which started in October 2021, only the mRNA vaccines were used. Hybrid vaccination – when a person is immunised with one type of vaccine and then boosted with another, was found to be just as effective as using the same vaccine throughout. The uptake of vaccination in the UK is shown in Figure 6.
It should be emphasized that the choice of vaccines to use, the prioritisation and scheduling of the programme was made pragmatically. In the early stages the supplies of vaccines were limited and the ability to deliver them in the community was dependent on the availability of suitably qualified staff who could carry out the immunisation procedure. In these conditions, decisions were taken to vaccinate those most vulnerable to severe disease, protect the health service from being overwhelmed and maximise benefit to the community, by reducing spread of infection.