

Background to FGM‑related mental health problems
Female genital mutilation (FGM) can cause significant lifelong emotional and psychological distress, particularly with Type 2 and Type 3 FGM (Abdalla and Galea, 2019). Trauma may arise from the mutilation itself, memories of the event, and the ongoing impact of painful debilitating physical complications. These experiences shape how survivors feel about their sense of self, bodies, relationships, and overall wellbeing.
The mental health impact of FGM
Survivors may experience:
- fear, shame, embarrassment, humiliation
- low self‑esteem, body image concerns
- helplessness, powerlessness, loss of control
- sleep problems
- difficulties with relationships and sexual intimacy
- anger or betrayal toward those involved
- loneliness and isolation
- anxiety, depression, phobias, suicidal thoughts
- post‑traumatic stress symptoms such as flashbacks, intrusive memories, hypervigilance, emotional numbing
- avoidance behaviours, including avoiding people, memories, medical settings, or using substances to cope.
How trauma emerges and re‑emerges
Mind UK (2026) describes trauma as a distressing event or series of events that overwhelms a person’s ability to cope. Trauma can occur at any age and may continue to affect someone for many years. It can take different forms, including childhood trauma, collective or generational trauma, racial trauma, and secondary trauma.
The trauma of FGM can shape how survivors think, feel, and respond to later experiences, creating ongoing patterns of distress, negative beliefs, and unhelpful coping behaviours. Shame and pain may resurface at different life stages, triggered by recalling the event, hearing others discuss FGM, encountering insensitive reactions, or during medical examinations, intimacy, menstruation, pregnancy, and childbirth. Some girls who were cut at a very young age may not remember it but later experience shock, grief, and a deep sense of violation when they learn what was done to them.
Trauma can also appear as moral distress or moral injury. This may affect some perpetrators who feel guilt or regret for carrying out, witnessing, or not preventing the FGM, including when done under strong cultural pressure. This can leave lasting feelings of responsibility and remorse.
Healthcare professionals may experience vicarious trauma when hearing survivors’ stories or witnessing the harm caused.
How depression, anxiety and trauma interact in FGM survivors
Depression (low mood) in FGM survivors often develops through the combined effects of trauma, physical complications, and social or cultural pressures. Trauma, anxiety and depression interact and reinforce one another.
The diagram below outlines the symptoms of depression.
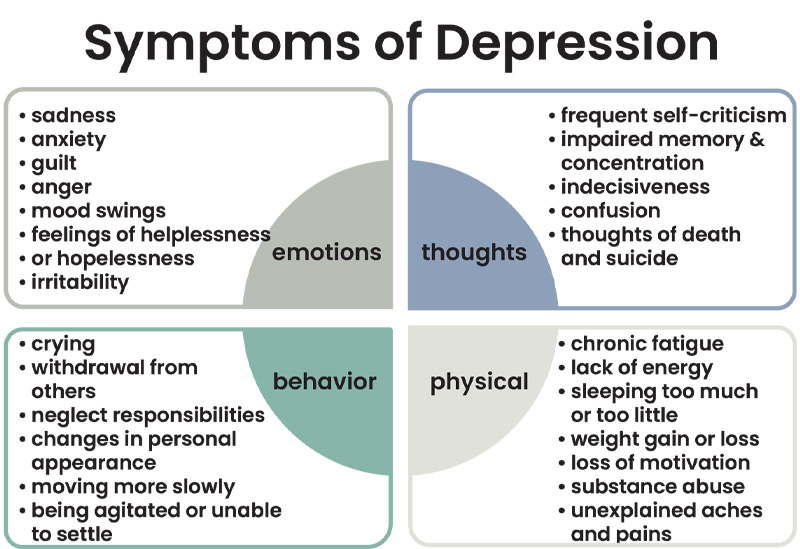
Anxiety is a common part of this cycle. Persistent worry can disrupt sleep, increase overthinking, and create a constant sense of being on edge. Even without real danger, the body may react as if threatened – raising the heart rate, quickening breathing, and remaining on high alert. Over time, this drains emotional reserves and contributes to low mood, withdrawal from relationships, and reduced confidence.
The diagram below outlines the vicious cycle of anxiety.
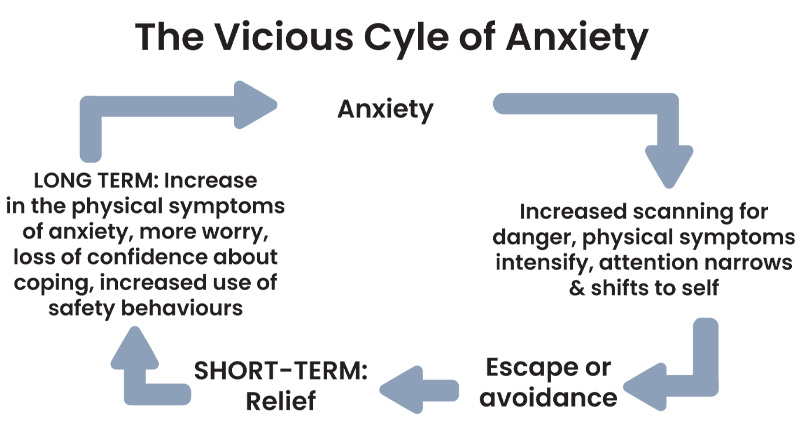
When the emotional or physical wounds of FGM are triggered, the body may respond as though the trauma is happening again. This can lead to cycles of fear, panic, hypervigilance and exhaustion. As survivors withdraw from family, friends, work, or social life to avoid distress, depression deepens, bringing sadness, shame, disconnection and hopelessness.
Depression then makes it harder to cope with anxiety and trauma symptoms. Low mood can reduce motivation to seek support or use coping strategies, reinforcing the trauma cycle and leaving survivors feeling stuck in patterns of fear, avoidance and emotional numbness. Without support, depression can become long‑lasting, and some people may turn to substances to cope, increasing isolation and health risks.
Understanding how trauma, anxiety and depression interact helps explain why survivors may struggle across many areas of life and highlights the importance of trauma‑informed, compassionate mental health care.
Cognitive Behavioural Therapy (CBT) can help
Cognitive Behavioural Therapy (CBT) is a structured talking therapy. The World Health Organization (2025) recommends CBT as part of a holistic, trauma‑informed plan to support FGM survivors with trauma, post‑traumatic stress disorder, depression and anxiety.
CBT helps survivors understand how their thoughts, emotions and physical reactions are connected to the trauma of their FGM and its ongoing consequences. It focuses on the distress a person is experiencing in the present and provides practical tools to manage these responses. It helps survivors to process and challenge unhelpful beliefs linked to the trauma, reduce avoidance, and build coping strategies to move forward and make daily life more manageable. It aims to strengthen a survivor’s sense of safety, control, confidence and emotional stability.
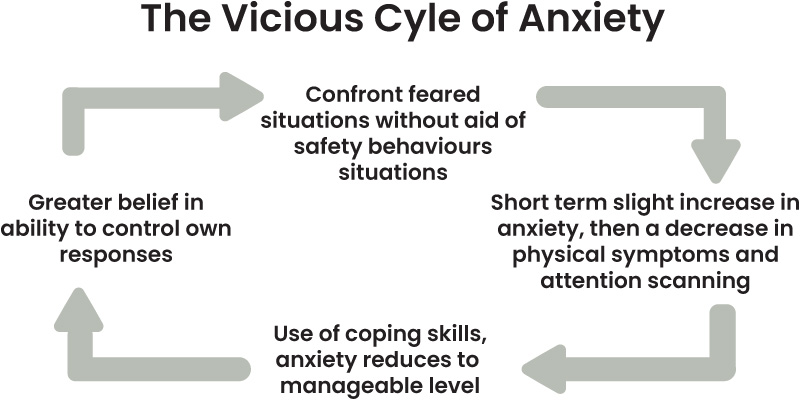
Other therapies, such as Eye Movement Desensitisation and Reprocessing (EMDR), may help survivors explore the origins of their trauma if they wish to do so. CBT differs in that it helps survivors notice unhelpful patterns and break the cycle by teaching practical ways to shift those patterns, manage anxious thoughts, and calm physical reactions. Techniques such as the ABC (Activating Event, Beliefs, Consequences) reframing approach and grounding exercises can help restore steadiness and a sense of control.
The diagram below outlines a model of reversing the vicious cycle of anxiety.
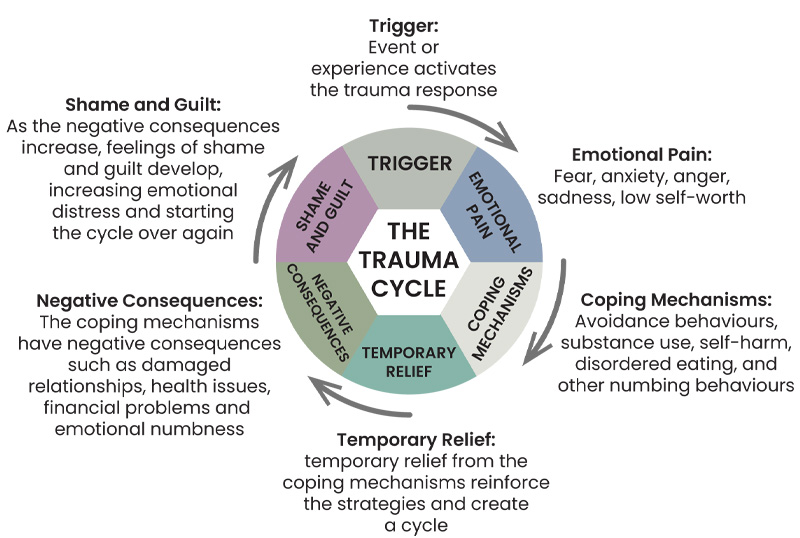
Edward’s Trauma Cycle (Edwards, 2024) can be a useful trauma‑informed tool within CBT. It can help practitioners understand how:
- unresolved FGM trauma continues to influence a survivor’s thoughts, emotions and behaviours
- patterns of fear, shame and avoidance can be triggered repeatedly throughout life
- the trauma cycle can be used to identify triggers, map links between thoughts, emotions, physical reactions, and behaviours, challenge unhelpful beliefs, develop coping strategies, and normalise trauma responses.
The diagram below outlines the Sally Edwards Trauma Cycle.
The Bottom Line
The World Health Organization (2025) calls for dedicated mental health support for FGM survivors, yet specialist services across the UK and Ireland remain limited and unevenly accessible. Examples of services include NHS National FGM Support Clinics, the Dahlia Project in London, and organisations such as the Irish Family Planning Association, AKiDwA, and Spirasi in Ireland.
To ensure consistent care, national mental health strategies across the UK and Ireland need to clearly outline how the emotional and psychological needs of FGM survivors will be met within mainstream provision. Survivors require trauma‑informed, sensitive, person‑centred support, including specialist psychotherapy and psychosexual therapy delivered by clinicians trained in FGM‑related trauma, particularly around gynaecological, obstetric and reconstructive procedures.
Mental health support and regular debriefing should also be available for healthcare professionals supporting FGM survivors, to help prevent vicarious trauma, reduce burnout, and maintain professional boundaries and wellbeing.
Try a related free course
-
Mental health in society
Learn more to access more details of Mental health in societyIn this free course, Mental health in society, you will explore and critically reflect on mental health. You will explore the relationship between the lived experiences of individuals, and the society and environment in which they live. Different perspectives, approaches and models of understanding and critiquing mental health will be explored ...

-
Exploring anxiety
Learn more to access more details of Exploring anxietyThis free advanced level course, Exploring anxiety, serves as an introduction to masters level study in neurosciences and mental health. Focusing on anxiety, you will consider key issues concerning diagnosis, causes and interventions. You will also learn how to evaluate news items, and to go behind the headlines and begin to explore some of the ...

-
Exploring depression
Learn more to access more details of Exploring depressionThis free advanced level course, Exploring depression, serves as an introduction to masters level study in neurosciences and mental health. Focusing on depression, you will consider key issues concerning diagnosis, causes and interventions. You will also begin to explore theoretical models, biological and psychological explanations, and look at ...

-
Exploring the relationship between anxiety and depression
Learn more to access more details of Exploring the relationship between anxiety and depressionThis free advanced level course, Exploring the relationship between anxiety and depression, serves as an introduction to masters level study in neurosciences and mental health. Focusing on anxiety and depression, you will consider key issues concerning diagnosis, causes and interventions, exploring how these conditions relate to each other. You ...

-
Supporting children's mental health and wellbeing
Learn more to access more details of Supporting children's mental health and wellbeingDo you have a professional or personal interest in the mental health issues affecting young children? Are you working with children or are you a parent or carer? This free course, Supporting children’s mental health and wellbeing, is designed to give insight into the factors that are contributing to our youngest citizens’ poor mental health; ...

-
Psychology around the world
Learn more to access more details of Psychology around the worldPsychology around the world looks at some of the ways people think in similar and different ways depending on where they live and their culture. The course starts with some general questions of how similar and different people’s psychology might be in different times and places. This is then followed with some key examples: how people perceive ...

FGM Collection
 This resource belongs to the FGM Collection on OpenLearn, designed for students and professionals in health, social care and related fields to support understanding, safeguarding practice, and compassionate, person-centred care.
This resource belongs to the FGM Collection on OpenLearn, designed for students and professionals in health, social care and related fields to support understanding, safeguarding practice, and compassionate, person-centred care.
Rate and Review
Rate this article
Review this article
Log into OpenLearn to leave reviews and join in the conversation.
Article reviews